
Abstract
Background:
Depression and anxiety are prevalent in the perinatal period and may contribute to adverse maternal and child health outcomes. A focus on multilevel protective factors may be effective in promoting well-being and increasing quality of life (QOL) in the perinatal period while simultaneously reducing or preventing depression and anxiety symptoms. We tested a conceptual model that posits specific personal, social, and community factors affecting depression, anxiety, and QOL among pregnant and postpartum individuals.
Methods:
Four hundred and thirty-eight pregnant or postpartum individuals completed a 121-item cross-sectional survey composed of validated tools that assessed multilevel protective factors, health behaviors, and mental health outcomes. Confirmatory factor analysis (CFA) was constructed to evaluate a 3-part conceptual model against measured indicators of well-being. A structural equation model (SEM) was then fit to test the pattern of associations between our latent structure and three end points: depression, anxiety, and QOL.
Results:
The CFA fit the data well (comparative fit index [CFI] = 0.907, Tucker–Lewis index [TLI] = 0.876, root-mean-square error of approximation [RMSEA] = 0.092) supporting the proposed conceptual approach to measuring well-being. The SEM fit well (CFI = 0.964, TLI = 0.941, RMSEA = 0.059), and all three end points were predicted in the hypothesized direction. Social factors predicted reduced anxiety symptomatology, personal and community resources predicted reduced depressive symptomatology, and social resources predicted increased QOL. In addition, we found that collective community resources were associated with social and personal resources, and social resources directly affected personal resources, showing the benefit of multiple levels.
Conclusions:
Our findings suggest that both the collection of and interplay between certain personal, social, and community-level resources may prevent and protect against depression and anxiety and promote QOL. Our conceptual model provides a framework to inform future interventions and clinical practice to better assess and promote maternal well-being during the perinatal period.
Introduction
Depression and anxiety are prevalent during the perinatal period (i.e., pregnancy throughout 1 year postpartum). Approximately 20% of pregnant individuals experience depression, and up to 40% report an anxiety disorder.1–5 The most common risk factors are personal history of a mood disorder, 6 exposure to life stress, 7 lack of social support,8,9 a history of adverse childhood experiences, 10 marital or partner dissatisfaction, 11 previous pregnancy loss,12,13 and medical complications.14,15 Untreated perinatal depression and anxiety are associated with high morbidity and mortality among mothers and their offspring, resulting in a significant economic toll, mainly attributed to reduced productivity among affected mothers and associated adverse maternal outcomes such as cardiovascular disease,16,17 hypertension, 18 and preeclampsia.19–21 In addition, untreated depression during pregnancy may increase risk of preterm birth and low birth weight,22–24 interrupted bonding between mother and infant,25,26 and detrimental growth and development outcomes from early childhood through adolescence,27,28 including delayed cognitive development and behavioral problems. 29
Perinatal depression and anxiety may be treated pharmacologically, including medications such as selective serotonin reuptake inhibitors,30,31 which are considered relatively safe 32 and effective treatment methods.33,34 Cognitive behavioral therapy35,36 as well as mind–body interventions are efficacious, nonpharmacological treatments for depression and anxiety during the perinatal period.37,38 However, these options are often limited due to socioeconomic barriers such as wealth inequality,1,7 limited access to adequate prenatal care,39,40 cultural factors and stigma that may prevent women from seeking treatment for perinatal mood disorders,41,42 perceptions of symptoms,43,44 and interpersonal distrust between patients and providers.45,46
The transition to motherhood may present unique stressors; however, women who are able to mobilize and utilize a combination of resources that foster their ability to effectively cope report more positive mental health and well-being during the perinatal period.47–50 Available resources may be garnered from a combination of system levels. 48 The socioecological framework is a conceptual model that illustrates an individual surrounded by various systems, namely the microsystem, which contains social influences, and the mesosystem, which consists of community-level influences. 51 Although there are additional progressively distal systems, our research focuses on the individual, the social, and the community resources that may be categorized by the socioecological model.
In our proposed conceptual model (Fig. 1), personal resources encompass beliefs, attitudes, and behaviors, including mindfulness,28,37,52 psychological capital, 53 gratitude, 54 self-efficacy, 55 and nature relatedness. 56 Social resources include influences through social support,57–59 including but not limited to a satisfactory and quality partnership.60,61 Community-level resources include access to adequate and quality care62,63 and resources available within a community’s built environment such as neighborhood attachment and cohesion. 64

Multilevel conceptual model to promote perinatal mental health and well-being.
The purpose of this study was to identify the collection of and the interplay among multilevel resources that can be modified using evidence-based strategies to promote well-being during the perinatal period. We conducted a cross-sectional survey of validated items measuring protective factors across personal, social, and community levels among pregnant and postpartum individuals to test and refine our proposed conceptual model based on extant literature to promote perinatal mental health and well-being.
Methods
All study procedures were approved by the Colorado Multiple Institutional Review Board (IRB No. 23-0272).
Recruitment
Recruitment of participants was completed through Centiment, an external company which provides panel recruitment to reach broad and representative audiences for the completion of survey research. 65 Individuals who were currently pregnant or had given birth within the last 12 weeks and were residing in Colorado were eligible to participate in the survey. Participants were recruited via advertisements and directed to Centiment’s website to complete an eligibility screener. Eligible participants subsequently completed an informed consent form followed by the survey. Participants were given a monetary incentive to complete the survey and were entered into a drawing for one of two $50 gift cards. All identifying information (email addresses) was obtained, classified, and discarded by Centiment and was not released to any members of the investigative team. To ensure genuine and accurate data, an “attention question” was placed near the middle of the survey. Those who answered incorrectly (indicating they were not reading the questions, but simply “checking boxes”) were directed to a termination link, and their data were not included in the final sample. All participation took place in January 2023. Data were compiled by Centiment using REDCap, 66 and then de-identified data were sent to the research team. SPSS 67 and Mplus 68 were used to conduct data analyses.
Survey
The final survey resulted in 121 items comprising validated items related to sociodemographic characteristics, protective factors across personal, social, and community levels, health behaviors, and mental health outcomes, described below.
Personal resources
The Mindful Attention Awareness Scale-5 (MAAS-5) 69 shows high internal validity (α = 0.92). Item analysis demonstrated that a 5-item scale shows the same results as the full survey or the 15-item survey which measures mindful awareness in daily activities (Nos. 7, 8, 9, 10, 14). The Compound PsyCap Scale (CPC-12) 70 measures psychological capital, which is the combination of self-efficacy, hope, optimism, happiness, and resilience. It measures all strength factors as well as the interplay between them. The Me as a Parent Short Form (MaaPs) 71 (α = 0.80) is a shortened, 4-item version of the 16-item measure of parental self-efficacy and self-management that can be completed by parents or caretakers of children and measures perceptions of their parenting role. The Gratitude Questionnaire-6 (GQ-6) 72 is a six-item self-report questionnaire with high reliability (α = 0.82–0.87) designed to assess individual differences in the proneness to experience gratitude in daily life. The GQ-6 is also positively related to optimism, hope, spirituality, and religiousness. The single-item Sleep Quality Scale (SQS) 73 was developed as a simple and practical sleep quality assessment as an alternative to the Pittsburgh Sleep Quality Index with similar internal validity (α = 0.76–0.92). The Short Form Nature Relatedness Scale (NR-6) 74 (α = 0.75) assesses the level to which one is connected to nature and how it may contribute to well-being. The survey also included self-report items to assess the frequency of health behaviors like physical activity, sleep, vitamin intake, alcohol consumption, and tobacco and cannabis use, but these were not included in the modeling due to the lack of robustness of single-item measurement.
Social resources
To assess relationship status, participants were simply asked “are you in a relationship.” The Relationship Quality Index (RQI-6) 75 is a 6-item measure designed to assess the quality of relationships in married and cohabiting couples. The Multidimensional Scale of Perceived Social Support (MSPSS) 76 shows an internal consistency of 0.90–0.94 in a prenatal sample. 77 To assess religiosity, one statement was presented from the 2006 Benchmark Social Capital Survey 78 (“My religion gives me a sense of who I am”) which participants were asked to rate from “not at all” to “very much.”
Community resources
The Revised Residential Environment Assessment Tool is a reliable, easy-to-use instrument that assesses items 127–132 from a multidimensional questionnaire for the measurement of perceived residential environment quality. 79 These items specifically measure neighborhood attachment and have a high validity (α = 0.91) when administered separately from the comprehensive scale. The Personal Social Capital Scale-8 80 (α = 0.83) is used for assessing personally owned social capital, including trustworthy and reciprocal relationships or partnerships, which leads to bridging and bonding to create a network.
Mental health and well-being outcomes
The Patient Health Questionnaire-8 (PHQ-8) 81 (α = 0.85) is a widely used validated diagnostic measure for depressive disorders. It shows high validity and reliability when using a cutoff score of 10. The Generalized Anxiety Disorder-7 (GAD-7) 82 scale is a brief measure of anxiety. When applied to a prenatal population, it shows high reliability (α = 0.89). When using a cutoff score of 7 or higher, the GAD-7 yielded a sensitivity of 73.3% and a specificity of 67.3%. Quality of life (QOL) was measured by self-reported Likert-type ratings of overall health, physical health, ability to carry out daily activities, absence of fatigue, and absence of pain. Items were identically scaled and were then standardized after being combined into a single QOL scale.
Data analyses
Each instrument was scored according to scoring instructions provided by its developer, and scores were standardized to z-scores for subsequent modeling. Variables were screened for floor and ceiling effects as well as distribution, with no significant issues identified. We fit an initial confirmatory factor analysis (CFA) model that positioned each of the proposed protective factors within its respective conceptual domain: personal, social, and community resources. After small model refinements were made, this measurement model was used to predict anxiety (GAD-7), depression (PHQ-8), and QOL in three separate models. Because these models examined the role that each of our factors played in predicting these correlates, we limited our models to z-score indicators for each scale rather than item-level indicator entry. Each model used Full-Information Maximum Likelihood estimation to avoid case loss due to missing data. Fit was assessed using comparative fit index (CFI), Tucker–Lewis index (TLI), and root-mean-square error of approximation (RMSEA). Based on initial model fit, we allowed for conceptually driven model specification that was also informed by modification indices.
Results
A total of 438 participants responded to some items on the survey. Because the survey allowed participants to complete the survey without responding to some items, we found that 360 respondents (90.9%) completed most items, with missingness ranging from 0% to 10.1% across items. Missing items were found to be missing completely at random (Little’s MCAR test chi square = 61.623, p = 0.994). For descriptive statistics, we used all available data for reporting. For structural equation model (SEM)-based analyses, we used Full-Information Maximum Likelihood estimation to utilize all available data for modeling.
The average age of the women who participated in the survey was 28.6 years. Of the sample, 20.4% identified as Hispanic. Of the sample, 67.1% identified as Caucasian, 22.4% as African American, and 10.5% as American Indian, Asian, Pacific Islander, or something other than these categories. Of the sample, 9.1% had less than a high school diploma, 34.7% completed high school, 29.9% had some college education, and 26.4% completed college or beyond. The majority of the sample (57.9%) was married or in a domestic partnership, 6.7% were divorced, separated, or widowed, and 35.4% were single. Of the sample, 41.3% were pregnant with or had just had their first baby, and 48.7% had other children (Table 1).
Participant Demographics (N = 438 a )

Participants were not required to answer every question. Therefore, although 438 total women completed the survey, the demographics shown in Table 1 reflect the numbers and percentages of respondents for each category.
SD, standard deviation.
Confirmatory factor analysis
A CFA was constructed to include the following indicators of conceptual latent variables as follows: Personal Resources was measured by Mindfulness, Psychological Capital, Parenting Self-Efficacy, Nature Relatedness, and Gratitude (Fig. 2). Social Resources was measured by Intimate Relationship Quality and Social Support from Family, Friends, and Significant Others. Community Resources was measured by Neighborhood Attachment and Personal Access to Community Resources. This initial model had marginal fit (CFI = 0.907, TLI = 0.876, RMSEA = 0.092), with the low correlations between Nature Relatedness and other constructs contributing substantially to this lack of fit. The model was respecified to remove Nature Relatedness and to allow for error correlations among the Friends, Family, and Significant Other subscales of the MSPSS since these all came from the same instrument. Moreover, the Friends subscale of the MSPSS demonstrated significant error variance correlations with the Community latent variable, so we estimated this error correlation as well. The respecified model demonstrated adequate fit (CFI = 0.963, TLI = 0.938, RMSEA = 0.071), and we moved forward to external correlate models with this as our base exogenous portion of the model.
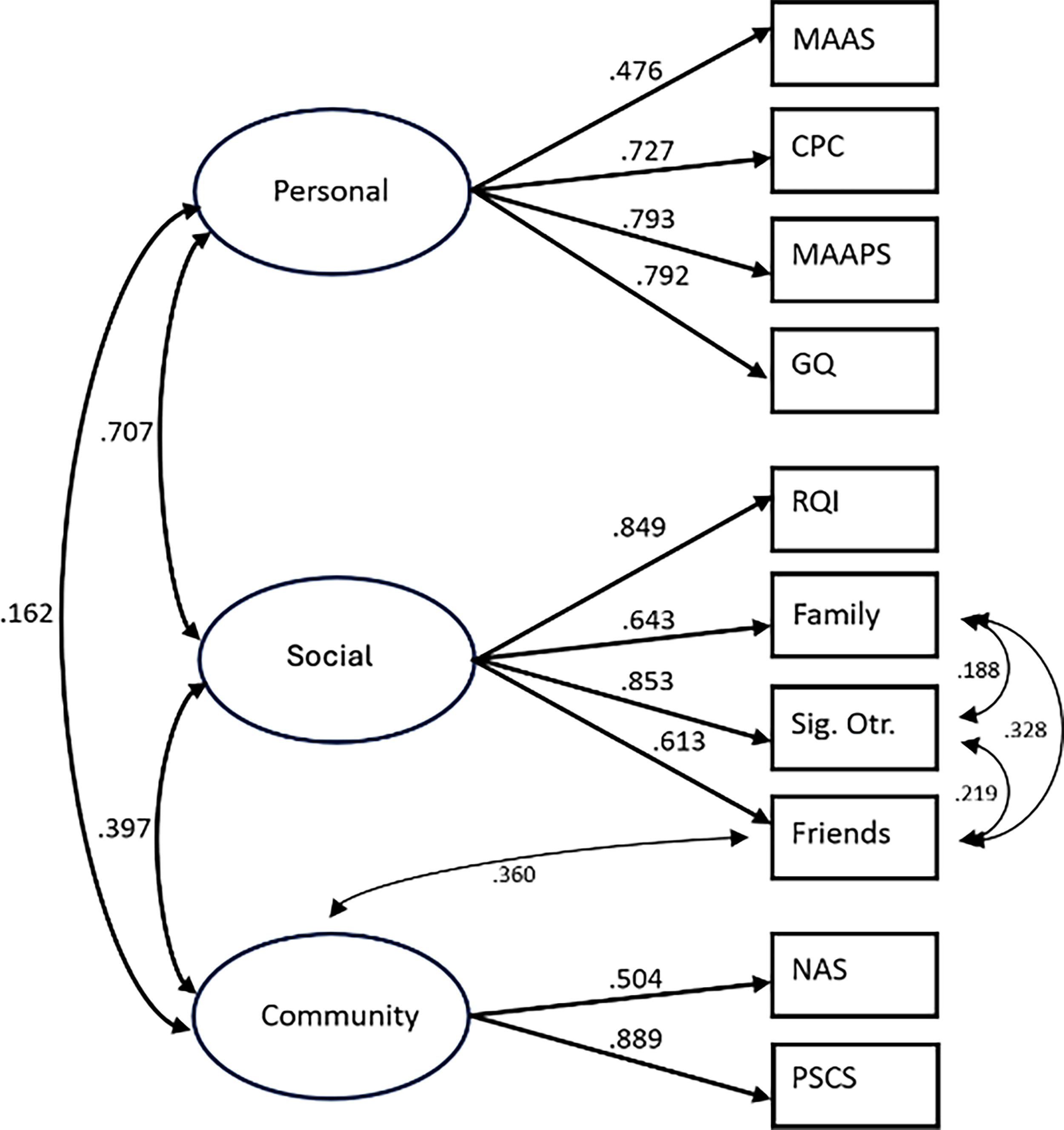
Confirmatory factor analysis for community, social, and personal resources. MAAS, mindfulness; CPC, psychological capital; MAAPS, parenting self-efficacy; GQ, gratitude; RQI, relationship quality; family, family-related social support; Sig. Otr., significant-other-related social support; friends, friend-related social support; NAS, neighborhood attachment; PSCS, personal social capital.
Model predicting anxiety, depression, and QOL
A SEM extended our base CFA in two ways (Fig. 3). First, the pattern of influence represented in our social–ecological model was modeled to test direct paths from community factors to social and personal factors, as well as a direct path from social to personal factors. This was done to capture the nesting structure in the model and to enable testing of indirect effects on our end points. Second, the model added three endogenous end point indicators for depression (PHQ-8), anxiety (GAD-7), and QOL. This expanded model demonstrated good fit with the data (CFI = 0.964, TLI = 0.941, RMSEA = 0.059).

Structural equation modeling predicting depression, anxiety, and quality of life with community, social, and personal resources. All coefficients displayed are standardized XY. Nonsignificant paths are not shown.
In this model, anxiety was negatively predicted directly by the Social Resources latent variable (b = −0.241; p = 0.020) such that higher values of Social Resources corresponded with lower levels of anxiety. Anxiety was not directly predicted by the Personal or Community Resources latent variables. We also observed a statistically significant indirect effect, such that Community Resources were positively associated with Social Resources, with Social Resources being negatively associated with Anxiety (b = −0.089, p = 0.040).
In this model, depression was negatively predicted directly by the Social Resources latent variable (b = −0.292; p = 0.004) such that higher values of Social Resources corresponded with lower levels of depression, but was positively predicted by Community Resources (b = 0.193; p = 0.002), which counterintuitively suggests that higher values of Community Resources were associated with higher levels of depression. Depression was not directly predicted by the Personal Resources. We also observed a statistically significant indirect effect, such that Community Resources were positively associated with Social Resources, with Social Resources being negatively associated with Depression (b = −0.108, p = 0.018).
In this model, QOL was positively and directly predicted by Personal Resources (b = 0.340; p ≤ 0.001) such that higher values of Personal Resources were associated with higher levels of QOL. QOL was not predicted by Community or Social Resources. We also observed a statistically significant indirect effect, such that Social Resources were positively associated with Personal Resources, with Personal Resources being positively associated with QOL (b = 0.253; p = 0.001).
Discussion
Our results support our proposed conceptual model. We found that the model fit well, with all three outcomes being predicted in the hypothesized direction. In particular, social resources predicted anxiety, personal and community resources predicted depression, and social resources predicted QOL.
Personal resources
Personal resources may aggregate and interact during the perinatal period to collectively influence prenatal, birth, and postpartum outcomes.48,83 Our results suggest that personal resources may be protective against depression. This finding is consistent with extant literature suggesting that mindfulness, self-compassion, and psychological capital may enhance maternal well-being and reduce the risk of perinatal mood disorders. In particular, extensive studies have investigated the impacts of mindfulness on perinatal mood disorders and found mindfulness to be protective for perinatal mental health and well-being.37,52 A recent systematic review found that maternal participation in mindfulness-based interventions was also associated with reduced perinatal anxiety of moderate-to-large magnitude. 28 Regular practice of mindfulness promotes self-compassion,84,85 a feeling of being kind and understanding toward oneself, rather than inflicting self-criticism.85,86 Self-compassion often enhanced with mindfulness practice is also correlated with significantly lower levels of anxiety and depression.84,85
Mindfulness practice may also help to harbor the tenants of psychological capital: optimism, hope, self-efficacy, and resilience. Optimism can be described as “a general sense that good things will happen” 52 and has been shown to be inversely correlated with prenatal depression. 53 In addition, optimism in pregnancy is associated with fewer depressive symptoms during the postpartum period. 54 Optimism can impact a woman’s overall health through the promotion of health behaviors such as substance use cessation, conscious healthy eating, physical activity, 87 and consistent participation in mind–body practices during pregnancy. 88 Optimism may also contribute to engagement in problem-focused coping strategies54,87 and is often used as a modifiable factor in the design of interventions and treatments for perinatal mood disorders. 53 Hope, much like optimism, is connected to the general belief of good things happening and is often related to the quality of prenatal care received. 89 Self-efficacy, while a strong indicator of well-being in the general population, takes on a more complex meaning when applied to parenthood; it is protective in itself while also a contributing factor to confidence and relationship satisfaction 55 as well as social connection, which was evident in our preliminary findings. Resilience, the ability to “bounce back” from difficult situations, is an important strength to foster in the case of difficult, high risk, 90 or unexpected pregnancies as well as adjusting to new family dynamics. 91 Access to nature and the presence of green space, including within the built environment, can be protective for maternal mental health. Social prescriptions in which health care providers or community health workers (CHWs) refer an individual to outdoor, health-promoting activities have been shown to promote overall well-being. 56 Nature-based social prescriptions can encourage women in the perinatal period, especially those in urban settings, to improve their mental health by “prescribing” outdoor activity. 92 Spending time outdoors can promote physical activity and relieve psychophysiological health, 93 especially among women living in low-resourced neighborhoods. 94 Furthermore, some studies link access to green space with more desirable birth outcomes, including birth weight, which can reduce risk for maternal depression and anxiety. 95
Social resources
Our study found that social resources are directly impacted by community resources, and social resources directly affect personal resources, confirming our prediction of the directional benefits of a multidimensional model. We found that social resources are specifically protective against anxiety, which reflects extant research.
Partner support is negatively associated with stress in the perinatal period, especially when the mother has risk factors for mood disorders.60,96 Marriage or domestic partnership is also protective against adverse birth outcomes such as low birth weight and preterm birth. 97 Having a partner may also increase health behaviors such as smoking cessation, diet, and physical activity. 97 Satisfaction within a relationship is also protective. Greater relationship satisfaction is negatively associated with perceived stress. 98 Furthermore, relationship satisfaction can increase self-efficacy and, therefore, boost well-being for both parents. 61 Evidence shows that women with higher perceived support from their partner during pregnancy and the postpartum period have decreased depression and anxiety. 99 This suggests that interventions may benefit from inclusion of partners or referrals to couples therapy if the relationship is less than satisfactory.
As our research shows, social support gained from family members, 100 peers,101,102 and friends is also protective. Perceived social support bolsters perinatal well-being 57 and also protects against perinatal depression and anxiety. 58 During stressful life events such as childbirth and the transition to motherhood, women are at an increased risk of perceiving inadequate social support and desire stronger support systems from partners, family, and peers. 103 Perceived social support during these critical periods mitigates the risk of depression for up to 12 months postpartum. 59 In addition, recent research shows that an increase in one source of support (i.e., partner, peer, or family) leads to an increase in other sources. 104
Community resources
Our results do not reflect the effects of individual constructs within the community level on well-being, but rather show that they collectively affect personal and social levels, as well as collectively show a negative association with anxiety. Taken together, the direct path between Social Resources and Depression and the indirect path that passes from Community Resources through Social Resources may have left little residual variance for the community resources factor, leading to an unusual and counterintuitive finding that merits further exploration.
Access to quality prenatal care, including referrals to specialists and resources for high-risk individuals, is critical for salubrious maternal and child outcomes.105–107 Women’s beliefs and behaviors may be influenced by prenatal health providers via the appraisal and informational support they provide.108,109 Women who value and trust the opinion of their health care providers are more likely to adhere to perinatal care guidelines related to self-care such as diet, exercise, and sleep recommendations.110,111 Respectful care also includes autonomy, the ability and confidence to make decisions about their pregnancy and birth. 112 Structured support in the form of community offerings such as parenting classes and support groups may encompass all levels of resources, as social connections may be made and relationships made stronger, and strategies taught may strengthen personal constructs. Finally, as quality prenatal care is often not equitably accessible, 62 there is a highlighted need for CHWs such as promotoras, doulas, and other community-based leaders to provide support for families navigating the perinatal period and beyond.105–107,113,114
The built environment (e.g., structural factors within a community) also influences maternal well-being. Strong neighborhood integration and cohesion may decrease stress and promote positive coping by providing a social network, supportive community, and access to instrumental resources.115,116 Low neighborhood cohesion within low-resourced communities creates a compound effect increasing social isolation and exacerbating maternal stress and depression. 117 Increasing social contact and trust among neighbors reduces fear and protects well-being, especially among residents in low-income neighborhoods, and provides social support that is lacking in family or friends. 118 Community interventions designed for low-income families that provide opportunities for parents to connect with peers in their community have been successful in well-being promotion. 119 Specifically, connections between parents are often protective and foster peer advice, support, and connections to other community resources. 120 This model of community intervention could be applied specifically to the perinatal population to promote instrumental support and resource acquisition.
Our conceptual model proposes that women may benefit by garnering resources across multiple levels to promote their well-being during the perinatal period. Network connections promote the interaction of these personal, social, and community resources. Social capital refers to resources which are embedded in social networks. 121 This occurs through two network pathways: bonding and bridging. Network connections that promote bonding provide direct emotional and appraisal support by members within a pregnant individual’s personal network (e.g., partner, family, and close friends). In addition to partner and family support, shared experiences in the form of peer interaction enhance bonding and help mitigate mood disorders among pregnant women, demonstrating the need for community-based facilitation of structured peer support during the perinatal period.122,123 Multiple “layers” of various types of support are more likely to be achieved related to the number of people a woman in the perinatal period considers to be in her network, 124 and research shows that the number of ways a person feels connected can cumulatively protect their mental health. 125 The concept of “bridging” to promote social capital includes the expansion of one’s network beyond family and close friends to accessing community resources. More diverse social networks lead to greater access to information and community resources and, in turn, promote physical 126 and mental health.122,123
Conclusion
The perinatal period can be a stressful transitional time for many women. Identifying effective resources to promote well-being and decrease the risk of perinatal mood disorders during this time is essential. Screening for risk factors alone may overlook potentially beneficial resources and opportunities for utilizing strengths. Our preliminary research shows directional effects on collective, multilevel protective factors, highlighting the importance of assessing and addressing perinatal mental health and well-being on multiple levels, and underscores the importance of connecting women to protective resources to promote perinatal well-being. More research is needed to better understand the interplay across these proposed pathways and resulting mechanisms that translate to improved maternal well-being during the perinatal period. This understanding can further inform the development of strengths-based screening instruments and protocols to connect women to existing multilevel, evidence-based resources that promote well-being during a critical time.
Authors’ Contributions
Conceptualization and study design: J.A.L., C.V.F., and J.F.P. Analysis and interpretation: J.A.L., C.V.F., and J.F.P. Writing—original draft: J.A.L., J.W.W., C.V.F., C.W.-M., and J.F.P. Writing—review and editing: J.A.L., J.W.W., C.V.F., C.W.-M., and J.F.P.
Footnotes
Acknowledgments
The authors would like to acknowledge Rachael Lacy for her contribution to the early conceptualization of this article. The authors would also like to acknowledge the women who participated in the survey.
Author Disclosure Statement
The authors report no conflicts of interest in this work.
Funding Information
This research received no specific grant from any funding agency in the public, private, or not-for-profit sectors.