
Abstract
Introduction:
Premenstrual dysphoric disorder (PMDD) is characterized by cyclical affective, cognitive, and somatic symptoms that occur during the late luteal (LL) phase. The primary objective of this study was to investigate changes in affective symptoms, emotional regulation, and psychological resilience across different menstrual phases in women with PMDD compared with healthy controls. Our secondary objective was to determine how comorbid emotional disorders and baseline psychological resilience moderate these patterns.
Methods and Materials:
A total of 58 women with PMDD and 50 healthy controls were examined during three menstrual phases: the preovulatory phase, midluteal phase, and LL phase. The study used various instruments to evaluate depression, anxiety, emotional regulation (Affective Style Questionnaire), and psychological resilience (14-item Resilience Scale) in the participants. Diagnostic interviews identified comorbid major depressive disorder and generalized anxiety disorder.
Results:
The results revealed that compared with the control group, the PMDD group exhibited significantly higher depression and anxiety levels across all phases, with peak symptoms during the LL phase. Emotional regulation and psychological resilience significantly declined during the LL phase. Women with both PMDD and comorbid emotional disorders exhibited persistently stronger affective symptoms and lower psychological resilience. Higher psychological resilience was correlated with lower depression and anxiety.
Conclusion:
PMDD involves phase-dependent emotional dysregulation and reduced psychological resilience, particularly during the LL phase. Emotional comorbidities exacerbate baseline affective vulnerability. Enhancing emotional regulation and psychological resilience may represent a key therapeutic target for improving emotional stability and quality of life in women with PMDD.
Keywords
Introduction
Approximately 1%–8% of women of childbearing age experience a series of mood-related, cognitive, and somatic symptoms during the late luteal (LL) phase, which often result in functional impairments. 1 These symptoms are collectively referred to as premenstrual dysphoric disorder (PMDD), which is classified as a subtype of depressive disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 2 Although several studies have explored the overall effects of depression and anxiety,3,4 the effects of these comorbidities on women with PMDD remain incompletely understood. In addition, whether emotional regulation and psychological resilience are affected by depression and anxiety in women with PMDD has not yet been comprehensively examined.
A review article revealed that PMDD was associated with an increased risk of depression and that having a history of depression was associated with an increased risk of PMDD. 5 According to the literature, the symptoms of PMDD, which include depression and anxiety, typically start to disappear within a few days after the beginning of menstruation. 2 However, whether women with both PMDD and a comorbid depressive or anxiety disorder actually experience a symptom-free follicular phase warrants examination. A study reported that women with generalized anxiety disorder (GAD) were more likely than others to have PMDD; in addition, the study indicated that women with PMDD and comorbid GAD experienced more severe anxiety symptoms, and their mood symptoms were not relieved during the follicular phase, unlike women without comorbid GAD. 4 Accordingly, we hypothesized that women with PMDD are more likely than others to experience depressive and anxiety disorders. We also hypothesized that women with PMDD and comorbid GAD are more likely to experience stronger emotional symptoms and to have poorer resources for coping with the symptoms of PMDD.
Emotional regulation is a process used to control and express emotions. 6 Different emotional regulation strategies lead to distinct long-term psychological and physiological health outcomes. For example, adaptive emotional regulation strategies such as reappraisal and mindfulness have a positive effect on the mood of women with PMDD during their menstrual cycle. 7 Women with PMDD often experience negative mood symptoms during the LL phase. In these women, the capacity for emotional regulation changes across the phases of the menstrual cycle. 8 Accordingly, we hypothesized that women with PMDD have a relatively low capacity for emotional regulation and that this capacity further decreases during the LL phase.
Resilience refers to an individual’s inner strength, competence, optimism, flexibility, and ability to cope with adversity. 9 Psychological resilience may help individuals cope with negative mood in cases of distress. Studies have indicated that interventions focusing on improving psychological resilience can reduce the severity of symptoms in women during their premenstrual syndrome phase.10,11 Accordingly, we hypothesized that women with PMDD tend to have relatively low levels of psychological resilience, particularly during the LL phase. We also hypothesized that psychological resilience can protect against the emotional reactions of PMDD during the LL phase.
The primary objective of this study was to explore the cyclical psychopathology of PMDD. Specifically, we examined whether women with PMDD experience unique changes in their affective symptoms (depression and anxiety), emotional regulation, and psychological resilience across different phases of the menstrual cycle (preovulatory [PO] phase, midluteal [ML] phase, and LL phase) when compared with a healthy control group. Our secondary objective was to determine how factors such as emotional comorbidities (GAD and MDD) and baseline psychological resilience level moderate symptom severity and cyclical changes in women with PMDD.
Methods
Participants
This study recruited participants by posting advertisements on the Professional Technology Temple (PTT), one of the largest online forums in Taiwan, from April 2018 to December 2020. The advertisement introduced a research project on PMDD and invited women with regular menstrual cycles to participate either in a PMDD group (with ≥5 PMDD symptoms listed on the advertisement that improved after menstruation) or in a control group (with no symptoms or mild symptoms with no functional impairment). Interested women contacted the research team by e-mail to be initially screened based on self-reported premenstrual symptoms. All women who met these preliminary criteria were invited to the hospital and were interviewed face-to-face by a psychiatrist using DSM-5 criteria for PMDD 2 and the Mini-International Neuropsychiatric Interview to exclude psychotic disorders and bipolar I disorder in both the PMDD and control groups. 12 A total of 71 and 66 women were assigned to the PMDD and control groups, respectively. Of these women, 58 with PMDD and 50 healthy were included in the final analysis after the elimination of women with irregular menstrual cycles or unfulfilled symptomatic cycles during testing, as described subsequently in the procedure section. Informed consent was obtained from all participants involved in this study. This study was approved by the Institutional Review Board of Kaohsiung Medical University Hospital (KMUHIRB-SV(I)-20160049).
Measures
DSM-5 diagnostic criteria for PMDD
The majority of women reported five or more menstrual cycles characterized by affective lability, irritability, depressed mood, anxiety, lack of concentration, lethargy, overeating, sleep problems, sense of being overwhelmed, and physical symptoms occurring during the final week before the onset of menses and disappearing within a few days after menstruation. These symptoms occurred over the preceding year and were associated with high levels of distress regarding work, school, social activities, or relationships, as confirmed by prospective daily ratings across at least 2 symptomatic cycles. 2 These prospective ratings are outlined in the Procedures section.
Chinese version of the Mini-International Neuropsychiatric Interview
Diagnostic interviews were conducted using the modules for MDD, dysthymic disorder, GAD, psychotic disorders, bipolar I disorder, and substance use disorder in the Chinese version of the Mini-International Neuropsychiatric Interview. 12 These interviews were conducted to determine whether the participants had MDD or GAD and to exclude other psychiatric disorders. Participants with depressive episodes, persistent depressive disorder, or a history of depressive episodes were classified as having depressive disorders.
Resilience Scale
The Resilience Scale is a 14-item instrument developed to determine the levels of resilience in the general population. 9 On this scale, scores of <65 indicate low levels of resilience, scores of 65–81 indicate moderate levels of resilience, and scores of >81 indicate high levels of resilience. In the present study, this scale was used to measure the participants’ levels of resilience. Participants with scores of <65 were classified as having a low level of resilience, and participants with scores of ≥65 were classified as having an adequate level of resilience.
Affective Style Questionnaire
The Affective Style Questionnaire (ASQ) is a 20-item instrument that covers the dimensions of concealment, adjustment, and tolerance. 13 Each item is rated on a 5-point Likert scale. In the present study, the internal consistency values for the ASQ subscales of concealment, adjustment, and tolerance were determined to be 0.84, 0.80–0.82, and 0.66–0.68, respectively. Overall, this scale was used to assess the tendency of emotional regulation. Depression and anxiety were evaluated using the Center for Epidemiologic Studies Depression Scale14,15 and the Penn State Worry Questionnaire, respectively. 16
Procedures
All participants were examined during their PO phase, ML phase (approximately 7 days after ovulation, validated using an ovulation prediction kit), and LL phase (2 days before the predicted onset of menstruation) within the same menstrual cycle. The PMDD Severity Questionnaire 17 was administered once a week for two menstrual cycles. Symptomatic cycles were defined according to the criteria of Smith et al. 18 ; the mean luteal-phase PMDD symptom score had to be at least 30% higher than the mean follicular-phase score. Data from participants with PMDD who met the symptomatic cycle criteria for two consecutive menstrual cycles were included in the final analysis.
Statistical analysis
A chi-square test was conducted to examine the association between MDD, GAD, and PMDD. Participants with MDD or GAD were assigned to an emotional comorbidity group to represent those with at least one anxiety- or depression-related disorder (referred to as an emotional comorbidity). An independent t-test was used to determine the difference in depression, anxiety, emotional regulation, and psychological resilience between the PMDD group and the control group during the PO, ML, and LL phases. A repeated-measures analysis of variance was conducted to determine the effect of the interaction between menstrual phase (ML phase vs. PO phase or LL phase vs. PL phase) and PMDD diagnosis on depression, anxiety, emotional regulation, and psychological resilience. A p value of <0.05 was considered statistically significant.
Results
Participant characteristics and psychiatric comorbidities
No significant differences were observed between the PMDD and control groups in terms of age or educational level. Compared with healthy controls, women with PMDD were significantly more likely to have GAD or MDD (Table 1).
The Comorbidity of Generalized Anxiety Disorder (GAD) and Major Depressive Disorder (MDD) Among Women with Premenstrual Dysphoric Disorder (PMDD) and Their Emotional Regulation and Resilience

Score of the Center for Epidemiologic Studies Depression Scale (CES-D).
Score of the Penn State Worry Questionnaire (PSWQ).
Score of subscales in the Affective Style Questionnaire (ASQ).
Score of 14-item Resilience Scale.
*p < 0.05; **p < 0.01; ***p < 0.001.
Group differences in psychological variables across menstrual phases
Independent t-tests (Table 1; Fig. 1) revealed that women with PMDD experienced significantly higher levels of depression during all three phases of the menstrual cycle. They also had significantly higher levels of anxiety during the ML phase and LL phase. Subscale analysis results indicated that women with PMDD had significantly lower scores on the adjustment subscale during the LL phase. They also had significantly lower levels of self-reported psychological resilience, but only during the LL phase.

The differences in depression, anxiety, emotional regulation, and resilience between women with PMDD and controls during preovulation (PO), midluteal (ML), and late luteal (LL) phases.
Interaction effects of menstrual phase and PMDD diagnosis
A comparison of the ML and PO phases revealed a significant interaction effect with PMDD for emotional regulation (Table 2; Test 1 for menstrual phase effect [ML vs. PO]), indicating that the change observed in emotional regulation from the PO to the ML phase significantly differed between the PMDD and control groups. A comparison of the LL and PO phases revealed significant interaction effects across all primary variables: depression, anxiety, emotional regulation, and psychological resilience (Table 2; Test 2 for menstrual phase effect [LL vs. PO]). Overall, these results confirm that the trajectory of change in symptoms and psychological resources from the follicular to the LL phase differs significantly between women with PMDD and healthy controls.
The Repeated Measures ANOVA Analysis for the Effect of Menstrual Phases and PMDD Diagnosis on Depression, Anxiety, Emotional Regulation, and Resilience

Score of CES-D.
Score of PSWQ
Score of ASQ.
Score of 14-item Resilience Scale.
*p < 0.05; **p < 0.01; ***p < 0.001.
ANOVA, analysis of variance.
Influence of emotional comorbidities in women with PMDD
Further analysis of the PMDD group (Table 3; Fig. 2) revealed significant differences between women with emotional comorbidities (PMDD + C group, N = 17) and women without (PMDD−C group, N = 41). Compared with the PMDD − C group, the PMDD + C group reported significantly higher levels of depression and anxiety and significantly lower levels of psychological resilience during the PO phase.
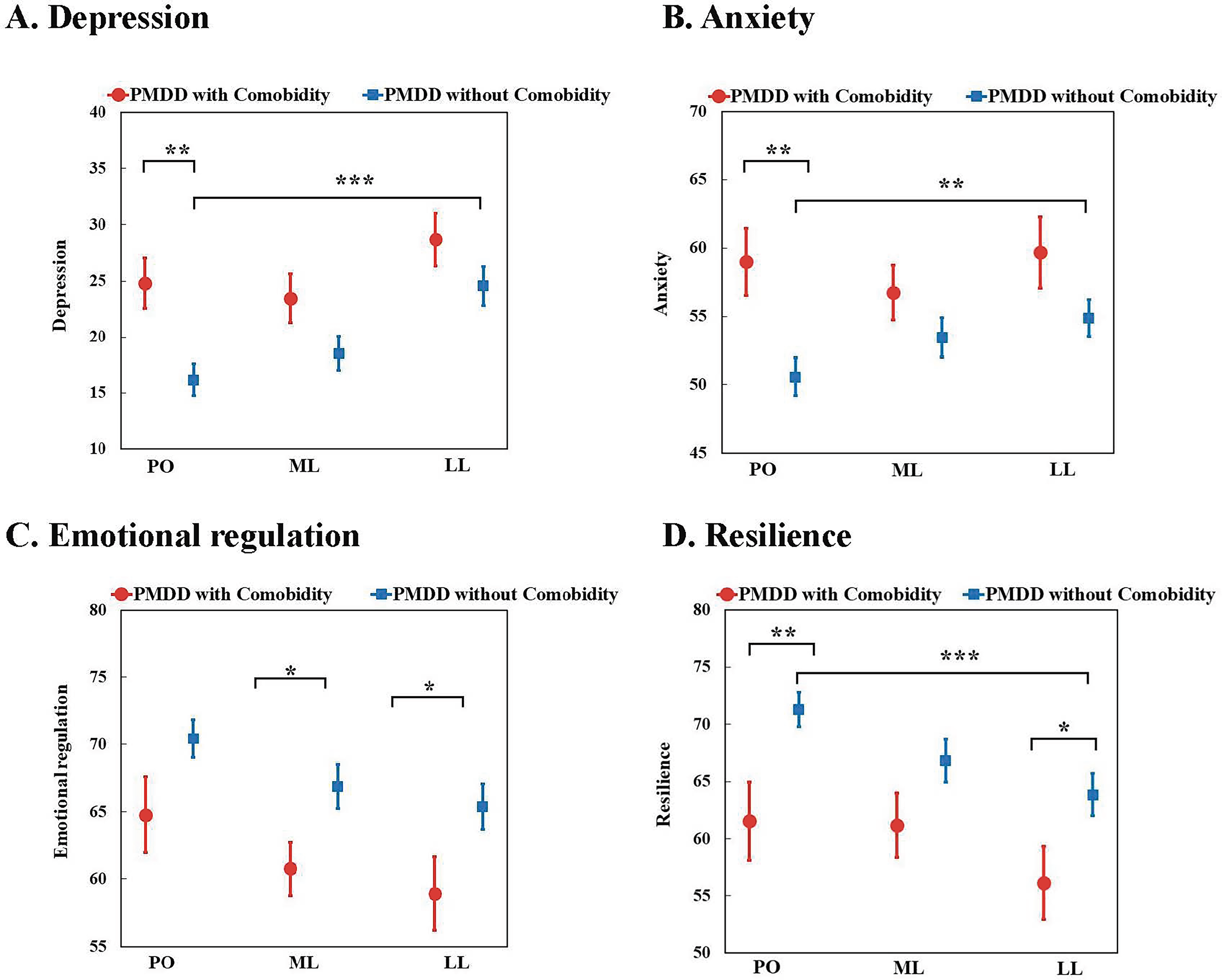
The differences in depression, anxiety, emotional regulation, and resilience between PMDD women with comorbidity and those without during PO, ML, and LL phases.
The Difference in Depression, Anxiety, Emotional Regulation, and Resilience Between PMDD Women With Emotional Comorbidity (PMDD + C) and Without Emotional Comorbidity (PMDD − C)

Score of CES-D.
Score of PSWQ.
Score of ASQ.
Score of 14-item Resilience Scale.
*p < 0.05; **p < 0.01; ***p < 0.001.
Paired t-tests of changes from the PO to the LL phase demonstrated that the premenstrual exacerbation of depression and anxiety was statistically significant only in the PMDD−C group. No significant increase was observed in the PMDD + C group, who had stronger baseline symptoms. However, the two subgroups experienced a significant decline in the levels of emotional regulation and psychological resilience during the LL phase.
Correlations of emotional regulation and psychological resilience with affective symptoms
As presented in Table 4, Pearson’s correlation analysis of the PMDD group indicated that higher levels of emotional regulation were significantly associated with lower levels of depression and anxiety. Specifically, strong negative correlations were observed between the adjustment and tolerance subscales and the symptoms of depression and anxiety. Higher levels of psychological resilience were also significantly associated with lower levels of depression and anxiety.
The Association Between Emotional Regulation and Resilience to Depression, Anxiety, Irritability, and Severity Among Women with PMDD

Score of CES-D.
Score of PSWQ.
Score of subscales in ASQ.
Score of 14-item Resilience Scale.
**p < 0.01; ***p < 0.001.
Role of psychological resilience in symptom expression
After the PMDD group was dichotomized on the basis of psychological resilience level (Table 5), women with lower levels of psychological resilience (N = 33) were noted to have significantly higher depression and anxiety scores across all three menstrual phases compared with women with adequate levels of psychological resilience (N = 25). In addition, women with lower levels of psychological resilience demonstrated significantly poorer emotional regulation during the ML and LL phases.
The Difference in Depression, Anxiety, Irritability, Emotional Regulation, and Resilience between PMDD Women with Adequate Resilience and Those with Lower Resilience

Adequate resilience: scoring 65 or higher in 14-item Resilience Scale; lower resilience: scoring lower than 65 in 14-item Resilience Scale.
Score of CES-D.
Score of PSWQ.
Score of ASQ.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study examined the cyclical psychopathology of PMDD by assessing the affective symptoms, emotional regulation levels, and psychological resilience levels of women with PMDD across different menstrual phases. Consistent with previous findings, the results reveal that women with PMDD exhibited significantly higher depression and anxiety scores compared with healthy controls across all menstrual phases, with peak symptom expression observed during the LL phase.1,2 These findings reinforce the notion that PMDD is characterized by phase-linked affective instability and that symptom remission after menstruation may be incomplete in women with comorbid anxiety or depressive disorders. 4
Emotional comorbidities and persistent emotional dysregulation
Previous studies have indicated that women with GAD or depressive disorders are at an increased risk of PMDD.4,5 Our study shows an association between GAD, depressive disorder, and PMDD and supports these previous results. According to the literature, fluctuations in hormones, including estrogen, serotonin, and hormones affecting the hypothalamic–pituitary–adrenal axis, can exacerbate the symptoms of anxiety and depression, highlighting a shared biological mechanism influencing GAD, MDD, and PMDD.19,20 In addition, our results extend prior work by comparing women with PMDD with and without emotional comorbidities. Specifically, women with both PMDD and emotional comorbidities (PMDD + C group) exhibited higher levels of depression and anxiety and lower levels of psychological resilience at baseline compared with women without such comorbidities. These findings are consistent with epidemiological evidence demonstrating a possible bidirectional relationship between PMDD and depressive disorders, wherein lifetime depression increases the risk of PMDD and PMDD increases the risk of recurrent mood episodes. 5 In particular, our within-subject analysis indicated that women with PMDD but without emotional comorbidities demonstrated clear premenstrual exacerbation, whereas women with comorbidities showed persistently strong affective symptoms across all menstrual phases.
Emotional dysregulation during the LL phase in women with PMDD
Women with PMDD experience an impairment in their cognitive reappraisal, which is an emotional regulation strategy that enables the modification of emotional responses under stress conditions. 21 In the present study, we used the ASQ, which is designed to determine how individuals regulate and respond to emotional situations in various contexts, such as during the menstrual cycle. Women with PMDD were found to have a lower capacity to adjust their emotional responses during the LL phase compared with healthy controls. Overall, these findings underscore the importance of developing tailored interventions aimed at enhancing the ability of women with PMDD to adjust their emotional responses.
Another notable finding of our study is that women with PMDD experienced a decline in their emotional regulation capacity during the ML phase, which preceded their depression and anxiety symptoms. This finding suggests that the capacity for emotional regulation decreases even before the exacerbation of PMDD symptoms. This exacerbation may be attributed to both intrinsic brain activity related to hormonal fluctuations and external stressors that contribute to emotional challenges in vulnerable populations. According to the literature, women with PMDD often exhibit hypoactivity in the dorsolateral prefrontal cortex, a brain region essential for emotional regulation, particularly when they are exposed to negative emotional stimuli during the premenstrual phase. 22 Difficulties in emotional regulation often emerge during the ML phase, when the levels of progesterone are elevated, suggesting that hormonal fluctuations impair emotional regulation even before the exacerbation of PMDD symptoms. 23 Women with PMDD often report major disruptions in personal relationships and daily functioning, which further affects their emotional capacity and regulatory abilities. 24 Negative interactions and emotional regulation impairments may amplify feelings of depression, anxiety, and emotional overload, facilitating the development of more severe PMDD symptoms with the progression of the menstrual cycle.
In this study, we observed that the deterioration of emotional regulation and psychological resilience was significant only in women with PMDD without emotional comorbidities, but not in those with such comorbidities. However, the scores for emotional regulation and psychological resilience during the PO, ML, and LL phases were lower in women with both PMDD and emotional comorbidities than in those without such comorbidities. Therefore, although the deterioration of emotional regulation and psychological resilience during the LL phase was not significant in women with both PMDD and emotional comorbidities, these women’s capacity for both emotional regulation and psychological resilience was significantly more impaired compared with those without such comorbidities.
Psychological resilience as a protective factor
As hypothesized in this study, higher levels of psychological resilience were significantly associated with lower levels of depression and anxiety in women with PMDD. Women with lower levels of psychological resilience were noted to experience higher levels of depression and anxiety across all menstrual phases. By contrast, women with higher levels of psychological resilience were observed to have a higher capacity for emotional regulation during the ML and LL phases. These results indicate that higher levels of psychological resilience are associated with a stronger capacity for maintaining or regaining mental health under stressful conditions. These findings are consistent with those of studies reporting that resilience-enhancing interventions can mitigate premenstrual symptom severity.10,11 Because psychological resilience is typically associated with cognitive flexibility and stress tolerance, 9 enhancing the ability of women with PMDD to cope with adversity and maintain their psychological well-being can enable them to better regulate their emotions during the luteal phase and can also mitigate their affective symptoms.
Clinical implications
Clinicians should routinely monitor for persistent emotional symptoms outside the luteal phase, particularly because these symptoms may reflect a comorbidity requiring an integrated treatment approach. In women with PMDD, the decline observed in emotional regulation and psychological resilience capacity, particularly during the LL phase, indicates that interventions aimed at enhancing adaptive emotional regulation (e.g., mindfulness and reappraisal training) may mitigate symptom exacerbation. Because psychological resilience serves as a robust protective factor across different menstrual phases, resilience training programs (e.g., stress management, self-efficacy enhancement, and psychoeducation) could serve as valuable adjuncts to conventional treatment strategies. Early identification of patients with low levels of psychological resilience or with emotional comorbidities may allow for the development of targeted interventions aimed at stabilizing affective fluctuations across the menstrual cycle.
Limitations
This study has three limitations that must be acknowledged. First, the number of participants was limited because of our requirement that women with PMDD demonstrate at least two prospectively confirmed symptomatic cycles. It likely selected a more consistently symptomatic subgroup; therefore, our findings may be more generalizable to women with consistent cyclic PMDD expression than to all individuals with PMDD in clinical settings. Second, because of the cross-sectional design of this study, we could not confirm a causal relationship between PMDD, GAD, depressive disorders, emotional regulation, and psychological resilience. Lastly, individuals who did not meet the inclusion criteria were excluded at the initial e-mail screening stage and were not recorded. The total number of excluded respondents at the screening stage could not be quantified, limiting our ability to fully evaluate potential selection bias in the recruitment process.
Conclusion
Emotional comorbidities such as GAD and MDD are highly common in women with PMDD. Women with emotional comorbidities typically exhibit persistently strong affective symptoms and low levels of psychological resilience, suggesting a trait-like vulnerability that extends beyond menstrual fluctuations. Both emotional regulation and psychological resilience contribute to individual differences in symptom severity and phase-linked variability. Hence, clinical interventions aimed at enhancing emotional regulation and psychological resilience skills may mitigate the emotional burden of PMDD. Overall, this study supports an interaction between hormonal and affective symptoms in PMDD.
Footnotes
Acknowledgments
This study was supported by grants from the National Science and Technology Council (NSTC112-2629-B-037-002, NSTC112-2314-B-037-042, and NSTC113-2629-B-037-002-MY2) and Kaohsiung Medical University Gangshan Hospital (KMGH-113R013).
Author Disclosure Statement
No competing financial interests exist.