
Abstract
Background:
Adolescent girls face numerous challenges which hinder their ability to manage menstruation in a healthy and dignified manner.
Objectives:
To examine the menstrual hygiene practices of adolescent girls schooling in rural Anambra communities.
Study design:
Cross-sectional descriptive study.
Method:
Participants were selected using multistage stratified random sampling technique and interviewed using self-administered semi-structured questionnaire. Data were analysed using Statistical Package for Social Sciences version 22.0.
Results:
Mean age of all, pre-menarche and post-menarche girls were 14.7 ± 1.84, 12.8 ± 1.09 and 15.1 ± 1.73 years, respectively. About 46% of the pre-menarche girls had not received any information on menstruation. Common sources of initial menstruation information were mother (87.3%), school (52.2%) and peers (20.0%). Among the 1091 (85.0% (1091/1283)) post-menarche girls, last menstrual period, last menstrual period duration and cycle length could not be recalled by 53.9%, 34.4% and 39.3%, respectively. Majority (98.3%) who could recall last menstrual period had a cycle length of ⩽30 days and the mean duration of menses was 4.4 ± 0.84 days. Disposable sanitary pad was mostly (60%) cited as recommended product, but cloth/rags (40.6%) or tissue paper (32. 3%) were predominantly used. Majority (88.6%) took their bath ⩾twice/day, 50.9% changed sanitary product ⩽twice/day while 72.5% exhibited poor hand washing. Sanitary products were mostly discarded by burning (45.4%). Fifty-one percent could not change in school predominantly due to lack of functional toilets/changing rooms (84.2%) while 72.5% of those who changed did so in bushes or unused spaces. Challenges faced during menstruation include restriction from holy places (38.9%), waist pain (74.9%), blood stains (36.1%) and lack of money to buy pad (27.0%). Factors significantly associated with using commercial pads were age (p = 0.047), class (p = 0.006), mother’s educational status (p < 0.001), social class (p < 0.001), ability to recall last menstrual period date (p = 0.029) or duration (p = 0.001).
Conclusion:
Menstrual hygiene management was unsatisfactory among studied adolescents. Continuous education of adolescent girls on menstrual hygiene management and advocacy for adequate menstrual hygiene management support are imperative.
Introduction
Menstruation is a normal part of a woman’s life, intricately woven to the reproductive process. Therefore, optimal menstrual hygiene health (MHH) is a prerequisite for physical, psychological and emotional well-being of adolescent girls and women. 1 According to UNESCO, MHH involves accurate and timely knowledge about menstruation; available, safe and affordable sanitary materials; informed and comfortable professionals; referral and access to health services; sanitation and washing facilities; positive social norms, safe and hygienic disposal; and advocacy and policy. 2
Menstrual hygiene management (MHM) is essential for good sexual and reproductive health of females. It plays a critical role in enabling adolescent girls and women to attain their full potential. 3 Globally, about 800 million adolescent girls and women menstruate everyday. 4 Yet about 500 million females all over the world lack access to menstrual hygiene products and adequate facilities for hygienic management of menstruation. 1 According to WHO/UNICEF Joint Monitoring Programme, MHM is the use of a clean menstrual management material to absorb or collect menstrual blood, which can be changed in privacy as often as necessary, using soap and water for washing the body as required, and having access to safe and convenient facilities to dispose of used menstrual management materials.3,5 This also involves an understanding of the basic facts linked to the menstrual cycle and how to manage it with dignity and without discomfort, embarrassment, stigma or fear.
To effectively manage their menstruation, girls and women require access to adequate water, sanitation, and hygiene (WASH) facilities, affordable and appropriate menstrual hygiene materials and information on good practices. 2 They require access to facilities with privacy for changing materials used for menses, washing body and hands with soap and water, privacy for washing off stains from clothes with water and soap, facility for drying reusable materials and disposal facilities for used menstrual products from point of collection to final disposal. 2 MHM has been a challenging issue in developing countries due to water scarcity and insufficient access to WASH facilities and lack of privacy especially for in-school females. 5 In Nigeria, menstruating school girls are faced with numerous challenges which hinder their ability to manage their menstruation in a dignified and hygienic way. 6 These include unavailability or inadequacy of WASH facilities, lack of information on MHM and access to hygienic menstrual materials, and harmful taboos and myths associated with menstruation. 6 Reports indicate that more than 50% of schools in low-income countries such as Nigeria have inadequate, unsanitary, unsafe toilets for girls and female teachers. 7
Post Covid-19 pandemic, the economic situation in most countries has been dwindling, and in Nigeria, the onslaught of inflation and financial crisis has caused serious financial hardship. The implication of this is that MHM may be affected adversely. Currently, there is sparse literature on MHM knowledge and practices among secondary school students in southeast Nigeria especially in the post-COVID-19 pandemic period. Current data is needed to update the evidence, both locally and internationally, and for education and health policy formulation. This study aims to assess the menstrual hygiene knowledge and practices among female adolescents secondary school students in rural Anambra state communities in the post-Covid-19 pandemic period.
Methods
Study design
A cross-sectional study was conducted to examine the MHM knowledge and practice among adolescents girls aged 10–19 years, who were attending public secondary schools in rural communities selected from each of the three senatorial Zones in Anambra State, South East Nigeria. The study was conducted as part of the 2022 World Menstrual Hygiene Day celebration activities of the Medical Women’s Association of Nigeria (MWAN), Anambra State, between 23 and 31 May 2022.
Setting
The study was conducted in Anambra State, South East Nigeria, which has three senatorial zones namely Anambra North, Anambra South and Anambra Central senatorial zones. Each of the senatorial zones has seven Local Government Areas. Based on projected 2.2% annual population growth between 2006 and 2022, the projected population of Anambra State was 5,953,500 in 2022. 8 According to the 2006 Nigerian Census, the population structure of Anambra State is characterized by a male:female ratio of approximately 1:1, and 24% of the population are adolescents aged 10–19 years. 8
Sample size determination
For each of the three senatorial zones in Anambra State, a minimum sample size of 380 was calculated giving a total minimum sample size of 1140. Sample calculation for each zone was based on the sample size formula for cross-sectional studies (n = Z 2 pq/d 2 ), where Z is standard normal variate at 95% confidence interval (Z = 1.96), p is expected proportion in the population based on a previous southeast Nigerian study (p = 0.56), q is complementary probability (q = 1 − p = 0.44) and d = precision = 0.05.
Selection of participants
Two rural communities were randomly selected from each of the three senatorial zones. In each selected community, a public secondary school was randomly selected. Eligibility criteria was adolescent girls aged 10–19 years who had lived in the selected community for more than 6 months. Adolescent girls who were yet to attain menarche were excluded from the analysis on practice of MHM.
Subjects were selected using a stratified random sampling technique. Using the total number of female students in selected schools as the sampling frame, participants were proportionately selected from each school according to the school’s population by multiplying the school’s population with the sampling fraction. The number of subjects allocated to each school was stratified into the six grades of secondary school. The number of students selected from each grade was based on the ratio of girls in the different grades. In each grade, the girls were selected from one class using systematic random sampling. Where number of girls in the class slightly differs from allocated number, the entire class girls were studied.
Data collection/variables
Data were collected using a semi-structured interviewer-administered pre-tested questionnaire. Pre-testing was done among 20 adolescent girls from a rural secondary school which was excluded from the study. The questionnaire was first read out to the pupils and any question they had was addressed. Variables included relevant socio-demographic details, and MHM knowledge and practices. After data collection, the entire pupils in the school were enlightened on basic facts regarding menstruation, and how to manage their menstruation hygienically. Menstruation myths and misconceptions were debunked. Advocacy visit was paid to the school management on the need to ensure the provision of adequate WASH facilities for menstruating girls.
Ethical considerations
Ethical clearance (NAUTH/CS/66/VOL.15/VER.3/108/2022/099) for the study was obtained from the Research and Ethics Committee (REC) of NAUTH, Nnewi. Study was conducted in accordance with Helsinki declaration. Participation was entirely voluntary and all data was handled confidentially. A written consent and assent were obtained as appropriate.
Statistical analysis
Data were analysed using SPSS version 21. The relationship between categorical variables was examined using chi-square test while Student’s t-test was used to compare the means of continuous variables between different categories. p-value less than 0.05 was considered statistically significant. The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines was followed when preparing the manuscript.
Results
A total of 1283 public secondary school adolescent girls aged 10–19 years were studied, out of which 1091 (85.0%) had attained menarche while 192 (15.0%) had not. The age at attainment of menarche ranged from 10 to 15 years, with a mean of 12.7 ± 0.99 years.
The socio-demographic characteristics and menstruation status of the girls are displayed in Table 1. The mean age of all girls, those who had attained menarche and those who were yet to attain menarche were 14.7 ± 1.84, 15.1 ± 1.73 and 12.8 ± 1.09 years, respectively. The ratio of senior:junior secondary school students was 1:1.3. Regarding the socio-economic status of their families, more than three-quarter of their mothers (76.9%) and fathers (77.0%) completed secondary education while 52.8% and 39.4% of their families belonged to middle and lower social class, respectively. On whether they received any information on menstruation prior to attainment of menarche, 44.3% of the 192 girls who were yet to attain menarche replied in affirmative, 45.8% had not received any information while 9.9% were not sure whether they received or not. Among the 1091 who had attained menarche, 92.8% received information on menstruation before menarche, 5.3% did not receive while 1.9% were not sure whether they received or not. The commonest source(s) of initial information on menstruation and its management were mother (87.3%), school (52.2%) and friends (20.0%).
Socio-demographic characteristics and menstruation status of secondary school adolescent girls in Anambra.

Table 2 presents the knowledge of personal menstrual cycle characteristics and safe sanitary products among the girls who had attained menarche. When asked about their last menstrual period (LMP), more than half (53.9%) of them could not recall their LMP date while a third (34.4%) could not recall how long the period lasted. Among the 716 girls who could recall the LMP duration, the period lasted from 2 to 8 days, with a mean of 4.4 ± 0.84 days. Concerning their menstrual cycle length, only about 61% of them were able to recall the average cycle length out of which about two-thirds reported a cycle length of 25 days or less. About 60% of the menstruating girls cited disposable sanitary pads as the recommended menstrual product while 35.7% and 14.8% cited reusable cloth and tissue paper, respectively, as shown in Table 2.
Knowledge of personal menstrual cycle characteristics and safe sanitary products among secondary school adolescent girls in Anambra.
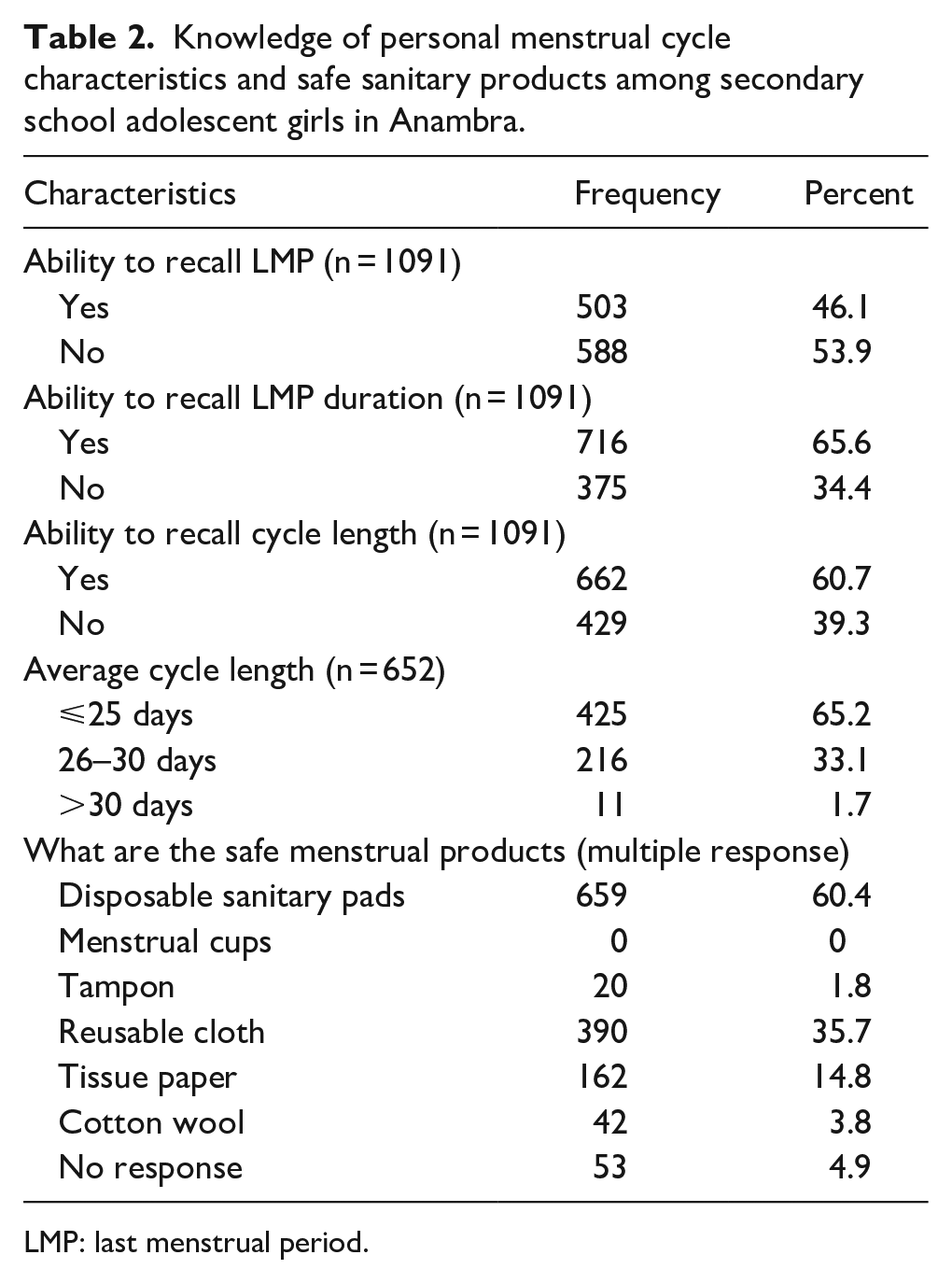
LMP: last menstrual period.
The MHM practices of the adolescents are presented in Table 3. Approximately 41% (443/1091) of them used reusable products in the form of reusable cloth/rags while the rest used disposable items such as tissue paper, cotton wool and sanitary pads during the LMP preceding the study. The most popular non-reusable product used was tissue paper (32.3%) and commercial disposable sanitary pad (23.7%).
Menstrual hygiene practice of secondary school adolescent girls in Anambra.

LMP: last menstrual period.
During their LMP, majority (88.6%) took their bath at least twice a day. However, about half (50.9%) changed sanitary product only twice per day or less while a considerable proportion (72.5%) did not often or always wash hands before changing sanitary product.
The most popular methods of handling used products, after changing, was burning (45.4%) and washing (20.8%).
Nearly half (49.0%) of the girls affirmed that they changed sanitary product during school hours about one-third of whom do so in bushes/farms within or around the school compound. The major reason cited for not changing during school hours was lack of functional toilets or changing room in the school (84.2%).
The commonest method used in tracking the menstrual cycle was making marks on a calendar at home (54.4%). A significant proportion of the girls (75.1% (819/1091)) experienced some menstruation-related myths or taboos, the commonest of which was restriction from certain places of worship (38.9%) as shown in Table 4. Of the health or psychosocial challenges associated with menstruation, waist pain (74.9%), blood stains on clothing (36.1%) and lack of money to buy sanitary products (27.0%) were the commonest.
Menstruation taboos and challenges experienced by secondary school adolescent girls in Anambra.
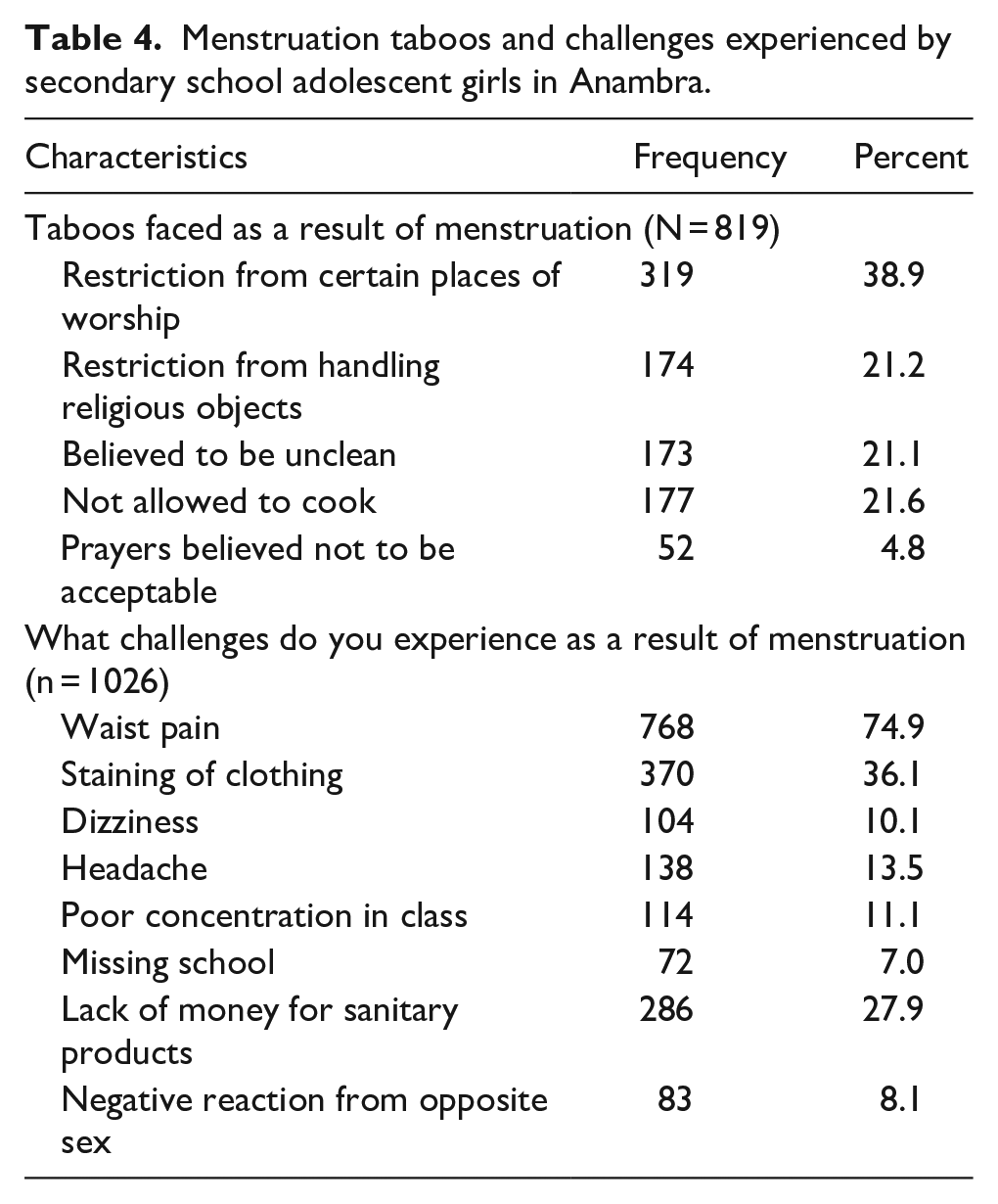
Table 5 presents the relationship between socio-demographic characteristics and type of material used for managing menstruation. A significantly higher proportion of older adolescents (p = 0.047), girls in senior classes (0.006), those who had more educated mothers (p < 0.001) or came from families with higher social class (p < 0.001), and those who were able to recall LMP date (p = 0.029) or duration (p = 0.001) used hygienic disposable sanitary pads instead of unhygienic products such as tissue paper, cotton wool or cloth rags.
Relationship between respondents’ characteristics and material used for menstruation.

LMP: last menstrual period.
Statistically significant
Discussion
Our findings highlight important gaps that may hinder achievement of optimal MHH among menstruating in school girls in rural communities. Despite the fact that the pre-menarche girls were predominantly at the median age for menarche, 45.8% of them were yet to receive any information on menstruation and its management. The finding that 92.8% of already menstruating girls had prior knowledge of menstruation before menarche implies a possibility of catch-up. However, the result still reflects the extent of missed opportunities in preparing young girls for MHH while they were still in primary school. The findings are contradictory to previous reports which indicate that majority of young girls are unaware of menstruation at menarche.4,6 Teaching pre-menarche girl about menstruation will ensure that she understands what will happen, why she should not be ashamed or scared when it happens, and the need to continue routine activities while menstruating.9,10 The opportunity can be used to debunk social taboos, myths and misinformation about menstruation. Girls who were educated about menarche and early menstrual patterns experience less anxiety when they start menstruating.6,11
The dominant role played by mothers as the initial sources of menstruation information agrees with previous reports.6,12,13 However, it is unsatisfactory that only about half of the girls obtained the initial information from school while none came from a healthcare worker. The responsibility should not be left solely for parents who may be poorly informed or reluctant to discuss issues pertaining to sexual health with the adolescent.10,13 According to the American Academy of Obstetricians and Gynecologists, clinicians should educate young girls and their caretakers on what to expect during first and subsequent menstrual period as soon as they turn 8 years. 10
The menstrual characteristics of the girls agree with previous reports from Anambra State study and the United States of America.10,12 However, awareness of personal menstrual characteristics such as ability to recall LMP, duration of LMP and cycle length fell below expectation. This may be attributed to the fact that up to a third of the girls do not track their menstrual cycle. Lack of such information may hamper the adolescent’s preparedness towards management of the menstrual period and contribute to unhygienic management of menstruation. Therefore, it is not surprising that this study found girls who had such information to be significantly more likely to use sanitary pads. It is recommended that every young girl should be taught how to track her menstrual cycle using appropriate technology. 10 This will equip her with details of her menstrual characteristics and promptly identify any deviation from normal. In addition, there is need to educate adolescent girls on safe menstrual materials since more than a third of our subjects had no idea on recommended products. It is imperative to build the capacity of young girls on MHM through active teaching programmes. Therefore, efforts should be intensified at fully integrating MHM into primary and secondary school curriculum, as well as school health programme and other preventive adolescent health programmes.
It is worrisome that a considerable proportion (76.3%) of the menstruating girls use unhygienic products such as reusable cloth rags, tissue paper and cotton wool. This contradicts report from Ethiopia which showed that 64.6% of girls use commercially produced adsorbent pads.14,15 Our findings also contrast reports from urban Nigerian settings which indicate a higher rate of commercial disposable pad use.16,17 The use of commercial disposable products could facilitate convenient and safer menstrual practices. However, cost of these products is a major deterrent.6,18 Therefore, it was not unexpected to find that a larger proportion of girls from families with higher social class and mother’s level of education significantly used commercial sanitary products. Reports indicate that choice of sanitary products vary according to socio-economic circumstances in developing countries. 18 In rural areas, the most preferred absorbents are reusable cloth pads while commercial sanitary pads are preferred in urban settings. A previous focus group discussion in three Nigerian States (Anambra, Katsina and Osun) revealed that commercial sanitary products are often not accessible to menstruating school girls. 6 The girls reported that local vendors within school premises often do not sell pads for emergency purchase. Where available, the pads were rather too expensive.6,16 In some school, cloth pieces were provided to the students for emergency use when menses starts during school hours. At home, girls may resort to use of pieces of clothes torn from mothers old blouses and wrappers, socks, old pants or scarves to keep themselves ‘packed’ in the absence of affordable commercial menstrual products.
Reusable and washable cloth pads may be cheap and sustainable but they must be hygienically washed, dried under sunlight and stored in a clean dry place to avoid contamination.1 –3 These conditions are often not met by cloth users, thereby exposing themselves to the risk of urinary and genital tract infections. 19 Sometimes, girls prefer to use tissues and cotton wool, which they consider to be less heavy, cheaper and easier to discard. 6 The above buttresses the need to train girls, families and schools on adequate preparedness for menstruation, and safe menstrual products. It is imperative to make safe sanitary products affordable and bank such products in school for emergency access.
Our findings agree with previous reports on the inadequacy of hygienic practices among menstruating girls in developing countries.20,21 Although majority of the girls (88.6%) took their bath at least twice daily, a considerable proportion (72.5%) did not often wash before changing sanitary products, and about half changed their pad only twice daily or less. This contrasts report from India where three-quarter washed hands while changing.22,23 In addition, more than half of the girls could not change while in school because of lack of facilities, and majority of those who changed did so in unsafe places such as bushes, unfinished buildings and toilets. This brings to fore the need to intensify advocacy on provision of adequate WASH facilities including changing rooms for menstruating girls.
Disposal of menstrual products is influenced by the type of materials used and cultural beliefs. Young girls are trained to keep used sanitary materials extremely private.6,16,18 This is to prevent it from being used by ritualists to perform rituals or witchcraft which are believed to be harmful to the girls. This could explain the finding that only about 10% of subjects in this study discarded their used sanitary materials into dustbins. This myth should be aggressively debunked to prevent delays in discarding used menstrual products as demonstrated by 5.2% of the study participants who were yet to discard used product as at the time of study, and 50.4% who had to wait for opportunity to burn or bury used sanitary product. To improve the psychosocial well-being of menstruating girls, practices such as restriction from places of worship, and handling religious objects and kitchen due to presumed uncleanliness, should be addressed. In addition, young girls should be trained on the appropriate management of waist pain and avoidance of stains, which was experienced by three-quarter and a third of the girls, respectively. This will enable them continue their daily activities without any intimidation or shame.
The information on menstrual hygiene practice and other experiences of the studied population was based on verbal response by the studied adolescent girls, rather than direct observation or interview of their parent/guardian where necessary. This may be prone to recall bias or tendency to report a practice that was deemed more acceptable, resulting in over-estimation of certain practices. Therefore, the study was limited by failure to confirm the actual menstrual hygiene practices. However, the findings are in keeping with some previous local studies and provide insight into the MHM and experiences faced by menstruating adolescent girls in Anambra State.
Conclusion
MHM is inadequate among secondary school girls in rural Anambra communities. There is inadequate knowledge of recommended products and personal menstrual characteristics, inadequate observance of personal hygiene during menstruation apart from bathing, and lack of facilities for changing during school hours. In addition, most girls use unhygienic products for menstruation. Active MHM teaching should be fully integrated into primary and school curriculum, school health programme and preventive adolescent health programmes. Safe sanitary products should be made affordable and easily accessible to menstruating girls.
{kind=link}