
Abstract
Objective:
The objective of this study was to establish the frequency of anxiety and depressive symptoms among women diagnosed with unexplained infertility and to identify risk factors.
Methods:
We conducted a descriptive cross-sectional study. Forty-two women from the CHU de Quebec fertility clinic were recruited. Women completed the ‘Hospital Anxiety and Depression Scale’ (HADS) self-administered questionnaire, used to estimate prevalence of anxiety and depressive symptoms (score ≥ 8).
Results:
Overall, 55% (n = 23) of participants were identified with anxiety or depressive symptoms according to the HADS questionnaire. Anxiety symptoms were more frequent (55%) compared with depressive symptoms (10%). According to a logistic regression model, being under 35 years old [odds ratio (OR) = 16.6, confidence interval (CI): 1.9–25.0], never had a previous spontaneous abortion (OR = 5.6, CI: 1.1–43.5) and never sought fertility treatment (OR = 5.5, CI: 1.1–45.4) were associated with a higher risk of anxiety and depressive symptoms.
Conclusion:
Anxiety and depressive symptoms are common among women with unexplained infertility, and strategies should be developed to better support and treat this high-risk population.
Introduction
Infertility affects about 80 millions of couples worldwide. 1 Ageing of couples trying to conceive has contributed to the rise in infertility in recent years. Infertility can cause significant psychological distress. About half of infertile couples state that infertility has been the most disturbing experience in their lives. 2 The intensity of anxiety and depressive symptoms is comparable with the one observed in conditions such as cancer, cardiac diseases or human immunodeficiency virus (HIV) infection. 3 This distress seems to be even more important for women compared with men 4 with a prevalence of anxiety and depressive symptoms of up to 90% and 50%, 5 respectively. Furthermore, a number of factors such as age, 6 socio-economical context 7 and duration of infertility 8 have been associated with the risk of anxiety and depressive symptoms in women and couples experiencing infertility.
Unexplained infertility represents a particular condition where no cause of infertility is identified and for which assisted reproductive technologies (ARTs), costly and invasive, are the only effective treatment options currently recommended [National Institute for Health and Care Excellence (NICE), American Society for Reproductive Medicine (ASRM)]. 9 Thus, women with unexplained infertility could be more likely to present psychological distress. Although it is estimated that 10% of infertile couples in Canada suffer from unexplained infertility, 10 little is available in the literature on the specific challenges faced by this population. The objective of this study was to assess the prevalence and predictive factors for anxiety and depressive symptoms among women diagnosed with unexplained infertility.
Materials and methods
We conducted a descriptive cross-sectional study at the fertility clinic of the CHU de Québec-Université Laval. We followed the STROBE check-list. Participants were enrolled among women accepting and signing a written consent to participate in a randomized controlled trial (RCT) on the efficacy of tubal flushing as a treatment of unexplained infertility. 11 The project was approved by the CHU de Québec-Université Laval Research Centre’s Ethics Committee (reference number: 2015-1146). Women were recruited during a follow-up visit following the completion of their initial fertility workup. Eligible women were aged between 18 and 37 years, had primary or secondary infertility for at least 12 months, and had met the diagnostic criteria for unexplained infertility in the last 36 months, 1 including (1) regular menstrual cycle of 25–35 days, positive ovulation tests and/or progesterone levels ⩾ 25 mmol/l; (2) normal sperm analysis according to the World Health Organization (2010) criteria 12 ; (3) FSH ⩽ 13 UI/l and AMH ⩾ 0.4 ng/ml 13 ; and (4) normal uterine cavity and patent tubes on imaging. Exclusion criteria included an ongoing pregnancy and severe obesity [body mass index (BMI) > 35]. A total of 42 women were included in the study between May 2016 and December 2017.
Participant characteristics and potential predictors of anxiety and depressive symptoms identified from the literature (sociodemographic characteristics, habits, interpersonal relationships, and gynaecologic and obstetrical history) were collected using a self-administered questionnaire pre-tested on 10 women. Anxio-depressive symptoms were also collected using the validated ‘Hospital Anxiety and Depression Scale’ (HADS) questionnaire 14 (validated French version, seven questions for anxiety and seven questions for depression), 15 as well as perceived level of daily life stress and impact of infertility on personal relationship. Data were collected as part of the baseline questionnaires completed by the study participants, before being allocated to any intervention. Anxiety or depressive symptoms were defined by a score of 8 or above on the anxiety or depression subscale, this threshold being associated with a sensitivity ranging from 0.83 to 0.89 and a specificity ranging from 0.78 to 0.79 for the screening of anxiety and depression disorders. 14 Study participants in the RCT completed their questionnaire before randomization or treatment.
Statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA). Fischer’s exact test and t-test were used for proportion and mean comparisons with a p-value < 0.05 considered statistically significant. We constructed a logistic regression model to identify predictive factors for anxiety or depressive symptoms (HADS ⩾ 8 on the anxiety or depression subscale). All potential predictive variables, as listed in Table 1, were introduced into the initial regression model. These variables were removed one at a time from the model, based on the highest p-value calculated using a partial inference statistical test, to include only variables with a p-value of less than 0.1. Finally, the reverse process was applied, and each of the variables removed from the final model was added again in the reverse order to ensure that the model was not modified. In addition, a Hosmer–Lemeshow fit test was used to validate the adequacy of the model. Missing data were rare (<3%), appeared to be random and were therefore ignored. Given the primary descriptive outcome, the sample size was fixed to the maximum number of consecutive women recruited over a period of 1 year as part of the RCT.
Participant characteristics (n = 42).
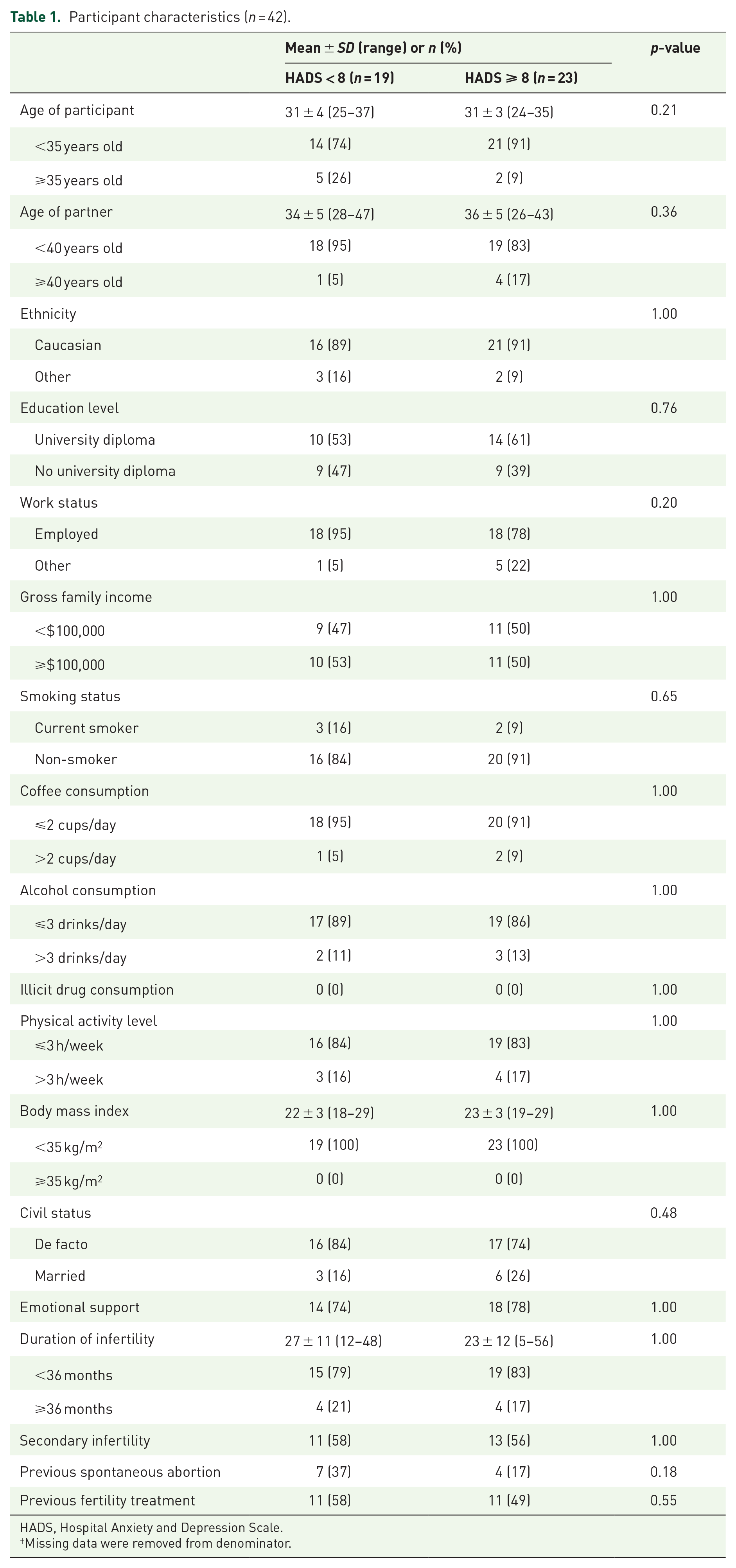
HADS, Hospital Anxiety and Depression Scale.
Missing data were removed from denominator.
Results
The characteristics of the participants are presented in Table 1. The mean age of participants was 31 ± 4 years and 57% (n = 24) had secondary infertility. Nearly half of the participants (n = 20, 48%) had never received any infertility treatment prior to enrolment in the study and were in the early stages of their follow-up at the fertility clinic.
Anxiety symptoms were shown to be common among the participants, being present in 55% (n = 23) of the women questioned (HADS score ⩾ 8). Depressive symptoms, although less prevalent, were also common with a prevalence of 10% (Table 2). All women who were identified with depressive symptoms also had a HADS score ⩾ 8 on the anxiety subscale. Nearly 30% of the women (n = 12) questioned reported experiencing a severe level of stress in their daily lives. A negative impact of infertility on their personal relationship was also reported in 29% of participants.
Levels of stress, prevalence of anxiety and depressive symptoms, and negative impact on relationship (n = 42).
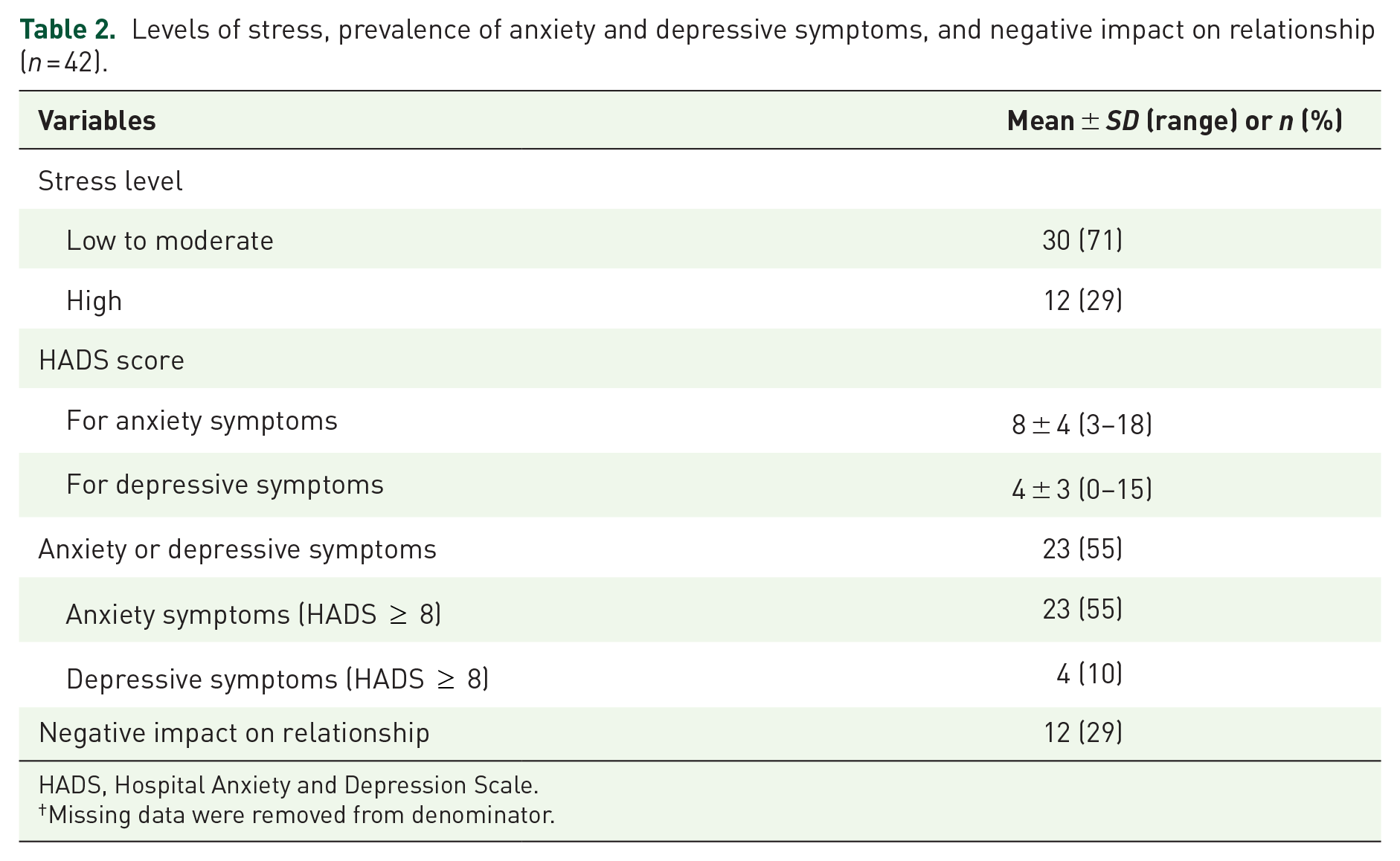
HADS, Hospital Anxiety and Depression Scale.
Missing data were removed from denominator.
Using a multiple logistic regression model, three predictive variables were identified as factors of anxiety and depressive symptoms. Being under 35 years old [odds ratio (OR) = 16.6, 95% confidence interval (CI): 1.9–25.0], never having had a previous spontaneous abortion (OR = 5.6, 95% CI: 1.1–43.5) and never having had any fertility treatment in the past (OR = 5.5, 95% CI: 1.1–45.4) were associated with a higher risk of suffering from anxiety or depressive symptoms. A p-value of 0.99 was obtained on the Hosmer-Lemeshow test, thus supporting a good fit of the model to the variables.
Discussion
Results from this study show that more than half of the women with unexplained infertility were experiencing significant psychological distress, with a prevalence of anxiety symptoms of 55% and of depressive symptoms of 10%. In fact, it seems that women with infertility are more likely to be affected by anxiety. 16 When comparing these results with the 90% prevalence of anxiety symptoms observed in a previous prospective study of 142 infertile women, 10 it could be suggested that women with unexplained infertility stand out with greater psychological distress compared with those with known aetiologies. When the cause of infertility is identified, the availability of targeted treatments could help decrease the anxiety of couples. The prevalence of anxiety symptoms observed in the present study is similar to that reported in women with ovarian cancer (56%) 17 and far exceeds the prevalence described for head and neck cancers (18%) using the same HADS questionnaire. 18 This comparison shows that infertility, although not a life-threatening condition, can have devastating psychological effects.
In the present study, almost a third of women reported a high level of daily stress and the same proportion of women reported adverse effects of infertility on their personal relationship. Indeed, several studies have observed negative impacts of infertility on the couple’s intimacy even affecting sexual function. In one study, nearly a quarter of women with infertility reported a decrease in the frequency of their sexual intercourse, potentially increasing the problem of infertility by reducing the chances of conception. 19
Interestingly, the use of infertility treatments has been found to be a protective factor for anxiety and depressive symptoms. In fact, having access to fertility treatments seems to be positively perceived by infertile women. In a study of 580 women with unexplained infertility, the use of intrauterine inseminations was better accepted than the expectation (96% versus 80%, respectively, p < 0.001), despite the lack of strong evidence supporting the efficacy of this treatment option. 20 Otherwise, it is also possible that women with psychological distress are less inclined to start fertility treatment. According to a prospective study, level of anxiety and depression also increase after failure to in vitro fertilization. 21 This suggests that new alternatives for treating unexplained infertility, such as tubal flushing, 11 could have a positive impact on couples suffering from unexplained infertility, by providing valuable and simple options before referral to ART.
Another interesting finding is the increased risk of anxiety and depressive symptoms in younger women. On one hand, a previous study observed an increased psychological distress in older women, 9 probably related to the decline in fertility prognosis with age. On the other hand, they could also be less likely to develop anxiety and depressive symptoms as a result of a better understanding of the cause of their infertility, a greater maturity and a better resilience to the situation. 22 Although a spontaneous abortion is an unfortunate event that can lead to significant psychological suffering, 23 results from this study show that it may also be a protective factor for anxiety and depressive symptoms, suggesting that previous success at conceiving could bring hope of another pregnancy.
This study presents both some strengths and limitations. First, a validated tool 14 was used to detect anxiety and depressive symptoms in the understudied population of women with unexplained infertility. In further studies, it would be interesting to extend the study to male partners, who are also at risk of experiencing psychological distress. 24 A wide range of potential predictive factors were investigated, such as socioeconomic status, lifestyle, interpersonal relationships, as well as gynaecological and obstetrical history. It is the uniqueness of this study. However, it is possible that some risk factors were not identified due to lack of power or because some aspects were not addressed in the study, such as personality traits, attitude towards stressors, or available support and resources. 22 Furthermore, although the logistic regression showed goodness of fit according to the Hosmer–Lemeshow test, large confidence intervals for predictive factors suggest a lack of power in our analyses. Finally, the use of a convenience sample from a single clinical centre and the relatively small sample size must be taken into account when generalizing these results to other populations.
Anxiety and depressive symptoms are common among women with unexplained infertility and seem to particularly affect younger women and those who never had fertility treatments or past pregnancy. Results from the present study suggest that it would be relevant to screen anxiety and depressive symptoms in women with unexplained infertility and to investigate strategies to better support and treat this high-risk population.
Footnotes
Acknowledgements
Authors would like to thank the clinical staff from the fertility clinic of the CHU de Quebec who assisted with the study as well as the staff of the Research Centre of CHU de Quebec for their help to collect data and support for good progess of this study.
Author contributions
The staff from fertility clinic of the CHU de Quebec helped for the recruitment.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The senior author is the recipient of a training award from the Fonds de Recherche du Québec-Santé.