
Abstract
Background:
Menstruation is a universal and normal phenomenon during the reproductive age of females; adolescence is an essential period where females are preparing and adjusting themselves to manage their menstrual bleeding safely and cleanly. Menstrual hygiene management (MHM) is an issue that is insufficiently acknowledged and has not received adequate attention among visually impaired adolescent girls (VIAGs).
Objectives:
The purpose of this study was to determine the knowledge and practice of MHM and associated factors among VIAGs of selected institutions in Rwanda.
Design:
This study consisted of a cross-sectional study design using a quantitative approach.
Methods:
A cross-sectional study was conducted in April and May 2021 on 92 VIAGs. They were recruited from educational institutions in two Provinces in Rwanda. Voluntary participation and confidentiality were assured. Socioeconomic and demographic data, menstruation, and menstrual hygiene questionnaires were used to obtain the required information. Statistical Packages for the Social Sciences (SPSS) for Windows version 25 was used. Descriptive statistics, Chi-square test, and logistic regressions were used for data analysis.
Results:
The study reached 92 respondents. The majority of the respondents, 67.4% had a poor level of menstruation and menstrual hygiene knowledge while only 32.6% had a good level of menstruation and menstrual hygiene knowledge. Also, it is confirmed that the majority of respondents, 52.1% had a good level of practice, while 47.8% had a poor level of menstrual hygiene practice. The multivariable analysis revealed that factors associated with the menstrual hygiene practice were as follows: the mother’s education (odds ratio (OR): 5.979; 95% CI: [1.700–21.032]; p value: 0.005) and level of knowledge of menstruation and menstrual hygiene (OR: 0.132; 95% CI: [0.028–0.622]; p value: 0.010).
Conclusion:
The knowledge and practice of MHM among VIAGs were poor. Recommendations included the need for mothers to assist their daughters in improving learning and practice of menstrual hygiene, as well as the integration of MHM into school curricula. Further research is suggested to better understand MHM among Rwandan adolescent girls, both visually impaired and non-blind.
Background
Menstruation is a natural and normal event during the reproductive age of females, marking an important phase in adolescence as girls prepare themselves to manage their menstrual bleeding safely and hygienically.1–3 Globally, around 26% of the world population (52% of the female population) are of reproductive age, and over 800 million women aged between 15 and 49 are menstruating.4,5 Still most adolescent girls enter their puberty phase without preparing themselves due to poor information.1,6,7
According to the World Health Organization (WHO) and UNICEF’s Joint Monitoring Programme for drinking water, sanitation, and hygiene, menstrual hygiene management (MHM) is defined as the use of clean menstrual products to absorb or collect menstrual blood, with the ability to change these materials in a private setting as needed during the menstrual period. 2 This process includes washing the body with soap and water as necessary and having access to safe and convenient facilities for the disposal of used menstrual products. It also involves understanding the fundamental aspects of the menstrual cycle, enabling women and girls to manage it with dignity, without experiencing discomfort or fear.2,8,9
Unfortunately, around 10% of women worldwide are exposed to genital infections, with approximately 75% having a history of such infections, often due to pregnancy and poor genital hygiene.10–13 In low- and middle-income countries, more than half of women use homemade materials for menstrual management, with studies showing that many girls in Ethiopia, for example, did not use commercial products for menstrual hygiene and often isolated themselves during menstruation.13–15 Poor menstrual knowledge, limited access to absorbent materials, and inadequate facilities at school have been linked to increased absenteeism among girls.4,7
Studies conducted in Africa have determined that adolescent girls often lack appropriate knowledge and practices related to menstruation, with low usage of sanitary pads and reliance on cloth or toilet paper to manage menstrual blood.1,16–18 In fact, around 1 in 10 adolescent girls did not attend school during their menstrual periods, with some even dropping out of school at puberty due to misconceptions, cultural beliefs, and lack of access to sanitary materials and facilities.10,19–21
For visually impaired adolescent girls (VIAGs), maintaining proper menstrual hygiene is particularly challenging due to their disability, and they often require daily assistance in managing their activities.22,23 Menstruation is a critical aspect of their health, and effective management is essential to prevent infections related to poor hygiene.12,24–26 According to the WHO, 19 million children are visually impaired, with 1.4 million being irreversibly visually impaired, emphasizing the need for tailored interventions to support their personal and psychological development.12,18,24
In Rwanda, MHM remains an overlooked aspect of reproductive health. Many schools lack adequate facilities for MHM, with only 37% of primary schools having improved water sources, 52% improved sanitation, and 37% equipped with handwashing facilities with soap. 25
This study aims to address the pressing need to support VIAGs in managing their menstrual hygiene effectively. Despite considerable research on reproductive health and MHM among adolescent girls globally, there is a significant gap in studies focusing on VIAGs.27,28 Understanding their specific challenges, habits, and needs is crucial for developing tailored interventions. These girls, like their peers, wish to talk openly about their bodies and menstruation, replacing feelings of shame with confidence, pride, and dignity.19,29,30
However, due to their visual impairment, they face additional challenges in maintaining menstrual hygiene, which can lead to health complications, school absenteeism, and social isolation.11,12 This study, therefore, seeks to explore the knowledge, attitudes, and practices of MHM among VIAGs, addressing these gaps in research.
By examining the current knowledge and practices of MHM among VIAGs, the study aimed to provide valuable insights that will inform targeted strategies and interventions. It explored the factors influencing these practices and proposed recommendations to ensure that VIAGs receive the necessary support to maintain their health and dignity during menstruation. Expected outcomes include data-driven interventions that promote effective MHM, contributing to the overall physical, emotional, and educational well-being of VIAGs. These findings are vital in bridging the research gap and improving MHM practices, ultimately enabling VIAGs to lead healthier and more empowered lives.
Objectives of the study
General objective
The broad objective of this study was to determine the knowledge and practice of MHM and associated factors among VIAGs of selected institutions in Rwanda.
Specific objectives
The specific objectives of this study were as follows: to assess the knowledge about MHM among VIAGs, to determine the practice of MHM among VIAGs, and to identify the factors associated with the practice of menstrual hygiene among VIAGs.
Materials and methods
Study design
This study consisted of a cross-sectional study design using a quantitative approach. It was conducted on VIAGs studying at Rwamagana Home de la Vierge des Pauvres and Kibeho Institute for the Blind Children in the academic year 2020–2021.
Study setting and population
In Rwanda, there are currently four schools where individuals with visual impairments can receive education up to the secondary level and access the minimum necessary study materials. These schools include Kibeho School for the Visually Impaired in the Southern Province, HVP Gatagara Rwanda (Rwamagana), Musanze Blessing School of the Blind and Groupe Scolaire Gahini, both located in the Eastern Province. 31 For this study, Rwamagana Special School (Gatagara Home de la Vierge des Pauvres, GHVP) and Kibeho Educational Institute for Blind Children were selected because they have the specific population needed to address the research questions.31–33
Both institutions offer primary and secondary education and adhere to the official curriculum established by the Ministry of Education. These schools primarily support visually impaired children from across Rwanda and work in collaboration with families and the government to enhance knowledge and skills. However, many of these families face economic challenges and often show limited interest in the education of their visually impaired children. 32
The study focused on visually impaired girls aged 10–25 years, selected from a total population of 52 visually impaired students at GHVP Rwamagana and 47 VIAGs from Kibeho Educational Institute for Blind Children.
Sample size calculation
The single population proportion was used to determine the sample size.
The formula used to calculate the sample size.
With a confidence level of 95%, the sample size was calculated using Yamane’s formula.34,35

Therefore,
n: sample size; e: precision = 0.05; N: study population = 99 VIAGs.

n = 80 VIAGs (sample size of both schools).
To ensure the adequacy of the sample size and to account for any potential non-responses or dropouts, a 20% buffer was added to the original sample size, resulting in an expected total of 96 VIAGs from both schools. This adjustment was made to enhance the reliability and validity of the study findings by ensuring a sufficient number of participants. The sample size for each school was then calculated proportionally based on the population of visually impaired girls at each institution.


However, during data collection, the researchers were able to reach a total of 92 VIAGs. The shortfall from the expected sample size was primarily due to the COVID-19 outbreak, which resulted in some students falling ill and others being unavailable at the time of data collection.
Sampling techniques
The sample size was selected from the total population using simple random sampling; all classes and eligible girls were given an equal opportunity to participate in the study.
The researcher tossed papers to identify the starting class and continued until all classes were determined. The VIAGs who met the criterion were given the opportunity to pick a paper from the box and those with paper written on Yes were selected to participate. This continued until the desired sample size was achieved. Moreover, every VIAG had an equal chance of being selected. Because the students are visually impaired, there was one female teacher who facilitated the sampling procedure.
Inclusion criteria
VIAGs are available at the institution in the academic year 2019–2020. Aged between 10 and 25 years old who had menarche prior to the time of data collection and who voluntarily consented to participate.
Exclusion criteria
Those who were critically ill or very busy were excluded.
Data collection procedures and tools
Before commencing data collection, all data collectors received training on the study objectives, procedures, and ethical considerations. During data collection at each school, COVID-19 preventive measures were respected. An electronically fully structured interview (conducted in Kinyarwanda or English) took place in two classrooms, with the presence of one female teacher and one data collector to ensure accuracy and reduce potential bias. The VIAGs selected for the survey were identified with the assistance of teachers and the discipline committee.
The researcher explained the purpose of the study to the participants and guided them on how the questionnaire would be completed. For each respondent, the researcher read aloud the questions and response options, while the trained data collector accurately recorded the answers provided. This process ensured that the visually impaired participants could fully engage with the questionnaire, and having a teacher/guardian present helped confirm the responses, further minimizing any potential bias.
The study primarily relied on data collected using a fully structured questionnaire to capture accurate and relevant information from the participants. The questionnaire consists of three main parts: Part 1 includes sociodemographic and economic data including age, sex, educational level, mother’s occupation and education level, and number of sisters. Part 2 includes multiple choice and closed questions on knowledge of menstruation and menstrual hygiene. Part 3 includes multiple-choice and closed questions about the practice of menstrual hygiene.
The study instrument was developed based on different publications like the United Nations Children’s Fund (UNICEF) Guidelines published in 2018 and modified the questionnaire from other publications to Rwanda context and it was translated into Kinyarwanda for better understanding to the respondents.8,36 Also, the questions were linked to research objectives. Furthermore, the reliability of the tool was established by pre-testing the questionnaire on 20 VIAGs. This helped to ensure that the questionnaire was well-organized, consistent, clear, and acceptable. During data collection, the investigator checked the questionnaire daily for completeness. The completed questionnaire was also rechecked by the principal investigator to maintain the quality of the data.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 37
Data analysis and management
The scoring calculation for menstrual hygiene information was based on guidelines from UNICEF, WHO, and peer-reviewed literature on MHM.2,38,39 To assess knowledge, we considered sources of menstrual information, awareness about menstruation, and awareness of sanitary materials. Practices were evaluated based on the use of sanitary materials, frequency of changing pads/cloth, cleaning and drying underwear, genital hygiene, disposal of used materials, and daily activities.
Adequate MHM was determined through a scoring system, with each question assigned one point. Scores were converted to a percentage scale, categorizing the level of knowledge and practice: scores <70% indicated “inadequate,” 70% and above indicated “adequate.”2,40 The collected data were double-entered into SPSS version 25 for accuracy, then cleaned and analyzed https://www.ibm.com/docs/en/SSLVMB_25.0.0/pdf/en/IBM_SPSS_Statistics_Brief_Guide.pdf. Descriptive statistics were employed to summarize the characteristics of the participants, as well as their knowledge and practices related to MHM. Measures of central tendency like means were used for continuous variables, while frequencies and percentages were applied for categorical variables. Bivariate analysis was conducted to explore potential associations between independent variables (e.g., age, educational level, accessibility to MHM materials) and the dependent variable (adequate MHM practices). Pearson’s Chi-square tests were used to test for statistical significance, with a p value of less than 0.05 considered significant.
Variables that were found to be significantly associated with the outcome in the bivariate analysis (p < 0.05) were included in the multivariate model. Multivariate logistic regression was then employed to identify independent predictors of adequate MHM. The selection criteria for variables included all those with a p value <0.2 in the bivariate analysis, following the backward elimination method. This approach ensured that potential confounders were accounted for, even if they did not reach strict statistical significance in the bivariate stage.
The variable input method used in the logistic regression was stepwise, where variables were entered based on their significance level and retained if they improved the model fit. The model’s goodness-of-fit was evaluated using the Hosmer–Lemeshow test, with a non-significant p value (p > 0.05) indicating an adequate fit. 41 In addition, multicollinearity was checked using variance inflation factor (VIF), ensuring that all VIF values remained below the commonly accepted threshold of 10. 42 Results were presented using odds ratios (ORs) with 95% confidence intervals (CIs) to interpret the strength of association between independent variables and adequate MHM practices. Visual presentations of data included tables, graphs, and charts for clearer interpretation. All questionnaires will be securely stored for 5 years before destruction.
Results
Socioeconomic and demographic characteristics of respondents
Table 1 shows that 58.7% of the 92 respondents were aged 15–25 years, while 41.3% were younger. Most were in primary school (46.7%), with only 8.7% in advanced secondary level. Catholics made up 59.8%, and Muslims 3.3%. Menarche occurred between 12 and 15 years for 44.6%, while 13.0% experienced it after 15. In addition, 53.3% of mothers were illiterate, with 64.1% engaged in farming. Half (50.0%) of the respondents were in the third Ubudehe category.
Distribution of socioeconomic and demographic characteristics of respondents.

Knowledge about menstruation and menstrual hygiene among VIAGs
Table 2 shows that 72.8% of the 92 respondents heard about menstrual hygiene (MH) before menarche, while 27.2% learned about it after. Mothers were the primary source of information (38.0%). Most respondents (46.7%) recognized menstruation as a natural body process, and 41.3% correctly identified that menstruation lasts 2–7 days. In addition, 58.7% knew conception was possible during menstruation. However, only 32.6% demonstrated a good level of knowledge overall. Most respondents (82.6%) correctly knew that girls could cook during menstruation, and 81.5% understood they could attend school.
Knowledge about menstruation and menstrual hygiene among VIAGs.

MH, menstrual hygiene; VIAGs, visually impaired adolescent girls.
Practice of menstrual hygiene among VIAGs
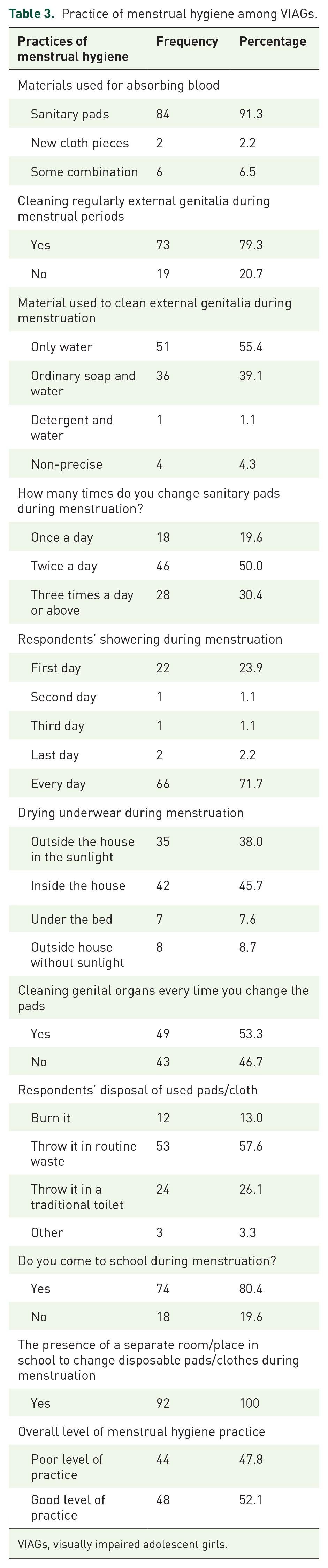
Table 3 presents that 91.3% of the 92 respondents used sanitary pads during menstruation, while only 2.2% used a new cloth piece. Most (79.3%) cleaned their genitalia regularly during menstruation, but 20.7% did not. Over half (55.4%) used water alone to clean, while only 1.1% used detergent. Half of the respondents (50.0%) changed pads twice daily, and 71.7% showered daily. Notably, only 38% of dried underwear is outside in sunlight. In addition, 53.3% cleaned their genitalia at every pad change, and 57.6% disposed of pads in routine waste. Overall, 52.1% demonstrated good menstrual hygiene practices.
Practice of menstrual hygiene among VIAGs.
VIAGs, visually impaired adolescent girls.
Bivariate analysis: Practice of MHM
Using bivariate analysis, the following variables were found significant as shown in Table 4: Age of respondents, level of education, mother’s education, mother’s occupation, family’s Ubudehe category, number of elder sisters, and overall level of knowledge on menstruation and menstrual hygiene. N = 92 VIAGS.
Distribution of practice of menstrual hygiene: bivariate analysis.

Multivariate analysis: Factors associated with the practice of MHM
Table 5 reveals that factors associated with the practice of MHM among the 92 VIAGs were the mother’s education and level of knowledge of menstruation and menstrual hygiene.
Multivariate analysis: factors associated with the practice of menstrual hygiene.

NAOR: Non Adjusted Odd ratio; AOR: Adjusted Odd Ratio.
VIAGs whose mothers were literate were 5.979 times more likely to practice good menstrual hygiene than those whose mothers were illiterate (OR: 5.979; 95% CI: [1.700–21.032]; p value: 0.005). In addition, VIAGs who had poor level of knowledge of menstruation and menstrual hygiene were 0.132 times less likely to practice good menstrual hygiene than those who had good knowledge (OR: 0.132; 95% CI: [0.028–0.622]; p value: 0.010).
Discussion
The findings from this study showed that the majority of the 92 respondents (67.4%) had a poor level of knowledge regarding menstruation and menstrual hygiene, while only 32.6% had a good level of knowledge. Similar studies conducted in Bangalore, India, and Ankara reported similar results, indicating that VIAGs tend to have insufficient knowledge about MH.18,43,44 However, a study done in Mangalore 5 revealed a higher percentage of girls (46.7%) with good knowledge, suggesting that other factors such as educational support or local awareness programs might be more effective in that region. It is crucial to consider that differences in sociocultural contexts, access to educational resources, or parental involvement may account for the variations in knowledge levels observed.
Other studies conducted in Chennai and Turkey12,45 proved differently that minimum girls had poor knowledge on menstrual hygiene.
The finding of the current study that only 31.5% of respondents knew the source of menstrual blood as the uterus mirrors results from a multivariate analysis study in India, where only 17.9% knew the correct source. 21 This suggests a widespread gap in basic reproductive health knowledge among visually impaired girls. The poor knowledge level observed might be attributed to the limited role of mothers in providing reproductive health education, as many were found to be illiterate. This suggests that mothers’ education level plays a crucial role in transmitting accurate information about menstrual health. Furthermore, the absence of structured inclusive menstrual health education programs in schools, combined with the lack of exposure to mass media and reduced father–daughter communication, may contribute to the girls’ lack of knowledge.
In terms of menstrual hygiene practices, this study found that 52.1% of the respondents demonstrated good practice, contrary to studies carried out in Ethiopia, Nepal, and India, where adolescent girls generally displayed poor menstrual hygiene practices.1,11,46 The difference in practices might be influenced by variations in access to sanitary materials, education on menstrual hygiene, or cultural beliefs. For example, in some cultures, restrictions during menstruation might hinder access to proper hygiene practices.
Interestingly, this study found no significant association between age and menstrual hygiene practices (p = 0.424), unlike an Indian study where older girls practiced better hygiene. 47 This difference could be explained by the unique challenges faced by VIAGs, where the opportunity to learn practical skills may not necessarily correlate with age due to visual impairment.
Furthermore, this study showed that factors such as the respondent’s level of education, mother’s occupation, family income, number of elder sisters, and sources of information did not significantly influence menstrual hygiene practices. These findings were consistent with a study conducted in Mangalore, 5 which also reported no significant associations between these factors and MH practices. However, in contrast, a study in Ethiopia found a significant link between family income and MH practices. 16 This suggests that while financial resources might be critical in some settings, they may not have the same influence in contexts where basic sanitary materials are provided by schools or community programs.
The most critical finding from this study was that a mother’s education and level of knowledge about menstruation and MH were significant predictors of good menstrual hygiene practices. VIAGs whose mothers were literate were 5.979 times more likely to practice good menstrual hygiene than those whose mothers were illiterate (OR: 5.979; 95% CI: [1.700–21.032]; p = 0.005). This aligns with studies from Ethiopia and India,16,21 suggesting that mothers’ literacy levels play a pivotal role in ensuring girls adopt proper menstrual hygiene practices. This emphasizes the importance of maternal education as a determinant of adolescent health behaviors.
Moreover, VIAGs with poor MH knowledge were 0.132 times less likely to practice good menstrual hygiene than those with good knowledge (OR: 0.132; 95% CI: [0.028–0.622]; p = 0.010), reinforcing that knowledge is a key factor in promoting healthy practices. Similar findings in Ethiopia indicate that targeted educational interventions could be effective in improving menstrual hygiene practices. 1
Study limitation
The limitations of this study include challenges related to generalizability, COVID-19 impact, and sample size. Given the cross-sectional quantitative methodology and the limited sample size drawn from two selected institutions, the findings are not generalizable to all VIAGs across Rwanda; rather, they reflect the specific contexts of the institutions under study. In addition, the study was conducted during the COVID-19 pandemic, which introduced restrictions and delays that may have impacted the study’s timeline and participants’ accessibility, potentially influencing data collection and overall study execution. The relatively small sample size may also have constrained the study’s ability to capture a comprehensive range of factors associated with MHM among VIAGs.
Conclusion and recommendations
This study assessed knowledge and practices of menstrual hygiene among VIAGs, finding that while knowledge was generally low, menstrual hygiene practices were good, particularly among girls whose mothers were literate or who had a better understanding of menstruation. To support VIAGs, an organized curriculum and standardized teaching protocols on MHM should be introduced in schools for visually impaired girls, alongside community and school campaigns to promote awareness. Health professionals can further contribute by educating communities to dispel menstrual misconceptions and guide proper hygiene practices. Future research could compare menstrual hygiene practices between visually impaired and non-visually impaired girls or explore these practices across varied age groups and settings.
Supplemental Material
sj-doc-1-reh-10.1177_26334941241303518 – Supplemental material for Knowledge and practice toward menstrual hygiene management and associated factors among visual impaired adolescent girls: a case of two selected institutions in Rwanda
Supplemental material, sj-doc-1-reh-10.1177_26334941241303518 for Knowledge and practice toward menstrual hygiene management and associated factors among visual impaired adolescent girls: a case of two selected institutions in Rwanda by Marie Laetitia Ishimwe Bazakare, Bernard Ngabo Rwabufigiri and Cyprien Munyanshongore in Therapeutic Advances in Reproductive Health
Footnotes
Appendix
Acknowledgements
This study would not have been possible without the support and encouragement of many individuals. First, the author extends sincere gratitude to the UR/SPH staff for sharing their knowledge and guidance throughout this research journey. The author is also thankful to the CMH IRB for their valuable insights. Special thanks go to the panelists for their assistance in reviewing this study, which contributed significantly to its success. The author is also grateful to the selected institutions for their facilitation and hospitality during the data collection period. Lastly, the author deeply appreciates classmates and friends for their continuous support and encouragement.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.