
Abstract
Background:
Patients who request but do not receive postpartum permanent contraception (PC) are at high risk of subsequent short-interval pregnancy.
Objective:
To describe contemporary subsequent pregnancy rates in patients requesting but not receiving postpartum PC.
Design:
Single-site retrospective cohort study using medical record data of 2720 patients, 388 of whom presented for delivery with a signed Medicaid sterilization form.
Methods:
Reproductive outcomes of patients with unfulfilled postpartum PC requests (n = 234) were compared to a comparison group (n = 246) who did not request postpartum PC using descriptive statistics and multivariate logistic regression.
Results:
The overall PC completion rate was 39.7%. Among those with unfulfilled requests, 15.0% had a subsequent pregnancy within 18 months, compared to 27.1% of the comparison group.
Conclusions:
The subsequent pregnancy rate following an unfulfilled postpartum PC request is lower than historic estimates; however procedure nonfulfillment remains high.
Plain language summary
This study describes the reproductive outcomes, including the incidence of short-interval pregnancy and postpartum contraceptive method choices, of patients who request but do not undergo a permanent contraception procedure (sterilization) during delivery hospitalization.
Introduction
Permanent contraception (PC) remains a popular contraceptive method, with an estimated 8% of individuals requesting the procedure postpartum. 1 In recognition, the American College of Obstetricians and Gynecologists states “making postpartum sterilization readily available for all people is critical to providing adequate care.” 2 However, several clinical, hospital, and systems-level barriers to fulfillment exist. At the clinical level, patient characteristics including medical comorbidities and higher body mass index (BMI) are associated with lower PC fulfillment compared to those without comorbidities.3 –5 Difficulty with staffing and scheduling and limited operating room availability are known hospital-level barriers to fulfillment of PC requests following vaginal delivery.4 –6 At the systems-level, the U.S. Medicaid sterilization policy, which requires Medicaid recipients to sign a consent form and endure a 30-day waiting period prior to undergoing the procedure, is a well-known barrier to fulfillment compared to those with private insurance. 1 Recent data suggests that only 53% of patients with Medicaid who request postpartum PC achieve fulfillment before delivery hospitalization discharge compared with over 70% of privately insured patients. 1
Nonfulfillment of postpartum PC is associated with high short-interval pregnancy rates, loss of autonomous choice, and increased healthcare costs.7,8 Prior research has described twice the subsequent pregnancy rate within 12 months among patients who requested but did not receive postpartum PC compared to patients who did not request PC during the index pregnancy. 7 However, given the increased prevalence of long-acting reversible contraception (LARC) and changes in postpartum care recommendations, contemporary estimates are needed. 9 The overall objective of this investigation was to describe the reproductive outcomes, including subsequent pregnancy and contraceptive uptake, of patients with Medicaid insurance who requested but did not undergo a postpartum PC procedure and compare those findings to a group of patients who did not request the procedure.
Methods
This is a single-site retrospective cohort study utilizing available data in the electronic medical record. The study population included pregnant persons with Medicaid who received prenatal care at hospital-affiliated obstetrics and gynecology clinics and delivered at a tertiary care hospital in Buffalo, New York, between January 1, 2019, and December 31, 2021. The presence of a Medicaid consent signed during the current pregnancy was used as a proxy for intent to have a PC procedure. Patients were eligible for inclusion if they were aged 21 or older, had a live birth, had Medicaid insurance, and received prenatal care at a hospital-affiliated OBGYN clinic. Patients with a subsequent delivery during the study period could be included more than once given pregnancy-specific factors can influence contraceptive decision-making and access. We excluded patients under age 21, who received care outside of the hospital-affiliated clinics, with non-Medicaid insurance, and those who had non-live births.
A sample size calculation was conducted. Using existing data published in the literature, we assumed a 45% incidence of subsequent pregnancy within 12 months among those who requested PC and 25% for those who did not. 7 Considering these assumptions, a sample size of 176 (88 in each arm) was needed (alpha = 0.05, beta = 0.2, power = 0.8). We abstracted demographic, clinical, and delivery information including fulfillment of postpartum PC, contraception method plan and uptake, and documentation of new pregnancy for all patients who signed a Medicaid sterilization consent during the index pregnancy. Similar data was abstracted for a comparison group, defined as those who met the same inclusion criteria but did not request postpartum PC. The comparison group was randomly selected in a 1:1 ratio.
Our primary outcome was subsequent pregnancy within 12 and 18 months of delivery. These time points were selected to allow for comparison to prior research. Additionally, short-interval pregnancy, defined as a subsequent pregnancy within 18 months of a prior live birth, is associated with increased perinatal morbidity including preterm birth and low birthweight; thus we were interested in identifying pregnancies at potentially increased risk of adverse perinatal outcomes. 10 Subsequent pregnancies were identified by documentation of either a positive pregnancy test, presentation for prenatal care, or a documented or self-reported miscarriage or abortion in the medical record. The secondary outcome was contraceptive uptake within 12 months postpartum. The contraceptive method uptake was a categorical variable (interval PC procedure, LARC, other (shot, pill, patch, condoms, or other method), declined method, and no method documented or missing data), and was observed when the method was both documented and prescribed or administered within 12 months of delivery.
Our primary exposure was request for postpartum PC via the presence of the signed Medicaid sterilization form. Given that presence of the signed Medicaid sterilization form was used as a proxy measure for patient’s desire for postpartum PC, we also abstracted reasons for nonfulfillment from the electronic medical record.
Statistical analysis
We conducted descriptive analyses, comparing those who had fulfilled and unfulfilled PC requests. We then analyzed the reproductive outcomes of patients with unfulfilled PC requests and compared these to the reproductive outcomes of the comparison group. Data were analyzed using chi-square tests, t-tests, and nonparametric tests. Multivariable logistic regression was used to model the association between subsequent pregnancy and PC nonfulfillment, with age and parity as covariates. These covariates were chosen a priori given the literature surrounding association with PC fulfillment. 11 A sensitivity analysis was conducted by excluding patients who had a documented reason for nonfulfillment as “patient decision” and delivered by a Cesarean section, with the rationale that a systems issue was unlikely to influence the decision-making of patients who delivered by Cesarean. Statistical analysis was performed in Stata v16. This study received ethical approval from the University at Buffalo IRB (approval #STUDY00006552). This is an IRB-approved retrospective study, all patient information was de-identified, and patient consent was not required. The reporting of this study conforms to the STROBE statement. 12
Results
Of the 2720 patients who received prenatal care at hospital-affiliated clinics and delivered within the study time frame, 1827 patients met inclusion criteria, 388 (14.3%) of whom presented with a signed Medicaid consent at time of delivery (Figure 1). The overall postpartum PC fulfillment rate prior to discharge was 39.7% throughout the entirety of the study period. However, prior to the start of the COVID-19 pandemic in March 2020, 46.3% of patients achieved fulfillment, while during the pandemic, 34.3% achieved fulfillment. Among patients who signed a Medicaid consent form, 50.0% of White non-Hispanic patients achieved fulfillment, compared to 38.0% of Black non-Hispanic patients and 36.7% of Hispanic patients.

Study cohort flowchart of patients who delivered at a Buffalo, New York hospital between 2019 and 2021.
There was no significant difference in median age, gravida, parity, or BMI between patients who had a PC procedure completed (n = 154) and those who did not (n = 234; Table 1). Among patients with unfulfilled PC requests, 71.8% had a vaginal delivery compared to 20.8% of those who achieved fulfillment (p < 0.001). Reasons for nonfulfillment are shown in Table 2. Most patients (54.7%) had no documented reason for nonfulfillment.
Demographic characteristics and reproductive outcomes of patients who requested a postpartum permanent contraception procedure and had the procedure completed, not completed, or who did not request the procedure (comparison group), and delivered at a Buffalo, New York, hospital between 2019 and 2021.

PC: permanent contraception; IQR: interquartile range; LARC: long acting reversible contraception; BMI: body mass index.
Asian, American Indian, and Pacific Islander were combined due to small numbers.
Defined by a documented positive pregnancy test, prenatal visit, or self-reported miscarriage or abortion.
Information on subsequent pregnancy in the setting of failed PC was not collected.
Contraceptive method plan as documented in the medical record at either hospital discharge or the postpartum visit, includes both already initiated and planned to initiate methods.
Contraceptive method uptake in year 1 was observed when the method was both documented and prescribed or administered during the first year. Methods prescribed at hospital discharge but not documented as being continued at the postpartum visit or during year 1 were not included.
Documented reasons for nonfulfillment of permanent contraception requests among patients who presented with a signed Medicaid consent form by mode of delivery.

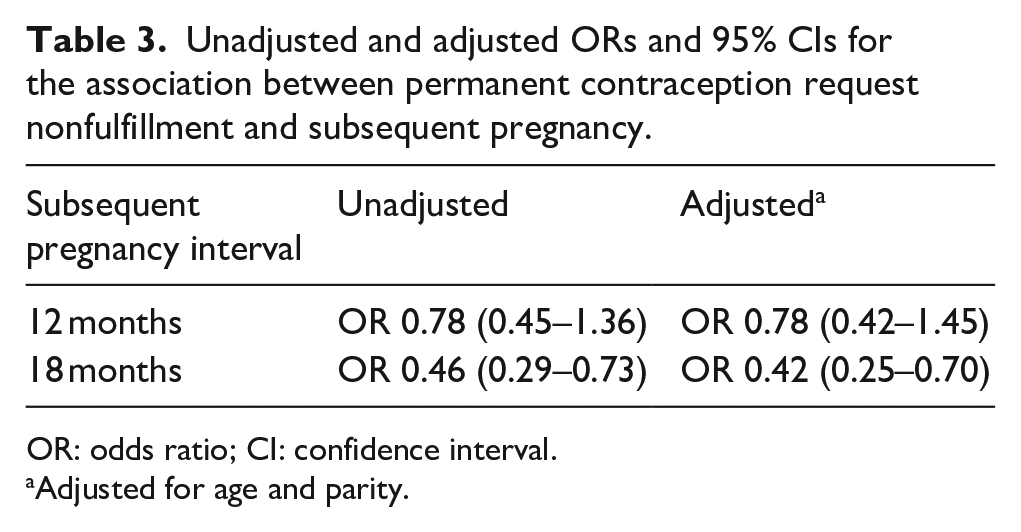
The reproductive outcomes of the 234 patients with unfulfilled PC requests were compared to 246 patients who did not request PC (Figure 1). Patients who requested PC were older (29 versus 26 years, p < 0.001) and had higher parity (4 versus 2 median births, p < 0.001; Table 1). The subsequent pregnancy rate among those with unfulfilled PC requests was 11.1% within 12 months and 15.0% within 18 months of delivery compared to 13.4% and 27.1%, respectively, among the comparison group (Table 3; 12 months: adjusted odds ratio (aOR) 0.78, 95% confidence interval (CI) 0.42–1.45; 18 months: aOR 0.42, 95% CI 0.25–0.70). Results of the sensitivity analysis, removing patients who underwent Cesarean section and whose documented reason for nonfulfillment was “patient decision,” demonstrated stability of the subsequent pregnancy estimates at 12 months and 18 months (12 months: aOR 0.72, 95% CI 0.38–1.37; 18 months: aOR 0.38, 95% CI 0.22–0.66).
Unadjusted and adjusted ORs and 95% CIs for the association between permanent contraception request nonfulfillment and subsequent pregnancy.
OR: odds ratio; CI: confidence interval.
Adjusted for age and parity.
At hospital discharge, 91 patients (38.9%) with unfulfilled requests had a documented plan for an interval PC procedure (Table 1). At the postpartum visit, 52 (22.2%) individuals planned a PC procedure, and 33 (14.1%) underwent a PC procedure within 12 months of delivery. Uptake of LARC by 12 months postpartum was similar between those who did and did not request PC (12.4% versus 13.7%). At 12 months postpartum, 50.4% of patients with unfulfilled PC requests had not initiated a contraceptive method or were lost to follow up, compared to 40.5% of the comparison group.
Discussion
Among patients in our study who presented for delivery with a signed Medicaid sterilization form, just 39.7% had a PC procedure completed during delivery hospitalization. The subsequent pregnancy rate among those with PC nonfulfillment was lower (11% at 12 months and 15% at 18 months) than what is described in older studies (47% at 12 months) 7 but aligns with newer estimates (6%–23% at 12 months, 23% at 18 months).1,4,13 In a comparison group of patients who did not request PC, the subsequent pregnancy rate ranged from 13.4% at 12 months to 27.1% at 18 months, consistent with prior work that found a subsequent pregnancy rate in this group of 22% within 12 months. 7 Notably, patients with PC nonfulfillment in our study were less likely than the comparison group to become pregnant again within 18 months which differs from prior research that showed the opposite trend. This finding may be explained by the difference in study population characteristics, particularly that patients in the study by Thurman and Janecek paid out of pocket for their PC procedures whereas the cost for our study population was covered by Medicaid. 7 Furthermore, increased access and coverage for LARC as an alternative contraceptive method in the setting of PC nonfulfillment could influence observed differences in contemporary subsequent pregnancy estimates. 9
Among patients with unfulfilled postpartum PC requests, less than 15% had an interval PC procedure completed within the year following delivery, while half had no documented contraception plan at 1 year postpartum. Possible explanations for these observations include known barriers faced by patients seeking postpartum and contraceptive care, including transportation challenges, lack of childcare and insurance, and competing priorities. 14 Alternatively, this may be attributed to contraceptive choice fluidity, the understanding that individual method preferences and goals change over time and with life circumstances.15,16 While subsequent pregnancy rates may be lower than historic estimates, a lack of contraception plan among those with previously documented undesired future fertility highlights considerations providers must undertake when counseling patients interested in PC, including setting realistic expectations and acknowledging known barriers for PC completion, and discussing alternative contraceptive methods in the setting of potential PC nonfulfillment. However, efforts must also be made at the institutional level to continue to reduce barriers to PC fulfillment and improve equitable access to the procedure.
Limitations
Our analysis was limited to information available in the electronic medical record. We used the presence of a signed Medicaid sterilization form in the patient’s record as a proxy for PC request as we felt this was a more reliable indicator of intent than documentation in a prenatal note at our institution, which was neither standardized nor consistent. With this approach, we recognize we cannot account for patients who ultimately changed their mind about undergoing the procedure prior to delivery. Reason for nonfulfillment was not routinely documented in the medical record and was unavailable in most cases. However, our sensitivity analysis which aimed to account for these limitations demonstrates stable results. While we did not match cases and controls on several demographic factors that may be associated with future reproductive goals (i.e., age, parity) and acknowledge this may influence estimates of reproductive outcomes observed in this study, these variables were included as covariates in our regression model.
Notably, the study period includes the years of the COVID-19 pandemic. In the early months of the pandemic, PC procedures following vaginal delivery were considered elective and paused at the study site, thus contributing to a lower overall completion rate. Additionally, because our clinics do not offer abortion services, it is possible patients sought pregnancy options, including termination and prenatal care, elsewhere, which may affect our estimates of the subsequent pregnancy rate.
In conclusion, we found subsequent pregnancy rates following postpartum PC nonfulfillment to be lower than historic estimates; however, lack of a postpartum contraceptive plan among the study population remains high. Equipping patients with the information and resources to achieve their desired contraceptive goals through shared decision-making and patient-centered contraceptive counseling is necessary to achieve higher patient satisfaction, greater autonomy, and overall improved reproductive health outcomes. Equitable access to PC necessitates ongoing efforts to reduce barriers to fulfillment, particularly in the postpartum period.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251356883 – Supplemental material for Reproductive outcomes of patients with unfulfilled postpartum permanent contraception requests
Supplemental material, sj-docx-1-whe-10.1177_17455057251356883 for Reproductive outcomes of patients with unfulfilled postpartum permanent contraception requests by Grace A. Trompeter, James Shelton, Kavita Shah Arora, Victoria Lazarov, Elliana Gianacopoulos and Rachelle St. Onge in Women’s Health
Footnotes
Acknowledgements
None.
Ethical considerations
This study received ethical approval from the University at Buffalo IRB (approval #STUDY00006552) on August 22, 2022.
Consent to participate
This is an IRB-approved retrospective study using chart review, all patient information was de-identified, and patient consent was not required. Patient data will not be shared with third parties.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Our regulatory approvals do not permit our data to be made publicly available. Researchers who are interested in viewing the data can contact the University at Buffalo Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.