
Abstract
Objective:
To find out the prevalence of adhesions, severity, and their relation to the current clinical scenario and to the type of previous surgery.
Methods and Materials:
A retrospective study of patients who already had different previous abdominopelvic surgery and subsequently underwent gynecological laparoscopic surgery for various indications. The patients’ clinical and operative notes were reviewed and analyzed.
Results:
There were 654 procedures performed. The most common indication for the laparoscopic surgery was secondary infertility 23.5%, followed by adnexal lesions 22.0% and primary infertility 19.6%. Intraoperative adhesions were found in 45.3%. Adhesions were deemed relevant to the clinical scenario in 21.3%. Patients who had a previous history of open (traditional) surgery were more likely to be found with adhesions in comparison with patients with history of laparoscopic surgery (odds ratio: 2.7, 95% confidence interval: 1.4–5.3, p = 0.0025). The presence of adhesions was found to be strongly associated with previous abdominopelvic surgery than non-abdominopelvic surgery (odds ratio: 4.3, p = 0.0078, 95% confidence interval: 1.5–12.5). The most common location of the adhesions was abdominal (36.1%), mixed abdominal and pelvic (35.1%), and pelvic adhesions (28.1%). Severe adhesions were found in 36.1%; 13.6% of converted laparoscopy to open surgery was due to adhesions. Cesarean sections were significantly associated with adhesions. Patients who had cesarean sections were more likely to have adhesions than those who had not (odds ratio: 5.7, 95% confidence interval: 3.8–8.6, p < 0.0001). Adhesiolysis was done without complications in 19.6% of patients with adhesions.
Conclusion:
Adhesions were prevalent in gynecological patients with previous abdominopelvic surgery. They were a significant contributor to the gynecological and reproductive issues. To minimize the risk of postoperative adhesions, laparoscopic approach should be encouraged instead of traditional surgery and rates of cesarean section should be reduced. Further high-quality studies are needed to establish conclusion and practical guidance toward the use of adhesion barriers.
Introduction
Postoperative adhesions, bands of connective tissue that join two normally separate anatomical structures, have become one of the commonest sequelae of 75 to 93% of gynecological surgeries, leading to chronic pain, infertility, or bowel obstruction.1,2 They are the result of surgical tissue trauma and healing. Adherence to microsurgical principles and minimally invasive surgery may help to decrease postoperative adhesions. 3 Evidence-based recommendations to reduce postsurgical adhesions in gynecological surgery allowed an improvement in the European surgeons’ knowledge and anti-adhesion strategies, as demonstrated in a survey performed in 2014. 4 The extent of the problem of adhesions has been underestimated by surgeons and the health authorities. There is rising evidence, however, that surgeons can take important steps to reduce the impact of adhesions. As well as improvements in surgical technique, developments in adhesion-reduction strategies and new agents offer a realistic possibility of reducing adhesion formation and improving outcomes for patients. 5 The reduction of the overall incidence of adhesions is essential for subsequent surgical treatments. Anti-adhesion strategies must be adopted for preventing the reoccurrence of adhesions after abdominopelvic operations. 6
Our primary objectives were to find out, in gynecological patients undergoing laparoscopic surgery, the prevalence of adhesions, severity, and their relation to clinical indication and to the type of previous different surgical operations.
Secondary objectives were to find out the risk of developing surgical adhesions after different surgical operations, the type of adhesions in relation to the previous surgical operations, and to compare laparoscopic and traditional surgery regarding the risk of adhesion formation.
This study emphasized the importance of considering adhesions as a cause of morbidity and encourages surgeons to deal with them during laparoscopy.
Materials and methods
This was a retrospective study at Jordan University Hospital, a teaching academic hospital. All women operated upon in the gynecological department with laparoscopy (diagnostic and operative) for various indications in the period March 2015 and March 2019 were included. We collected demographic data including age, past history including past surgical history (types of surgical operations and indications), and clinical symptoms. We studied patients with previous surgical operations that involved abdominopelvic surgeries or cesarean section(s). Although cesarean section was regarded as an abdominopelvic surgery, patients with previous cesarean section were studied alone as this type of surgery had almost a standard and uniform technique, while abdominopelvic surgeries were diverse surgical procedures with different indications, techniques, and complications. Abdominopelvic surgeries, whether laparoscopic or traditional surgery, included appendectomy, myomectomy, adnexal surgery, ectopic pregnancy, and cholecystectomy. Intraoperative reports of adhesions were noted and analyzed as reported regarding their type (thin or thick) – filmy adhesions were regarded as thin, while thick fibrous bands were regarded as thick adhesions – location, and severity and whether they were relevant to the patients’ symptoms. The criteria used for the relevance of adhesions to the clinical picture were the patients’ complaints, location of the adhesions, the pelvic organs that were involved in the adhesions, and the judgment of the operating consultant. This relation was substantiated further by another consultant gynecologist’s second opinion who reviewed the clinical case scenario and any improvement in the clinical symptoms after adhesiolysis. We did not use a formal scoring system for the severity of the adhesions. The adhesions were deemed mild if they involved only one abdominopelvic organ with no obliteration of spaces or obstruction of the fallopian tubes. Severe adhesions were those involving two or more organs with or without obliteration of a space or tubal blockage. Abdominopelvic organs included bowel, liver, uterus, tubes, ovaries, and peritoneum. We found out whether adhesiolysis was done or not and whether adhesion barriers were used or not. Rate of conversion to laparotomy was calculated and whether the surgical adhesions were the indication for conversion. We also related the risk of developing adhesions to the type of abdominopelvic surgery. We compared the risk of developing adhesions between laparoscopic versus open (traditional) surgery.
The data sources were the patients’ electronic files, clinic, operative, and postoperative notes. Gynecological oncology patients were excluded.
The study obtained the institutional review board (IRB) approval at Jordan University Hospital decision number 126/2019, dated 14 May 2019.
The statistical analysis was performed with the Data Toolkit in Excel (Microsoft, Redmond, WA, USA) using descriptive analysis. Relative risk and 95% confidence intervals (CIs) were also calculated to compare variables. The obtained data were examined using a frequency table and are presented as frequency, percentage, and mean. All patients’ data were copied onto an Excel sheet after collection, where a pivot table was applied. The main point of splitting our data was – ‘patients with adhesions’ versus ‘patients without adhesions’ – in order to study predisposing factors or surgeries performed. Data Toolkit in Excel was used to determine the t test for comparing the difference in the mean age between adhesion and non-adhesion groups, where significant value was taken as <0.05. All other factors studied in Tables 1, 2, 4, and 5 were studied in the form of an odds ratio. We used a formula template and the Data Toolkit to calculate each odds ratio, 95% CI, and p value. Table 3 was calculated as simple descriptive statistics.
Comparison of adhesions versus no adhesions in relation to patients’ demographics, previous medical and surgical history.

AP, abdominopelvic; CI, confidence interval; CS, cesarean section; D&C/E, dilatation and curettage or evacuation; D&E, dilatation and evacuation; Hx, history; SD, standard deviation. Bold value indicate p values.
Results
After excluding those with undocumented adhesion status, there were 654 patients reviewed. There were 296 patients with adhesions and 358 patients without adhesions. There were no differences in the prevalence of adhesions regarding age, parity, previous history of miscarriage, and past medical history (Table 1).
Compared with patients with no previous surgical history, presence of previous surgical history was significantly associated with adhesions (odds ratio: 4.2, p < 0.0001, 95% CI: 3–6; Table 1). Compared with those who had no previous surgical history, patients with previous abdominopelvic surgery had significantly more adhesions (odds ratio: 4.3, p = 0.0078, 95% CI: 1.5–12.5; Table 1). Compared with patients who did not have a history of ectopic pregnancy, patients who had a history were 2.5 times more likely to be found with adhesions (Table 1).
The most common indication for the laparoscopic surgery was secondary infertility (154 patients) followed by adnexal lesions (145) patients and primary infertility (128) patients. There were many other rare indications in 26 patients including amenorrhea, dysmenorrhea, dyspareunia, pelvic inflammatory disease (PID), endometrioma, acute pelvic pain, and so on (Table 2).
Indications and gynecological laparoscopic operations performed.

CI, confidence interval; IUCD, intra-uterine contraceptive device; LAVH, laparoscopic assisted vaginal hysterectomy; TLHBSO, total laparoscopic hysterectomy-bilateral salpingo-oophorectomy. Bold value indicate p values.
Regarding the prevalence of adhesions in relation to the clinical indication for laparoscopic surgery, adhesions showed a statistically significant association with secondary infertility (p = 0.0001). The odds of secondary infertility as an indication was 2.1 times more likely in patients with adhesions than patients without. Absence of adhesions was more likely with primary infertility, ectopic pregnancy, and chronic pelvic pain (p values were 0.0034, 0.0067, and 0.0002, respectively; Table 2). The odds of ectopic pregnancy as an indication was half as likely in patients with adhesions than patients without. Adhesions were not found to be significantly associated with the other laparoscopic gynecological surgery indications (Table 2).
The most common laparoscopic gynecological surgery performed in our patients was diagnostic laparoscopy, laparoscopic ovarian cystectomy, laparoscopic adhesiolysis, and laparoscopic tubal ligation. None of the types of surgeries we performed was more commonly performed in patients with adhesions in comparison with patients without adhesions (Table 2).
Intraoperative adhesions were found in 296 patients (45.1%). These adhesions were described as thick in 104 patients (35.1%) and severe in 107 patients (36.1%) (Table 3).
Intraoperative adhesions (type, severity, relation to patients’ symptoms, and location).

Of the patients who had a history of cesarean section and were found to have adhesions, 72.4% had only cesarean section and 85.4% had other abdominopelvic surgeries too. There was no statistically significant difference (odds ratio: 0.5, 95% CI: 0.2–1.2, p = 0.102) (Table 4).
Presence and absence of adhesions in relation to history of different surgical operations.
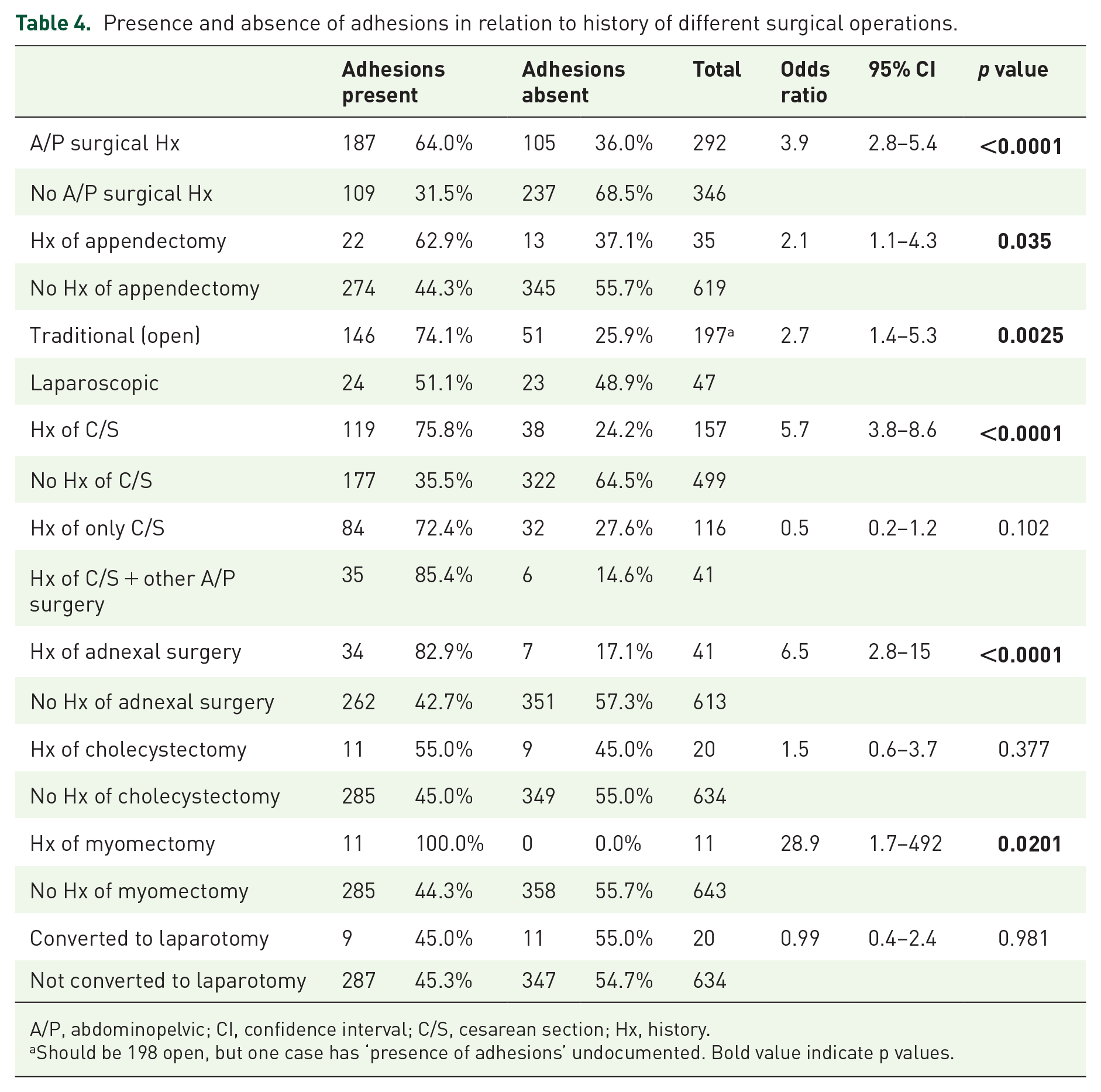
A/P, abdominopelvic; CI, confidence interval; C/S, cesarean section; Hx, history.
Should be 198 open, but one case has ‘presence of adhesions’ undocumented. Bold value indicate p values.
Adhesiolysis was performed in 58 patients (8.9% of the total number of patients or 19.6% of patients found to have intraoperative adhesions). The clinical scenario was deemed related to the adhesions in 63 patients (21.3%), while in 230 patients (77.7%) who were found to have adhesions; these adhesions were judged to be irrelevant to their clinical picture (the symptoms were not related to the adhesions; Table 3).
The most common location of the adhesions was abdominal (36.1%). Among the abdominal adhesions, 17.9% were involving the bowel. The second-most common location of the adhesions was mixed abdominal and pelvic (35.1%). Pelvic adhesions were seen in (28.1%). Adhesions involving the uterus were the commonest pelvic adhesions (11.1%) (Table 3).
Of all the laparoscopic procedures that were performed, 22 were converted to laparotomy. Of those, nine cases (40.9%) had intraoperative adhesions. In the converted cases, the indications for conversion were the presence of adhesions in 13.6%. Two of these 22 cases had undocumented state of adhesions. However, we found no significant difference in this conversion rate in patients with adhesions compared with patients with no adhesions (odds ratio: 0.99, 95% CI: 0.4–2.4, p = 0.981).
Of the 292 with previous abdominal/pelvic surgi-cal history, 64% were found to have adhesions. Patients who had a history of abdominal/pelvic surgery were 3.9 times more likely to be found with adhesions than without adhesions (p < 0.0001, 95% CI: 2.8–5.4; Table 4).
Patients who had a history of appendectomy were found to be at higher chance to have adhesions than those who had non-appendectomy abdominopelvic surgery (odds ratio 2.1, 95% CI: 1.1–4.3, p = 0.035; Table 4). We calculated the same ratio for patients who had an open versus laparoscopic appendectomy and reached an insignificant result.
Regarding adnexal surgery, the risk of adhesions for a patient with a history of adnexal surgery was statistically significantly more than those with no history of adnexal surgery (odds ratio: 6.5, 95% CI: 2.8–15, p < 0.0001; Table 4).
However, there was statistically significant risk of adhesions for open versus laparoscopic adnexal surgery.
Of the 20 patients who had a history of cholecystectomy, none of which were open cholecystectomies, 55% were found to have adhesions. However, there was no statistically significant difference in the presence or absence of a history of cholecystectomy in patients with adhesions (Table 4).
The odds ratio of developing adhesions for a patient with history of laparoscopic cholecystectomy versus no previous surgical history was 1.8 (95% CI: 1.1–2.7). A total of 91.7% of those who had open myomectomy were found to have adhesions. We found that the odds of having a previous history of myomectomy was 28.9 times higher in patients with adhesions (Table 4).
Of the 157 patients who have had cesarean sections, 75.8% (119) were found to have adhesions. Patients who had cesarean sections were more likely to have adhesions than those who had not had cesarean sections (odds ratio: 5.7, 95% CI: 3.8–8.7, p < 0.0001), a statistically significant risk (Table 4). Of all the patients with adhesions who had a history of cesarean section (isolated or among other abdominopelvic surgeries), 70.5% had only cesarean section and 29.5% had other abdominopelvic surgeries too.
We further studied the prevalence of adhesions in relation to the number of previous cesareans; patients with previous two to four cesareans are 1.3 times more likely to have adhesions than those who had only one previous cesarean (odds ratio: 1.3, 95% CI: 1.1–1.6). Furthermore, compared with those who had less than four cesarean sections, patients who had more than four previous cesarean sections were 1.33 times more likely to have adhesions (odds ratio: 1.3, 95% CI: 1.2–1.5).
Patients who had a previous history of open (traditional) surgery were more likely to be found with adhesions in comparison with patients with history of laparoscopic surgery (odds ratio: 2.7, 95% CI: 1.4–5.3, p = 0.0025; Table 4).
We could not find adhesion barrier use in our patients in both laparoscopic and open surgery.
There were only 169 cases with documentation of the type of adhesions (thick/thin).
We found there was no statistically significant difference in the types of adhesions in relation to the types of previous abdominopelvic surgical history (laparoscopic versus open/mixed; odds ratio: 1.1, 95% CI: 0.5–2.6, p = 0.87; Table 5).
Types of adhesions (thin or thick) and the types of previous surgical history (laparoscopic versus open and mixed).
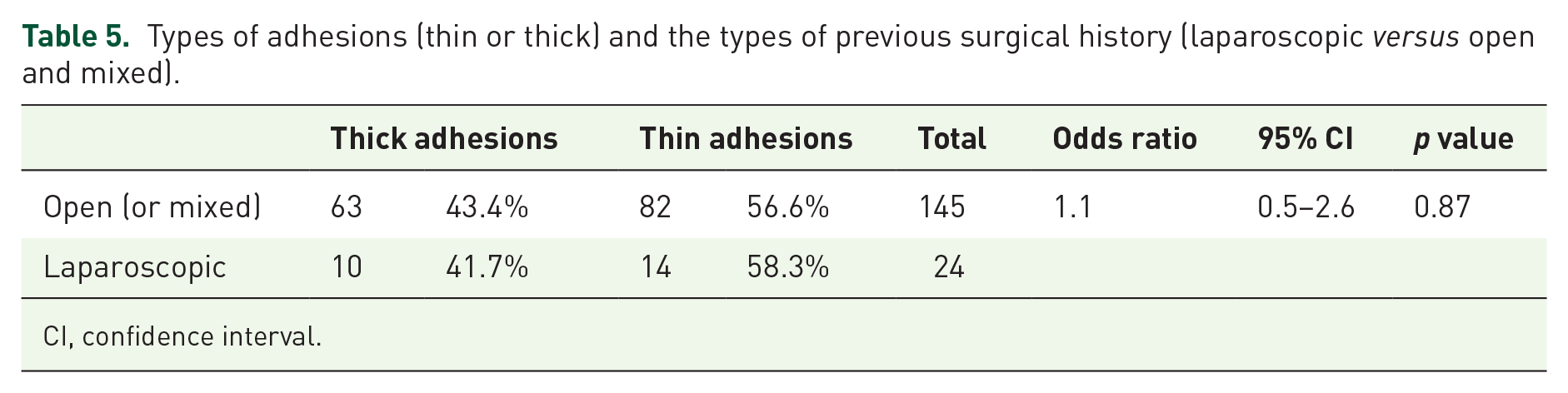
CI, confidence interval.
Discussion
Postoperative adhesions occur after most surgical intra-abdominal procedures. 7 Our patients had a previous surgical history in 47.3%. In total, 94.50% of them had abdominal and/or pelvic surgery. The risk of postoperative abdominopelvic adhesions following open surgery was found to be 34%, 8 40.6%, 9 and 50%. 10 In our study, the overall risk of adhesions was 45.1%. Moreover, we found that women with previous abdominopelvic surgery were 4.3 times more likely to have adhesions than those without.
We found that 75.8% of women with history of previous cesarean section had postoperative adhesions. Compared with those who had no previous cesarean, the odds ratio in our study to have post-cesarean section adhesions was 5.7. Similarly, Hesselman and colleagues 11 found that adhesions were present in 37% of women with previous history of cesarean, compared with 10% of women with no previous cesarean with an odds ratio 5.2. They also found that adhesions increased with age (⩾35 years) and the number of cesarean sections: 32% after one; 42% after two, and 59% after three or more. Only 2.5% of our patients had five or more cesarean sections and the mean age of our patients with adhesions was 34.3 years. The high rate of post-cesarean section adhesions in our study could be due to the fact that most cesarean sections in our patients were done by residents in training.
We found that the rates of postoperative adhesions were 74.1% and 51% in patients with previous open and laparoscopic surgery, respectively. In a survey and literature review by Hackethal and colleagues, 12 the risk of adhesion formation was widely underestimated and laparoscopy resulted in less adhesion than laparotomy.
The indications of the gynecological laparoscopic surgery in our study were mostly reproduction related. Those patients had both gynecological and non-gynecological operations. Previous appendectomy was threefold more prevalent in women seeking fertility treatment than the general population because of intra-abdominal adhesions. 13 Different surgical operations may lead to intra-abdominal adhesions and, thus, to dysfunction of the fallopian tube.14,15 Ikechebelu and colleagues 16 found that the prevalence of adhesions after open myomectomy was 80.2% versus 20.3% in the control (odds ratio: 15.9, p < 0.001) and adhesions are statistically higher at the uterus (68.6%), fallopian tubes (77.7%), ovaries (62.8%), and bowel 53.7%. In our study, uterine adhesions were found in 11.1% and bowel adhesions were seen in 17.9%. In our study, open myomectomy was associated with an odds ratio of 2.9 for developing adhesions. The differences in our results from theirs were obviously due to the various surgical operations history in our study. Moreover, all our cholecystectomy cases were laparoscopic.
Of those converted to laparotomy, 40.9% had intraoperative adhesions; only in three cases (13.6%), the adhesions were the indication of conversion. Lim and colleagues 17 found that conversion to laparotomy of laparoscopic hysterectomy was associated with moderate or severe adhesive disease and increased specimen weight. Twijnstra and colleagues 18 studied age, uterine weight, and body mass index (BMI) but not adhesions as a risk factor of conversion. Driessen and colleagues 19 in a systematic review identified adhesions as a predictor of longer operative time, complications, and conversion in laparoscopic hysterectomy.
We performed laparoscopic adhesiolysis for various indications without intraoperative complications or postoperative morbidity. Adhesion barriers were not used in these cases. Molegraaf and colleagues 20 found that laparoscopic adhesiolysis in a randomized clinical trial in patients with abdominal pain attributed to adhesions was less beneficial than laparoscopy alone in the long term and adhesiolysis was associated with an increased risk of operative complications. Van den Beukel and colleagues 21 in a systematic review and meta-analysis found that laparoscopic adhesiolysis reduces pain from adhesions in 70% of patients in the short term but there was little evidence to support routine use of adhesiolysis in treatment for chronic pain. In total, 36.8% of patients with adhesions had no abdominal and/or pelvic surgery. In these patients, there could be various causes of their adhesions. 22 Adhesion barriers were not used at our hospital. Ten Broek and colleagues 23 in a systemic review and meta-analysis of the benefits and harms of their use found that oxidized regenerated cellulose and hyaluronate carboxymethyl cellulose could safely reduce clinically relevant consequences of adhesions. An overview of Cochrane reviews by Hindocha and colleagues 24 found insufficient evidence to withdraw any conclusions about the effectiveness and safety of anti-adhesion agents in gynecological surgery. Furthermore, Farag and colleagues 25 in a systematic review of management, prevention, and sequelae of adhesions concluded that there was a need for high-quality trials to evaluate the efficacy of surgical techniques, adhesion barriers, and other treatment modalities.
Our study had the strength of the relatively large number of patients combined with laparoscopic identification of the surgical adhesions.
The limitations of our study were that it was a retrospective study and it included patients who had various previous abdominopelvic operations. We recommend studying prospectively individual abdominopelvic surgeries, laparoscopic or traditional surgery, to identify the risk of adhesion formation.
Conclusion
Adhesions were prevalent in gynecological patients with previous abdominopelvic surgery. They were a significant contributor to the gynecological and reproductive issues. To minimize the risk of postoperative adhesions, laparoscopic approach should be encouraged instead of traditional surgery and rates of cesarean section should be reduced. Further high-quality studies are needed to establish conclusion and practical guidance toward the use of adhesion barriers.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.