
Abstract
Background:
There is an increasing emphasis on promoting women’s autonomy in reproductive decision-making, particularly given global efforts to increase contraceptive access and uptake. Scales to quantify autonomy have inconsistently included the effect of external influences and focused primarily on influences of partners.
Objectives:
This study aimed to gain greater depth in understanding how influences including and beyond a woman’s partner affect her contraceptive decision-making, as well as how external influences can overlap and further complicate contraceptive decision-making.
Design:
A phenomenological, qualitative study in which in-depth interviews were conducted in three phases from May 2021 to February 2022 with women living in northwest Tanzania who had varying histories of contraceptive use or non-use.
Methods:
One-on-one, in-depth interviews were conducted in Swahili, the national language of Tanzania, by trained female interviewers. Interviews were digitally recorded, transcribed, translated into English, and independently coded by three investigators. Analysis was conducted using NVivo. The codes developed from the transcripts were grouped into overarching themes with supporting illustrative quotes.
Results:
A total of 72 women were interviewed. Partners were the most influential in women’s family planning decision-making, followed by friends, relatives, community religious leaders, and healthcare providers. Out of the 52 women with a partner who had ever used family planning, 76.9% had discussed their desire to use family planning with their partner and nearly all reported strong pressures to use or not to use family planning from partners, family, and friends. Rarely, participants stated that they were devoid of any influence.
Conclusion:
In rural Tanzania, women’s decision-making about family planning was highly impacted by external influences, including not only partners but also family, friends, and community. Indicators of women’s reproductive autonomy and measurements of interventions to promote contraceptive use should incorporate measures of these external influences.
Introduction
The past decade has seen a growing emphasis on gauging the success of family planning (FP) programs by examining women’s independence in planning when and how many children to have, rather than simply measuring the contraceptive prevalence rate. 1 This emphasis reflects the globally agreed-upon United Nations Sustainable Development Goals of achieving gender equality and empowering women and girls by 2030 (Sustainable Development Goals (SDG) 5), which includes a specific sub-aim of ensuring that women have the right to make decisions about their sexual and reproductive health (SRH). 2 Women’s autonomy in SRH decision-making can translate to improved access and utilization of SRH services including antenatal, perinatal, and postnatal care, FP, and gynecologic primary care. 3 Ultimately, improved SRH care can promote better economic outcomes, for example, by increasing opportunities for women to work outside the home, and improve health outcomes for both women and children by enabling birth spacing.3,4
Several groups over the past decade have constructed scales to quantify women’s autonomy in reproductive decision-making. A contraceptive autonomy indicator proposed in 2020 evaluates three subdomains of contraceptive autonomy: informed choice (adequate, unbiased knowledge about contraceptives), full choice (access to a variety of contraceptives), and free choice (voluntary desire to use contraceptives). This indicator allows the broad quantification of multiple important domains of contraceptive autonomy, 1 but does not evaluate or account for the impact of external influences in a woman’s decision to use or not to use contraceptives. A second scale, the reproductive autonomy scale, evaluates a woman’s autonomy in deciding on contraceptive use, pregnancy, and childbearing using three sub-scales: decision-making, freedom from coercion, and communication. Notably, this scale was developed in the United States and focuses on evaluating the influence of partners but does not account for multiple other interpersonal influences that may affect a woman’s informed and free choice. 5
External influences on an individual’s decision-making, including about personal health matters, are common in Tanzania and many other sub-Saharan African countries. Decision-making in such contexts is frequently dominated by men and influenced by social and environmental factors that can hinder women’s ability to make decisions independently.6,7 Multiple studies have suggested the strong impact that social, familial, cultural, and religious pressures can have in discouraging or encouraging the use of FP,8 –16 underscoring the importance of accounting for these influences when measuring contraceptive autonomy. However, the power of these multiple influences, and the overlap and interactions between them, have not been comprehensively incorporated in investigations of contraceptive autonomy. To address this gap, we conducted 72 in-depth interviews with women living in 5 communities in rural northwest Tanzania. Our goal was to gain greater depth in understanding how influences including and beyond a woman’s partner affect her contraceptive decision-making, as well as how external influences can overlap and further complicate decision-making.
Methods
Study design and setting
We employed a phenomenological, qualitative study in which we conducted in-depth interviews in three phases from May 2021 to February 2022 with women living in northwest Tanzania who had varying histories of contraceptive use or non-use. Based on our previous experience conducting interviews in Tanzania on FP, we understand that FP is often perceived as a private and sensitive subject in which people hold varying and sometimes opposing perceptions. Hence, in order to allow participants to freely discuss their experience and perceptions of FP, private in-depth interviews were conducted in Swahili, the national language of Tanzania. The consolidated criteria for reporting qualitative studies (COREQ), as outlined in Table 4, was used to ensure comprehensive reporting of the study methodology and findings. Interviews were conducted in the rural communities of Nyasenga, Ngoma B, Sima, Tunyenye, and Kasenyi. These five communities were purposively selected because they were part of an ongoing cluster randomized trial in which religious leaders were invited to attend an educational seminar about FP.
This trial involved 12 intervention communities, which received an educational intervention for Christian religious leaders about FP, and 12 control communities that received the intervention after completion of the trial. 17 The intervention was initially implemented among Christian religious leaders, based on our prior qualitative work that showed that there are belief-based perceptions about FP. This demonstrated the need to develop a curriculum that included specific teaching from the Bible or the Qur’an relevant to each group. 10 We recently developed and pilot-tested a similar intervention for Muslim communities. 18 In the intervention communities, all churches in that community were invited to send up to four official or lay leaders to attend an educational seminar in which theological, social, and medical aspects of FP were discussed. These seminars were co-taught by medical personnel (a nurse and/or doctor) and pastors or other senior Christian leaders with training in theology. Programmatic data on contraceptives dispensed from community health facilities was collected 1 year before and 1 year after the date of intervention initiation to quantify the difference in contraceptive uptake before and after the intervention. At the time of these interviews, the intervention communities had received the intervention for religious leaders 6–10 months previously, and the control communities had not yet received an intervention for its religious leaders.
Sampling and recruitment
In collaboration with a nurse at the primary health clinic in each community, the study team purposively sampled women to participate in in-depth interviews using the criterion sampling strategy, which used a pre-determined eligibility criteria based on their categorization into one of four contraceptive status groups based on the use of modern contraceptives that were locally available free of charge at the health facility: current contraceptive user, past contraceptive user, recent contraceptive user, and contraceptive non-user. A current contraceptive user was defined as a woman who had used modern contraception for more than 1 year. A past contraceptive user was defined as a woman who had a history of using modern contraception but was not currently using any modern contraceptive method. A recent contraceptive user was defined as a woman who started using modern contraception less than 1 year previously. A contraceptive non-user was defined as a woman who had never used modern contraception or had only used traditional or non-medical contraceptive methods, that is, calendar method. Interviews ranged from 30 min to 1 h. General topics discussed in the interviews for contraceptive non-users and users are outlined in Tables 1 and 2.
Main topics included in the interview guide for contraceptive users.

Main topics included in the interview guide for contraceptive (current) non-users.

The in-depth interviews were conducted in three iterative phases. After conducting the Phase 1 interviews, transcripts were coded by study team members and evaluated in a collaborative group process to revise and clarify the interview guide. This revised interview guide was used by interviewers conducting the Phase 2 interviews and again revised during subsequent coding by the study team and interviewers to further enrich data. Following each round of interviews, the team of interviewers discussed findings and noted down initial reactions. These discussions, in conjunction with the ongoing analysis of transcripts after each phase of interviews, allowed us to assess whether data saturation had been achieved. Upon reviewing the Phase 2 interviews, it became evident that, because the majority of participants resided in the intervention communities and were identified as FP current or past users, we had not sufficiently captured the experiences of non-users. This led to the design of an additional interview guide for non-users of FP, which was then used in the Phase 3 interviews. Phase 3 interviews were conducted in one intervention community and one control community to capture diverse perceptions that might exist in communities not included in the intervention arm of the cluster randomized trial. Interviews were conducted among different participants throughout this study, with no repeat interviews. Table 3 shows the sampling criteria of each interview phase, including dates and number of interviews conducted in each phase.
Three-phase sampling method and sequentially enrolled study participants.

Data collection and sample size
Each in-depth interview was conducted by one trained female interviewer face-to-face. Interviews were conducted in Swahili in a private and quiet area near the community’s health facility. The open-ended questions were designed to assess knowledge of FP, community discussions about FP, perceptions of FP, FP discussions within close relationships, and reasons that participants use or do not use FP. We aimed to understand how other people in a woman’s life (including partners, relatives, friends, medical personnel, and influential community members) impacted her decision to use or not to use FP. We pre-specified that we would investigate the influence of religious leaders given the design of the larger cluster randomized trial.
Data processing and analysis
Interviews were digitally recorded, transcribed verbatim, and translated into English after each interview phase by experienced research assistants. All interviews were independently coded by at least two investigators on the study team. Interview transcripts were not returned to participants for comment and/or correction. Following each phase of interviews, investigators independently developed an initial list of codes after coding three interviews and then shared codes via a group process to agree on consensus codes. Additional in vivo codes identified during subsequent coding were discussed for potential inclusion. After each phase, codes and overarching themes were discussed by study team members in a collaborative group process. Finally, the codes were grouped into overarching themes with supporting illustrative quotes presented.
Quantitative sociodemographic data were summarized using medians [interquartile ranges] and number (percent) using Stata/IC Version 17 (College Station, Texas).
Reflexivity statement
The authors have varying levels of experience conducting qualitative research in rural Tanzania. V.J.L., A.N., L.M., N.K., and S.B. hold bachelor’s degrees. A.S. holds a master’s degree. S.E.K. holds MD and MMED degrees. A.H.M. holds a DIS degree and J.A.D. holds a MD/PhD degree. V.J.L., A.N., A.H.M., and J.A.D. are very familiar with this community through prior research activities and were involved in participant recruitment. V.J.L., A.S., A.N., L.M., and N.K. are fluent speakers of Swahili and natives of Tanzania. They interviewed participants, worked together to revise interview guides after each phase, and contributed to the creation of the first version of the code book. The first version of the code book was created by V.J.L. and A.S. after coding three interviews each. Upon the creation of the first version of the code book, it was shared with all the study team who conducted the interviews for feedback, further revisions, and finalization. New codes were discussed as they emerged and added once agreed upon. After all transcripts were coded, codes were grouped into larger categories from which themes were developed, with divergent perceptions flagged. V.J.L. and A.S. created the final version of the code book and independently coded all interviews via NVivo. S.B. coded the first phase of interviews via NVivo and contributed to the revision of the interview guide after the first phase of interviews. A.H.M. and J.A.D. have extensive experience conducting qualitative research in this community and are co-leading the cluster randomized trial in which this study was nested. They served as advisors throughout this qualitative study, together with S.E.K. J.A.D. contributed to the revision of the interview guide and analysis of the interviews. V.J.L. and J.A.D. wrote the first version of the manuscript, which was reviewed and revised by all nine authors. At the time of the study, V.J.L., A.S., A.N., L.M., and N.K. worked as research assistants at differing public/global health institutions. S.B. was a medical student at Weill Cornell Medicine. S.E.K. was professor of internal medicine at Weill Bugando School of Medicine. A.H.M. was the principal of Mwanza Christian College and J.A.D. was an associate professor of medicine at Weill Cornell Medical College. V.J.L., A.S., A.N., L.M., N.K., S.B., and J.A.D. identify as female. S.E.K. and A.H.M. identify as male. Consent to publish these findings was given by all contributing authors.
Results
Demographic characteristics
Among the 72 women included, the median age was 29.5 years, with 72.2% of the women being married and having a median number of four living children (Table 4). Participants had attended a median of 7 years of school. 94.4% of the women reported either Christian or Muslim religious affiliations, with 88.9% being Christian and 5.6% being Muslim. Among participants, 69.4% were current contraceptive users and 19.4% had never used contraception. Overall, no one who was approached for an interview refused to participate.
Demographic characteristics of 72 women who participated in in-depth interviews.
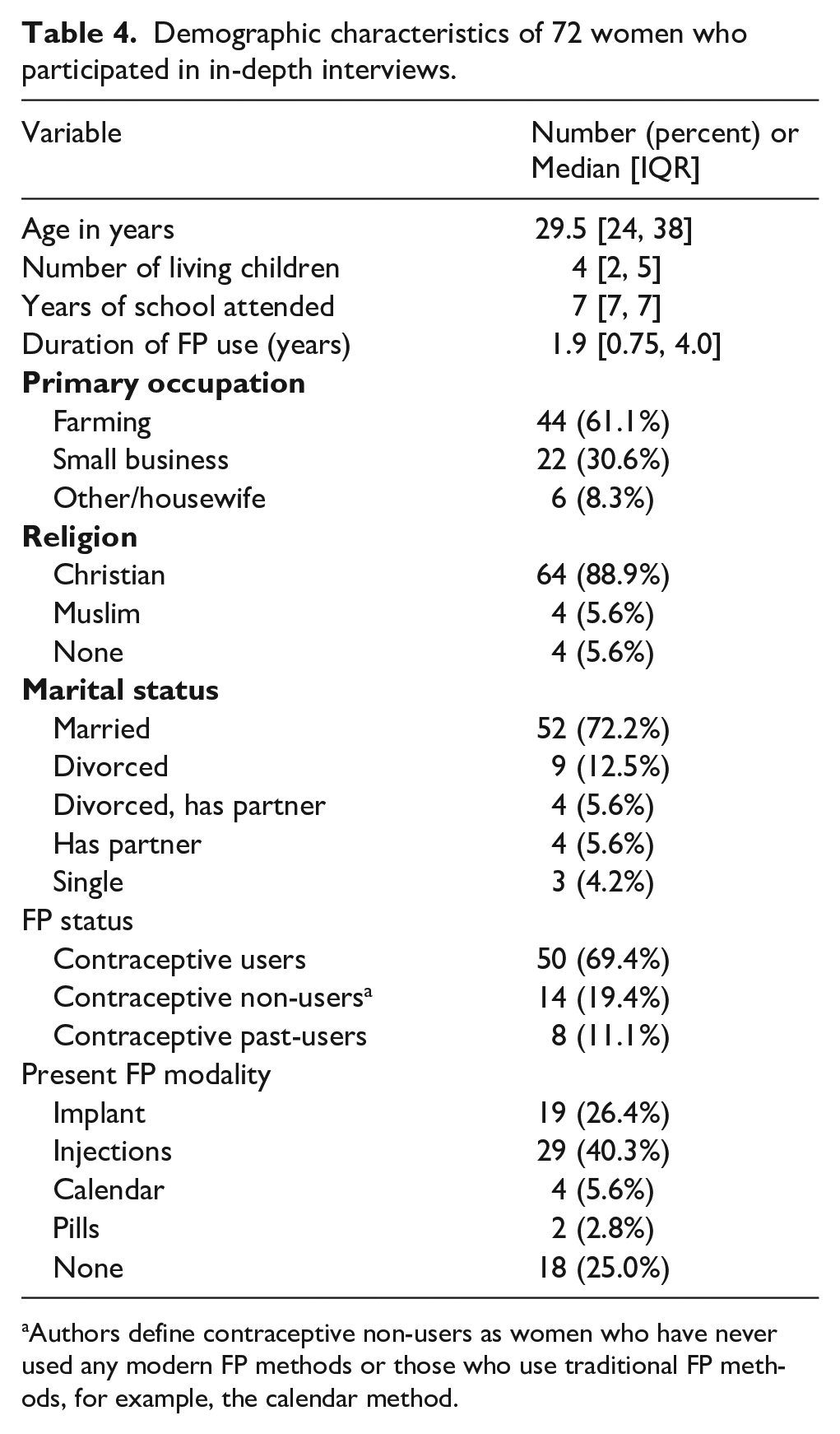
Authors define contraceptive non-users as women who have never used any modern FP methods or those who use traditional FP methods, for example, the calendar method.
Analysis
The socio-ecological model was used to evaluate and categorize the multiple factors that impact women’s contraceptive autonomy and decision-making. These are summarized briefly here, depicted in Figure 1, and discussed in greater depth below. Overall, on the intrapersonal level, we identified factors that a woman assimilates that ultimately contribute to her decision about contraception, including knowledge about contraception, assessment of risks and benefits, and her religious beliefs in relation to contraception (e.g. a woman’s interpretation of how contraceptive use relates to her religious beliefs).

Socio-ecological model depicting interpersonal and community-level influences that affect a woman’s use of contraception.
As shown in the model, women’s ultimate decision-making is enfolded by external influences at both the interpersonal and community levels. We defined the interpersonal level as close relationships that may affect contraceptive decision-making, and the community level as more distant relationships with influential community members that may affect decision-making. A majority of participants stated that, after encountering many influences, they ultimately make the final decision about using or not using contraception. However, we found that it was rare that this final decision, whether or not she would use contraception, was made completely independently, at the intrapersonal level only. Rather, most women’s final decisions were highly subject to complex interpersonal and community-level influences. We found that both intrapersonal level and external (interpersonal and community level) influences greatly impacted a woman’s decision to use or not to use contraception. For the purpose of this article, we will only focus on the external influences that are categorized in the interpersonal and community level (Figure 1), and consequently describe the power of these multiple external influences on the final decision that women make regarding whether to use or not to use FP.
Interpersonal level influences
A majority of participants stated that the most powerful external influences that either positively or negatively impact their contraceptive decision-making occur in close relationships. The relationships described to be the most influential were those with intimate partners, trusted friends, and relatives.
Male partners’ perception of contraception can strongly influence women’s contraceptive decision-making
Intimate partners wielded high influence on women’s contraceptive decision-making. Analysis showed that out of the 52 women who have a partner and have ever used contraception (current, recent, and past users), 76.9% had discussed their desire to use contraception with their partners (Table 5).
Characteristics of discussions about family planning between participants and their partners.
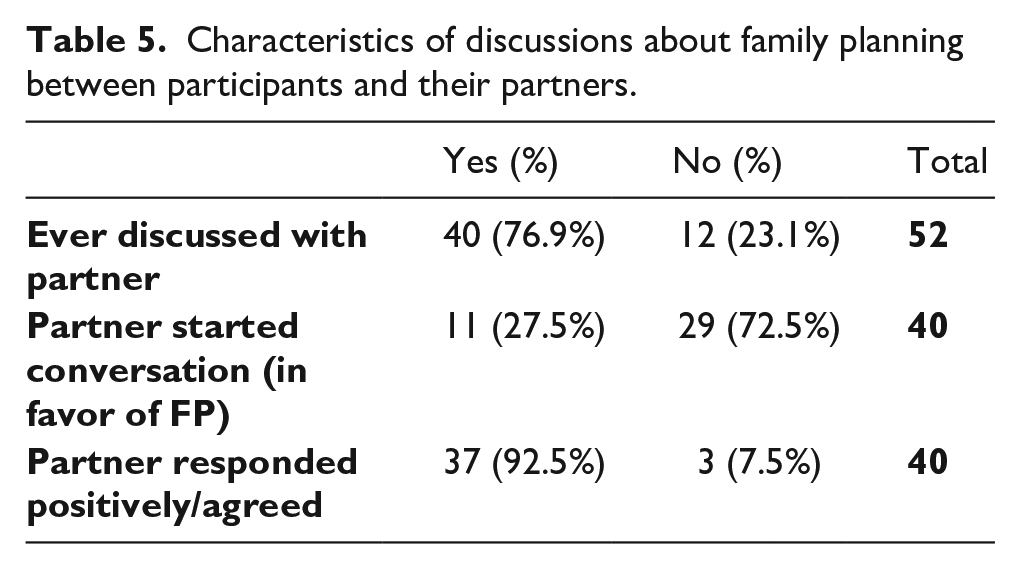
Among these 40 participants who had discussed FP with their partners, 92.5% described responses from their partners that were positive and supportive (Table 5). Examples of the types of reports from these participants included statements such as “the two of us, me and my husband, made the decision [to use FP]” (Contraceptive user, Christian, Intervention community) and “he is happy about FP because it gives a woman time to rest” (Contraceptive user, Christian, Intervention community). One participant reported that her husband not only agreed for her to use contraception but also went with her to the clinic for her first consultation: “He received the matter well, and we went together to the health center” (Contraceptive user, Christian, Intervention community). These quotes exemplify the openness of some men to discuss FP, prompting mutual decision-making with their partners. Another expressed her husband’s like-mindedness: “I think he thinks just like me that we should use FP and have children at the right time” (Contraceptive user, Christian, Control community). Overall, many participants reported that they “felt good because it’s [FP] a useful thing” (Contraceptive user, Christian, Intervention community) when their partners agreed, advised them, or initiated the conversation about FP.
Interestingly, approximately one-fourth of the participants who had discussed FP with partners reported that their partners were the ones who broached the topic and/or advised them to start using FP (Table 5). One woman explained, for example:
My husband started [the conversation] . . . he told me, my wife, we have to use FP . . . so that we too can stop giving birth in short intervals. Let us work first while we have stopped having children by using FP, and I told him that that is a good idea. (Contraceptive user, Christian, Intervention community)
In some of these cases, men were not only sources of support for women but also sources of knowledge:
My husband [is the one who influenced me to start using FP] . . . because I give birth with no space in between . . . I did not know [about FP before talking to him] . . . Yes, [he is the one that taught me about FP]. (Contraceptive user, not religious, Intervention community)
In situations in which men started the discussion about FP, women described feeling more open to use FP and engaging in the conversation freely. One contraceptive user reported, “I said it is good that you are the one who started that conversation. Because if I had started that conversation, you could have even scolded me” (Christian, Intervention community).
Another woman echoed this sentiment by describing her reaction to her partner advising her on starting to use FP:
I felt at peace because I did not expect him to ever advise me about that [FP] because it is very hard for men to agree to use family planning. When you tell him [a man] about family planning, he will say that you don’t want to give birth. So, I was happy because I felt that he understands that we have to use family planning now so that the child can grow properly. (Contraceptive user, Muslim, Control community)
In contrast, approximately 8% of participants who had FP discussions with their partners expressed that their partners did not support FP use (Table 5), frequently because of their misconceptions or negative views of FP and women who use FP. One woman explained that “he just doesn’t like to hear about FP . . . He is afraid that after using FP you can’t get a child again” (Contraceptive user, Christian, Intervention community). Another described men’s suspicion of women who use contraceptives, explaining that “they [men] believe that when a woman uses FP, a large percentage of them want to have affairs . . . so if you don’t get pregnant how would he know that you have cheated?” (Contraceptive non-user, Muslim, Intervention community).
In some instances, men’s negative perceptions of FP resulted in women deciding not to use FP despite their desire to do so:
I would have loved to use FP, but he [husband] refused. He said that if I do [use FP], I should leave his house and go use it at home [her parent’s house] . . . I felt bad . . . because I am the one who conceives, gives birth and raises the child. (Contraceptive non-user, not religious, Control community)
Furthermore, some women who were currently using contraception admitted that “Eee [yes], I would stop” using a contraceptive if their partners did not support its use (Contraceptive user, Christian, Intervention community).
Notably, participants reported that these negative views could sometimes be transformed after multiple discussions about FP, resulting in men agreeing and supporting their partners to use FP: “I was just telling him and he was refusing. When I gave birth to this [my youngest] child is when I told him again and he accepted” (Contraceptive user, Christian, Intervention community).
In other instances, women decided to not have FP discussions with their partners based on their partner’s known negative attitude toward FP. These women were among the one-fifth of participants who reported not discussing FP with their partners (Table 5). Other times, women reported using contraception without their partner’s knowledge and in spite of his disapproval. However, this was not an easy decision for women facing such strong oppositional influence:
I told him that I want to use FP. But he told me not to use it. I stayed for a long time [before starting to use FP]. I took like months . . . like seven months . . . I told him [when I was going to start FP] and he refused again . . . because he wanted children. No [he doesn’t know until now that I use FP] . . . he hasn’t asked [for another child] but I know he will ask. [and when he does ask] I will say that I am no longer fertile. (Contraceptive user, Christian, Intervention community)
Another described postponing the discussion about FP for months despite intending to broach the topic:
Right now he lives on his own so I can’t consult him [because] he will not accept [to use FP]. That’s why I just decided on my own. For now, I will tell him maybe in January . . . I just decided that I should tell him then [in January] because in the month of January I will be going back to get an injection [Depo-Provera], so if he agrees I will tell him but if he disagrees, I will just come on my own. (Contraceptive user, Christian, Intervention community)
In contrast, women with short-term partners frequently did not discuss FP with them, even if they were current users of FP, nor feel the need to do so, because “he is not my husband, he is just a lover. I am alone, and I live with my children” (Contraceptive user, Christian, Intervention community).
In principle, most women agreed that involving partners in FP decision-making was best for three key reasons. First, many felt ideologically that the decision to use FP should be made mutually by a woman and her partner. A contraceptive non-user explained her view “that FP is the agreement of a husband and wife on how long will they stay until they add another child” (Christian, Intervention community).
Second, women felt that informed partners can support women who experience side effects from contraceptive use. A woman who was not using contraception explained that involving the partner “is an important thing because if you don’t involve him there comes a time some issues arise as I told you before” (Muslim, Intervention community). Another woman similarly endorsed telling partners about FP use out of fear of potential negative consequences later:
It would be a nice thing to tell your husband because sometimes in using FP, you may end up facing some negative side effects . . . Some men may become mad at you and let you fight the consequences on your own. (Contraceptive user, Christian, Control community)
Third, women supported discussing FP with partners because men can threaten to separate from partners whom they learn were surreptitiously using FP. One contraceptive user described her fears:
He can know about it and asks you if he told you to go and put FP? [and then tell you to] go right now and remove that FP or leave my house. Go to your parents’ house so that I can look for the ones who can give birth. (Christian, Control community)
Given these complex considerations and partners’ strong influence, many participants suggested that a woman should “secretly make the decision [to use FP] on her own” only if her partner isn’t supportive of her desire to use FP (Contraceptive user, Christian, Intervention village). Another explained her recommendations:
it is good to involve him so that he can also understand . . . some of them [men] don’t have the knowledge and so it is better to tell him and get to know if he supports or doesn’t. If he doesn’t, then you will have to go by yourself. (Contraceptive user, Christian, Intervention community)
Female friends can highly influence FP decision-making
After partners, female friends were frequently mentioned as another source of influence in FP decision-making. Friends often advised and emboldened other women to use FP. One participant’s friend “told me that you are just giving birth all the time. It is not good, use FP. I agreed and started using it” (Contraceptive user, Christian, Intervention community). The participant further expressed that after receiving this advice, “I felt good and I have loved it [FP]. I will never stop using it [FP].” Another participant also reported that her friends “advised me to use FP and told me that FP is good and that I too should use it. [They advised me] to encourage my husband so that I can use FP” (Contraceptive user, Christian, Control community).
Additionally, participants stated that friends can also influence their choice of contraceptive method. One participant relayed that
when I got pregnant, I told her [friend] that my children do not have an interval. Before this little one reaches a year, I am pregnant again. And she told me, you should do what I do. The injection method is good. (Contraceptive user, Christian, Intervention community)
This participant decided to take her friend’s advice “because this is my close friend and she has told me about her experience [using Depo-Provera], so I also went with [Depo-Provera].” Another participant reported that she decided to obtain an implant because her friend who uses an implant told her that “it’s better than other methods” (Contraceptive user, Christian, Control community).
In contrast, other participants experienced being pushed not to use FP by friends. One participant, having decided to start using FP, was discouraged after a friend informed her that “some people don’t get pregnant again if they use FP . . . you will never give birth” (Contraceptive user, Christian, Intervention community). This participant withstood her friend’s influence by telling her friend that “those beliefs are the ones misleading you all, and then you find yourself giving birth often because of not using FP.”
Finally, participants reported that they also advise their friends to use FP. One woman described confidently advising her friend based on her own experiences after the friend experienced side effects while using an implant: “I told her to use Depo Provera because I have been using it and I have never faced any challenges” (Contraceptive user, Christian, Intervention community). Another counseled her friend not only about FP use but about managing her husband’s beliefs:
When I advised her, she said that she will go to talk to her husband. I asked her whether her husband is an understanding person or not and she said her husband is not understanding at all. So I told her that she should first make the decision on her own because men these days love having a lot of children. Then I told her to go to a health center for better advice about FP. (Contraceptive user, Christian, Intervention community)
Furthermore, some women described being so committed to supporting a friend in starting FP that they volunteered their own time to help:
She went and talked to her husband, and he agreed. She then came and I brought her here [dispensary] and they inserted an implant in her. Until now she has just those four children. (Contraceptive user, Christian, Intervention community)
Parents or relatives can support or discourage FP use
The third type of influential close relationships described were those with parents and/or other relatives. Many participants reported that their parents had been supportive of their desire to use FP, often citing reasons such as the expense of raising children, participant’s marital status (single/unmarried), or prior complicated pregnancies the participant had experienced:
My mum told me that because I don’t have a husband currently, I am supposed to use family planning. [Then] you will be able to continue farming in order to support your children. (Contraceptive user, Christian, Intervention community) I talked to my parents and they advised me to go and get it [FP] placed. [They said] you see the problems you faced during your first pregnancy and you had complications during your first delivery. You had to have an operation during your first pregnancy. (Contraceptive user, Christian, Intervention community)
Many described parents urging them to discuss FP with their partners, such as a woman whose mother agreed with her desire to use FP, advising that
it [using FP] is a good idea because life is getting harder [financially] lately. So long as you have agreed with your husband, then it is good and it will even help your children. You give your children time to grow while you look for money. (Contraceptive user, Christian, Intervention community)
Others described parents initially opposing their desire to use FP and how they defended their decision. A participant relayed that she had responded to her father’s concern about possible side effects by telling him “that we will see those challenges for ourselves and not rely on hearsay” and that more recently, “he is now thankful I used [FP] because he saw how I had close births” (Contraceptive user, Christian, Intervention community).
In addition to parents, female relatives such as sisters and sisters-in-law were reported to encourage participants to use FP. A sister advised one participant “to go and get the injection [Depo-Provera] so that I can raise my children” (Contraceptive user, Christian, Intervention community). Another sought the advice:
There is my sister in-law who was taking care of her children until they grow up a bit. So, I asked her and she told me that she is using an implant. She told me to go and put it instead of giving birth every year . . . when you put it [FP] you will rest. (Contraceptive user, Christian, Intervention community)
One participant, who had not yet used FP, explained how her sister had been encouraging her to start using FP in the near future by advising her “to rest by using FP since I already have five children” (Contraceptive non-user, Christian, Control community). The participant further reported that she is currently “waiting to get my period so that I may start [using FP].” This illustrates how these external influences are constantly at play, continuing to affect, and sometimes to change a woman’s initial decision to use or not use FP.
In contrast, a few participants reported opposition from female relatives. One participant explained that her sister, who had never used FP, argued against her desire to use FP by insisting that “FP destroys ovaries” (Contraceptive user, Christian, Control community). Another described having advised her own sister to stop using FP because
there was a time she was using the injection method and it caused her a problem. She was bleeding a lot. So I told her that she should stop using it . . . so, she decided to stop and didn’t use it again. (Contraceptive non-user, Christian, Intervention community)
Finally, similar to parents, female relatives sometimes urged participants to seek approval from their husbands before using FP. One participant, who had not yet used FP because of her ex-husband’s refusal to do so, described her sister urging her to not use FP without her husband’s approval: “I talked to my sister and said that I wanted to use FP but my husband is against the idea. She told me that there is nothing that I can do if my husband has refused.” The participant then challenged her sister’s stance by asking “should I just continue giving birth knowing that the man doesn’t even take good care of the children?” (Contraceptive non-user, not religious, Control community).
Community-level influences
Within the broader community, participants reported three major sources of influence that impacted both their perceptions of FP and the methods they choose: religious leaders, health professionals, and other women within the community, typically when those women shared their FP views in settings in which they are heard by others.
Religious leaders’ teaching on FP can influence women’s FP status
Participants frequently recalled situations in which religious leaders advised them to use FP. One participant stated that a religious leader told her “to go use FP freely and not have any doubts” (Contraceptive user, Christian, Intervention community). Another participant explained that religious leaders “say that we see a lot of women struggling but the [FP] services are now available in health centers” and that after hearing this, she “felt happy and she is using [FP] to date” (Contraceptive user, Christian, Intervention community).
The same participant also expressed that such teachings by pastors can encourage men to discuss about FP with their partners: “because even my neighbor came to tell me that her husband was happy [after the teaching] and asked her to start using it [FP].” Another participant recalled how a religious leader not only encouraged women to use FP but also encouraged men by saying “men, let us change. It is better if we use FP, and it is available in the hospital. Go and use FP, do not torture women.” This participant reported that her husband’s stance on FP was transformed after hearing the religious leader talk about FP in their church:
because there was a time, I hinted at him about FP and he refused saying it has a lot of effects. I told him to let go of those beliefs. So, on that day, in church is when I told him and he said it is true, it is better that we are able to use FP. (Contraceptive user, Christian, Intervention community)
Another participant described an occasion when she and some of her friends heard a pastor’s wife encourage women to use FP by saying:
Women, let us not be like the past [older generation] women. Yes, nowadays there is nothing like giving birth every time. Those are outdated things, and now there is education . . . My fellow women, it is important for us to use FP. It is nice and safe. I also use it. (Contraceptive user, Christian, Intervention community)
This participant explained that she and her friends were happy to hear from the pastor’s wife because they looked at her as an example and saw that “her children are doing well . . . there is a good interval [between them].” And so they “saw that what she was teaching was true.” She concluded by saying that “[the pastor’s wife] was one of the things that influenced me [to start using FP]. I went and thought about what she was telling us. [At that time] I hadn’t yet started [using FP].”
In stark contrast, others reported encountering religious leaders who opposed FP use and told them “to go and multiply.” While some described being discouraged by this preaching, others were able to reason against this influence. One participant asserted, “as a woman you have to be smarter. If you say you are filling the nation by yourself, it will never be filled.” She followed up this statement by saying that even if she heard a religious leader say FP is a sin, she would still choose to use FP due to practical challenges of having a large family: “Yes, it is a sin and we know that, but even God said that help yourself so that I can help you” (Contraceptive user, Christian, Control community).
A 33-year-old participant described an in-depth discussion about FP among religious leaders and community members that she overheard when she was 13 years old. This discussion started with the pastor stating that he opposed the use of FP from a biblical standpoint: “if you use FP, you are committing a sin since God said give birth and multiply.” This participant explained that this statement prompted multiple questions from the people present, with others opposing this view by saying that “we know that when you get FP, it is not an issue because you are not killing anything in comparison to abortion where you are now killing something.” The participant described how this statement elicited further discussion that ultimately led to the religious leaders concluding that “FP is not bad unless you get pregnant and abort it, that’s when you commit a sin” (Contraceptive past-user, Christian, Intervention community). However, this participant reported that despite overhearing this conversation, because of her age at the time, she couldn’t grasp the discussion and formulate her own perception regarding FP until she grew up and ultimately decided to use FP.
During the interview, participants who were currently using FP were asked how they would feel if they heard a religious leader opposing FP use. Multiple women admitted that they would grapple with their desire to use FP after hearing this opposition. For example, one contraceptive user said she would “feel bad [because] it is like he is opposing my decision to use FP” (Christian, Intervention community). Another said she would
feel bad because it is something that is mentioned and stated to be wrong in God’s eyes. But even if it is stated to be wrong by God, if you really want to use it [FP], you will still use it. (Contraceptive user, Christian, Intervention community)
Another participant echoed the above sentiment that she will feel bad if she heard a religious leader discourage FP use because “in this world, we need to use these things [FP] because there are a lot of challenges.” Despite not being an FP user, this participant understood the importance of using FP and consequently expressed her openness to using FP in the future if she receives adequate education about FP: “I have never been educated about it [FP], may be if you even explain about it [FP] to me right now I will also try to use it [FP]” (Contraceptive non-user, Muslim, Control community).
Others were able to maintain and defend their beliefs and perspectives such as a woman who explained that “he [the pastor] is a man and he is not struggling. Women are the ones who are struggling . . . FP helps us women a lot” (Contraceptive non-user, Christian, Intervention community). Another said she would be ready to challenge this position: “If he says that FP is bad, [I will ask] how is FP bad? Because you are protecting yourself so that you also get enough time to even contribute to the church. And get time to fulfill church tasks” (Contraceptive past-user, Christian, Intervention community). Others said they would challenge opposition to FP by thinking about their own understanding of their faith: “How is it a sin? I think it is just someone’s decision to use FP” (Contraceptive non-user, not religious, Control village). Another stated that “God has not said that we should use or not use FP” (Contraceptive user, Christian, Intervention community), and that this therefore provided her with freedom to decide about FP on her own. Finally, one woman asserted that she would be able to completely disregard such teaching from a religious leader:
if the religious leader will say that we shall give birth and multiply, will he be the one to take care of all my children? Will he even bring the offerings he gets to you so that you can take care of your family? . . . I can’t listen to him at all. (Contraceptive user, Christian, Intervention community)
Health professionals influence FP decision-making by providing both knowledge and individualized counseling
Many participants also reported that nurses or doctors could be highly influential in FP decisions. Women described receiving trusted medical information from these medical professionals. Others stated that hearing a brief FP education from local nurses while they were attending the clinic for other purposes had encouraged them to start using FP, explaining that “when I was coming to the clinic, the nurses were explaining about FP and that is why I decided to come [use FP]” (Contraceptive user, Christian, Intervention community). Another reported, “What helped me [decide to use FP] was the advice from the doctors that we should use FP so that our children can have good health and we can spend more time with them” (Contraceptive user, Christian, Intervention community).
Additionally, participants described how repeated discussions about FP at the clinic over time could be influential. One woman explained that during the first FP education from a nurse, “some of us were ignoring the teaching thinking that if you get injected you may get sick or get cancer.” However, after some time passed, they came “to the realization that we were overwhelmed and needed the service” (Contraceptive user, Christian, Intervention community). Another participant described the influence of repeated personal encouragement from nurses, who “advised me multiple times. They would advise me on FP. I initially refused the offer, but later saw that it was good advice, and hence I started using FP” (Contraceptive user, Christian, Intervention community). Another participant similarly expressed that a nurse “motivated me and that’s why I came [to start FP]” (Contraceptive user, Christian, Intervention community).
Stories shared among women in the community can negatively influence FP use
Participants reported that they often hear stories regarding women’s FP experiences, and that these stories can be highly influential. For example, a participant explained that she became “a little hesitant” to use FP because “you might be in a group, and you hear a woman say that she has a backache, and when you ask her why, she tells you that it’s because she went to put an implant” (Contraceptive non-user, Christian, Intervention village). Others reported hearing women discouraging others from using FP. Two contraceptive users described hearing women say that “FP has side effects [and] it’s better that I give birth until my eggs are finished [menopause]” and that “the implant disappears within the body” [an inaccurate statement] (Contraceptive users, Christians, Intervention communities). Another participant explained more generally that some women hear “that FP has negative effects, so [women who don’t use FP] don’t really understand why some of us use it” (Contraceptive user, Christian, Intervention community).
Some women reported that they resorted to using traditional FP methods such as the calendar method because of the negative side effects that other women had attributed to contraceptives: “I decided to use it [calendar method] because I see that it’s the only method that doesn’t have effects. From the way we see people talk about it, it’s a totally safe method more than the others” (Contraceptive non-user, Christian, Intervention community).
Effects of confluent influences on women’s ultimate decision-making
Taken together, these data indicate that participants frequently wrestled with a variety of external influences, oftentimes with multiple influences at once, when considering FP use. For example, a participant described hearing religious leaders state that FP is a sin because “FP goes and destroys eggs, and those eggs are your future children.” In response to this influence, she “thought about [what the pastor said] and didn’t see that it was okay [because] how will a woman give birth until all her eggs are finished?” She explained that this reflection led both her and her friends to decide collectively that even though “the pastor has said that it’s a sin . . . we won’t stop [using FP]” (Contraceptive user, Christian, Control community). This illustrates not only the pastor’s power to influence his congregation but also the tension between influences with which the woman had to wrestle before making a final decision regarding FP use. Ultimately, the community-level influence (pastor) was superseded by the interpersonal-level influence (friends) and by the woman’s own perception of FP.
Another participant stated that a year ago the pastor “told us about FP and that health providers were coming at the dispensary . . . he just announced and advised us to go and listen to them” However, despite this positive influence from the pastor, she didn’t go to the dispensary because “I was not allowed to go [by my husband].” However, after multiple attempts to convince her husband, he finally agreed:
I was just telling him and he was refusing, when I gave birth to this [eighth] child is when I told him again and he then accepted . . . On that day when I told him, he told me to just go [get FP]. (Contraceptive user, Christian, Intervention village)
In this scenario, the influence of the partner (interpersonal-level influence) was ultimately more powerful than the influence of the pastor (community-level influence).
Overall, these data show the strong external influences that women encounter, which can alter their decision to use or not to use FP. Interestingly, women were aware of the power that external influences have, and several described not telling those close to them about wanting to use FP out of fear of being dissuaded by these external negative influences. For example, one participant described why she didn’t involve her husband in her decision to use FP:
I did not tell him . . . I told him [before] that I am tired from having children and that we should use FP and he disagreed: [he said] I cannot live with a woman who can’t give birth. So, I said then let me just go [myself, secretly]. (Contraceptive user, Christian, Intervention community)
Another reported her rationale for not involving female friends or relatives in her decision to use FP:
No [I didn’t involve anyone in my decision to use FP] because you can involve someone and then she tells you not to go [use FP] because it has effects. You can also find that someone has used FP and it has caused her side effects. So, she will also tell you not to use it. (Contraceptive user, Christian, Intervention village)
Finally, a participant emphasized that she had to consciously choose not to listen to others in order to make the decision independently:
No [I didn’t involve anyone in my decision to use FP] because if I chose to listen to people, I possibly wouldn’t be using FP. So the decision [to use FP] was purely mine. (Contraceptive user, Christian, Intervention community)
Discussion
Our findings demonstrate the profound, complex, and largely underappreciated role that external influences—particularly those from partners, friends, relatives, community religious leaders, and health providers—have on a woman’s decision about the use of FP. These influences are persistent and strong, extending well beyond a woman’s initial decision to use or not to use FP and sometimes causing them to change their minds. We found that instances in which women decided to use FP devoid of influence were rare and quite often these women had specifically determined that they would not discuss FP with others out of fear of being influenced. These data draw attention to the critical importance of understanding how deeply these strong external influences affect FP use for the majority of women and, consequently, how efforts to equip women with knowledge and access to FP must reckon with, and ideally leverage, these influences to support women in their decision-making around FP.
Our findings build on a number of studies that have indicated that incorporating partners in decision-making about FP leads to healthy couple communication, decreases mistrust and covert contraceptive use, 19 and increases informed, sustained use of modern contraception. The CHARM intervention, which consisted of three FP and gender equity counseling sessions for men and couples in rural India, reported that women in the intervention group were more likely to report modern contraceptive use at 9- and 18-month follow-up in comparison to the control group. 20 Additionally, a study in Ethiopia showed that participants for whom both husband and wife participated in counseling groups were nearly twice as likely to have ever used FP and go to a health clinic together. 21 Finally, a study in Bangladesh reported lower rates of FP discontinuation in a husband-counseled group than control group. 22 These studies demonstrate the major influence that partners have on FP usage and discontinuation and highlight the importance of including male partners in FP interventions. Interestingly, to our knowledge, few to no interventions have intentionally incorporated friends or relatives. Our data suggest that incorporating others who are in women’s spheres of influence could be a novel and complementary approach to further promote uptake of FP.
Our work adds to the growing body of literature on the high impact of external influences in many African communities and more specifically demonstrates the potential of working with religious leaders to address public and reproductive health issues.23 –25 Most women described important influences, both positive and negative, and in both intervention and control villages – that their Christian or Muslim religious leaders had had on their and others’ decisions about FP. We have previously shown that education for religious leaders can impact not only the health perspectives of an individual but also the perspectives of others with high interpersonal influence including partners and friends. In the cluster randomized trial that included the communities in which this qualitative study was conducted, we observed 41% of those seeking FP in the intervention communities reported receiving FP information from a religious leader. 17 This underscores the impact of equipping Christian religious leaders with FP knowledge as it contributed to an overall increase in community awareness of FP. 17 Furthermore, our current qualitative data illustrate instances in which religious leaders’ teaching influenced both a woman herself and also her partner and friends. This simultaneous influence on both the interpersonal and community levels suggests that incorporating and addressing these external influences could be an innovative and effective way to affect health in these and other similar communities.
This study had strengths and limitations. We acknowledge that, as with any qualitative study, social desirability bias and participants’ perceptions of their obligate roles in society may have influenced their answers. Furthermore, the reported mostly positive perception of FP use among external influences (i.e. partners, religious leaders) could be attributed to the fact that 80.5% of our study participants were current or past users of FP, and that most resided in intervention communities where religious leaders received FP education. Consequently, this positive perception of FP within this study population may not accurately reflect the broader perception of FP in Tanzania. Nonetheless, we attempted to lessen this bias by using trained qualitative interviewers from outside the participants’ communities. In addition, our data were only collected from one region of Tanzania. However, the data are consistent across the five villages despite them being isolated from one another due to poor transport and infrastructure and spread over ~160 square miles. Therefore, we believe that these perceptions are reflective of many communities and are generalizable in Tanzania and beyond. Moreover, the relatively large sample size for qualitative data and our arrival at data saturation while coding suggest that even minority or rare views were represented in these data.
Conclusion
Overall, we provide compelling data on the multiple and complex influences experienced by women in rural Tanzanian communities when considering FP use. Our data suggest that indicators of women’s reproductive autonomy in this and similar communities must incorporate measures of these external influences, beginning with a woman’s partner and extending to account for her family, friends, and community. Among 72 women interviewed, those who made decisions about FP devoid of influence were rare. Furthermore, these women’s experiences speak volumes to the potential effectiveness of interventions that employ community, rather than individualistic, approaches to promote FP in this and similar settings. It is in using contextually informed measures and interventions that we will come closer to the global goal of empowering women to make their own decisions about their SRH.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241259173 – Supplemental material for “If I chose to listen to people, I possibly wouldn’t be using family planning”: Impact of external influences on women’s contraceptive autonomy in rural Northwest Tanzania
Supplemental material, sj-docx-1-whe-10.1177_17455057241259173 for “If I chose to listen to people, I possibly wouldn’t be using family planning”: Impact of external influences on women’s contraceptive autonomy in rural Northwest Tanzania by Valencia J Lambert, Anna Samson, Aneth Nzali, Lydia Mukasa, Neema Kachembeho, Sheridan Bowers, Samuel E Kalluvya, Agrey H Mwakisole and Jennifer A Downs in Women’s Health
Footnotes
Acknowledgements
We would like to thank the nurses at each dispensary for working with us to purposively sample women for this qualitative study and the women who participated in these interviews for openly sharing their views and experiences.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.