
Abstract
Background:
The United States has one of the highest cesarean section (c-sections) rates among high-income countries. Birthing people who self-report as Black women in the United States are not only are three to four times more likely to die from preventable prenatal challenges, but also are the most prevalent racial group to receive either planned or unplanned c-sections.
Objectives:
Our initial aim focused on the lived experiences of prenatal care and the variety of birth types among Black women that was analyzed for a prior publication. In this secondary analysis, we noticed there was a large portion of study participants who discussed their perceptions of cesarean births.
Design:
In this specific analysis and due to c-section prevalence among Black women, we solely focused on the perceptions of c-sections, whether of planned or unplanned mode of delivery.
Methods:
We analyzed interviews from 25 women in the South Florida region of the United States who had at least one recent pregnancy and/or birth of a living child (<24 months) at the time of data collection. Data were thematically analyzed and coded using NVIVO 12 software by our research team.
Results:
Nineteen Black women had high-risk prenatal status, with n = 15 of the 25 Black women having c-sections. Regardless of whether c-sections were planned or unplanned, perceptions of c-sections were expressed as traumatizing and coercive. We also noticed how participants described their experiences with intergenerational trauma from the collective memory and triggers of their familial social groups who also had adverse experiences with c-sections. Participants who desired vaginal-births-after-cesarean sections or wanted to incorporate approaches with midwives or doulas further experienced constrained choices due to their high-risk prenatal diagnosis and limited insurance coverage. Based on our results, we designed a conceptual model to illustrate how our findings can be applied to better understand the overlap between medical racism and obstetric racism, which has implications for the perpetuation of unwarranted c-sections, high-risk pregnancies, negative mental health issues, and racial birth trauma.
Conclusion:
Social factors, including medical racism, contribute to obstetric racism and racial birth trauma throughout postpartum and impact mental health.
“Shalon Irving didn’t feel right. There were red flags. First, a painful, tender lump formed along her c-section incision, requiring lancing and draining. Then came alarming spikes in her blood pressure. A nurse who made visits to Irving’s Atlanta home to treat her incision every other day recorded a dangerously high blood pressure of 174 over 118. The new mother suffered chronic pain, persistent headaches, and swellings in her legs. She had had a complicated journey to pregnancy, with several years of fertility difficulties, a blood clotting disorder, and surgery to treat uterine fibroids. Her health history, coupled with the known risks of postpartum hypertension and peripartum heart failure among Black mothers, indicated Irving might require close monitoring and follow-up care after giving birth . . . [On Jan. 24, 2017], Irving collapsed in her home from cardiac arrest and was rushed to the hospital, where she was removed from life support a week later. An independent autopsy her mother ordered showed that Irving had died from complications of high blood pressure.” (Cruickshank
1
)
Introduction
The performance of cesarean-sections (c-sections), are steadily increasing in U.S. hospitals, regardless of high- risk prenatal status. Not only does the United States have one of the highest c-sections rates among high-income countries, but also over one in every three live births were delivered via c-section in 2022, 2 making c-section deliveries the designated birth type across majority of U.S. hospitals. A C-section, a surgical procedure in which the placenta is removed from the abdomen’s uterus via abdominal incision, 3 has a fundamentally troubling history in the United States.4,5 C-section surgical techniques often can be lifesaving in some medical circumstances. White male doctors, however, conventionally performed and perfected the process of c-sections on enslaved Black women’s bodies without anesthesia, or pain medicine, or without their informed consent,5,6 and supported by the fundamental eugenic ideology that Black women were property and thus were not human enough to feel pain. 6 This stark medical history of c-sections is what makes this birthing procedure one that needs critical investigation, particularly as there is an increase of c-sections, whether planned or unplanned, among racially minoritized populations.
Birthing people who self-report as Black women in the United States are the most prevalent racial group to receive c-sections even though Black women only account for 15% of deliveries in the U.S. population.3,7 Black women are also three to four times more likely to die from preventable pregnancy-related complications, 8 and these reproductive health inequities are fundamentally driven by structural racism and thus have become a public health crisis. 4 Not only are Black women 243% more likely to experience prenatal morbidity and mortality,9–11 but also Black women have the highest total c-section rate out of all racial/ethnic groups. Black women’s c-section rates are higher than White groups (30.7%), American Indian and Alaska Native groups (28.9%), and Asian groups (32.7%)12,13,14 at 35.9%, 15 which is higher than the national average c-section rate of 31.7%. To better understand the persistence of reproductive inequities, we sought to examine Black women’s perceptions of c-sections.
Recent news in the U.S. public media also claimed that the leading reason for c-sections has been to fill operating rooms. 16 Prevalence of c-sections among Black women, we acknowledge, is not entirely due to high-risk prenatal status (high-risk prenatal status is also an elusive factor that can change throughout the peripartum period and is further complicated by the lack of standardized risk assessment models or tools to address risk of maternal mortality 14 ; e.g., emergency-related labor and delivery complications). We recognize, however, that women with low-risk prenatal status may self-elect to have a c-section for non-emergencies,17,18 particularly as “scheduling” trends also advance.17,19 Although these trends for “scheduling” and self-election are plausible considerations, that is not the focus of our study. Rather, we investigate the lived experience and perception of c-sections among Black women, whether planned or unplanned. Therefore, we sought to investigate: (1) how Black women perceive c-sections; and (2) whether lived experiences can help us to discover additional pathways for understanding racial trauma and mental health, particularly as this is a neglected area in maternal health research.
Methods
Recruitment
Eligible study participants met the following inclusion criteria: (1) self-identified as Black women, (2) adults (18 and older) who can provide either optional written or verbal consent, (3) not currently pregnant at the time of the study, (4) not presently involved with any correctional facilities (e.g., not incarcerated or on probation or parole at the time of the interview), and (5) must have had at least one pregnancy regardless of birth outcome (e.g., pregnancy loss, stillbirth, or birth of a living-child is less than 2 years of age). At the time of data collection (and due to time constraints), while some women did mention miscarriages and pregnancy losses, we only focused our analysis on the lived experiences among Black women who had given birth to a living child (24 months or less in age).
To reduce recruitment bias, we recruited Black women who experienced a variety of birth types. However, during the data analysis, we noticed a large pattern of Black women who received c-sections, which is why we wanted to isolate this pattern and explore this thread in our data. The observations on the lived experiences of c-sections became a latent result from our primary data collection. Participants were recruited via respondent driven referrals as well as purposive and referral sampling, which served as a triangulation recruitment strategy, allowing the researcher and/or participants to make recommendations of other potential persons to be interviewed. 20 In other words, referral sampling, in this aim, was rooted in a purposive sampling strategy as an attempt to be intentional about recruiting among populations that are often hesitant to trust researchers with their lived experiences. Referral-sampling techniques, such as asking a variety of women within the University of Miami network for referrals and recommendations, were employed. Black women who self-identified as Black, African, African American, Caribbean, Biracial, Mixed Race, and/or Afro-Latina or Black Hispanics were included in this study sample to capture the wide variety of ethnicities within Black womanhood.
We intentionally decided to exclude recruiting at the sites of hospitals, maternity centers, and biomedical facilities, so as not to give the impression of institutional advocacy and/or partisan partnerships. This distinction is important because it aims to reduce the potential stigmatization that may arise during the interview process if a study participant decides to share experiences using midwifery or holistic health approaches, rather than biomedical interventions. 21
Data collection
The data were collected in 2019; and thus, we note that COVID-19 significantly delayed our data analysis, which explains our 5-year lapse. We should also note that this dataset initially focused on a broad variety of Black women’s lived experiences with a wide array of birth types published on in a prior publication. 10 As of 2020 and since COVID-19, the trend of maternal morbidity, mortality, and medically unnecessary c-sections among Black women have since increased and have been exacerbated since COVID-19. 16 Thus, the data capture a small snapshot on the rise of this prevalence.
Data analysis
We are aware of postpartum health experiences; however, this study initially focused on pregnancy and birth experiences among Black women as the core component of its study scope. Our methods focused on the lived experiences of the patient; thus, we intentionally asked the participant to describe how they went about finding or requesting their clinicians of choice, while allowing the participant to opt out of sharing this information (and/or to tell us as much they were comfortable with sharing) solely during the reflections of their pregnancy and birth experiences.
C-sections were not the sole focus of birth type in our recruitment process. Rather, in our initial data collection, we requested and recruited on a wide range of birth types. Please note, however, because we noticed that c-sections were more prevalent in our primary analysis, we decided to build upon our data analysis by solely focusing on the lived experiences of c-section birth types in this secondary analysis. Study participants were required to have at least given birth to one living infant (less than 24 months of age) at the time of data collection we focused on their prior birth experiences. In other words, we did not necessarily require the respondent to have prior formal knowledge of a c-section to birth or any birth type (e.g., some did take birth classes, and some did not). Rather, we focused on their own lived experience as a substantial form of patients having and expressing legitimate scientific knowledge of their own bodies. Many of the study participants did express having prior birth expectations to have an unmedicated or nonintervention birth (e.g., vaginal non-epidural, water birth, with a midwife or doula). But, and in many cases, these expectations were not met due to other factors, such as emergencies, insurance changes, clinician, and/or provider changes. We captured these as unplanned c-sections. Planned c-sections were captured when participants specifically desired a c-section regardless of prenatal risk status. We use the technical definition of high-risk as someone who has pre-existing medical conditions from a medical diagnosis and under activity restriction during their trimesters, may have preterm ruptures of the placenta, fetal growth delays, and/or required to have special monitoring, or surgical processes in a hospital setting. 22
Interview duration was approximately 60–120 min and was conducted at the location of the participant’s preference. To address validity, it is most effective if interviews are conducted where respondents have options to suggest where they feel the most comfortable to share narratives and testimonials.10,21,23,24 The study participants had the option to conduct their interview in the location of their choice. In some cases, the respondent preferred phone interviews or to be in the comfort of their own homes or even at beauty salons or daycare centers. The rationale for this aspect was to go where the respondents felt most inclined to feel comfortable sharing their story.
We acknowledged that we followed the relevant qualitative data reporting guidelines, as stated by the “Checklist for Reporting Qualitative Research,” known as the COREQ guidelines. For example, the reporting of this study conforms to the COREQ guidelines to ensure reliability of our reporting as cited within these referenced articles.25,26 Thus, for the purposes of the COREQ guidelines and for transparency when conducting qualitative research, it is important to mention some personal aspects of the research team. All interviews were conducted by the first author of this study, particularly since this initial data collection stemmed from the first author’s PhD dissertation collection (completed in 2019–2020) at the University of Miami. The first author (who is currently an Assistant Professor at the Ohio State University, College of Medicine) has since shared this data collection with the following coauthors (research team) of this study for secondary analysis. This dataset originally derived from the first author’s dissertation, in which she obtained her PhD from the University of Miami, and she also identifies as a South Florida native. The third author also attended University of Miami and was a South Florida pre-med student. Our network affiliations aided the recruitment strategy, specifically regarding cultivating a respondent driven recruitment strategy among Black women who have given birth in the South Florida region of the U.S. context. For example, the research team consists of four research scientists (including the first author) who self-report as Black women and one research assistant who self-reports as a White woman. The research team members are at various stages of their research careers (e.g., an associate professor with tenure, a postdoctoral fellow, and one research associate; and one research assistant), all of whom focus on maternal-and-child health research across biomedical disciplines and across wide-ranging capacities.
The interview protocol was designed to address two phases that divide the data collection into (1) pregnancy/prenatal care and (2) birthing/labor and delivery. Demographic information was collected about the participants, including self-identified racial background (self-reported), date of birth, number of births, type of birth (e.g., vaginal delivery or cesarean section), type of health insurance, birth weight of infant, type of provider, and duration of labor. The interview protocol was based on six broad phenomenological questions: “Tell me about your most recent pregnancy”; “Tell me about your prenatal care”; “What were your experiences with the person(s) involved in your care?”; “Tell me about the place where you gave birth”; “What were your experiences like being a Black woman (and / or being perceived as a Black woman) with the providers in your care?”; and “Tell me about your care experiences of being pregnant and giving birth in South Florida?” We inquired into more examples through probes regarding how the respondents went interpreted meaning at their clinical encounters or requested by their clinicians, including midwives and doulas.
Data analysis
The codebook was developed at the University of Miami. The data analysis was conducted during the first author’s fellowship at Harvard University, School of Public Health. The first author is currently an Assistant Professor at the Ohio State University, College of Medicine. The data were analyzed thematically analyzed and coded using NVIVO 12 software by our research team and two research assistants helped quality check coding for inter-reliability. Data analysis consisted of coding the transcriptions (and listening to the audio files) of the interviews, 24 in a thematic analytical process as well as drawing from the literature to substantiate coding themes. Additionally, we randomly selected study participants and invited them to review their respective patient transcript to ensure reliability. The content of the transcriptions was validated through a quality check process conducted by our research team and coauthors. Data were analyzed using phenomenological methods as a qualitative process. Phenomenology draws upon principles of narrative medicine which focus on the fundamental premise that the lived experiences of patients are substantial evidence for legitimate scientific data about one’s perception of their health condition. Field notes were made during and after each interview for the data analysis process. Data saturation was reached with the target amount of recruiting 25 respondents. Themes were derived after the initial data analysis, as this was a secondary analysis.
Ethical approval
The Institutional Review Board at the University of Miami approved this study in June 2018 (IRB #20180221). The continuing report approval was added in June 2019–2020 (CR#00010707). Both written and verbal consents were approved by the IRB. Field work and data collection were completed between January and July 2019. Informed consent was obtained in either verbal or written format, with an option for verbal consent from the study participants. Verbal consent was taken as optional. Many of our study participants preferred verbal consent, since they had given birth about 24 months prior, at the time of data collection, and were often busy with recovery and caretaking. Names of study participants were deidentified for the protection and honor of the study participants who shared such personal perceptions.
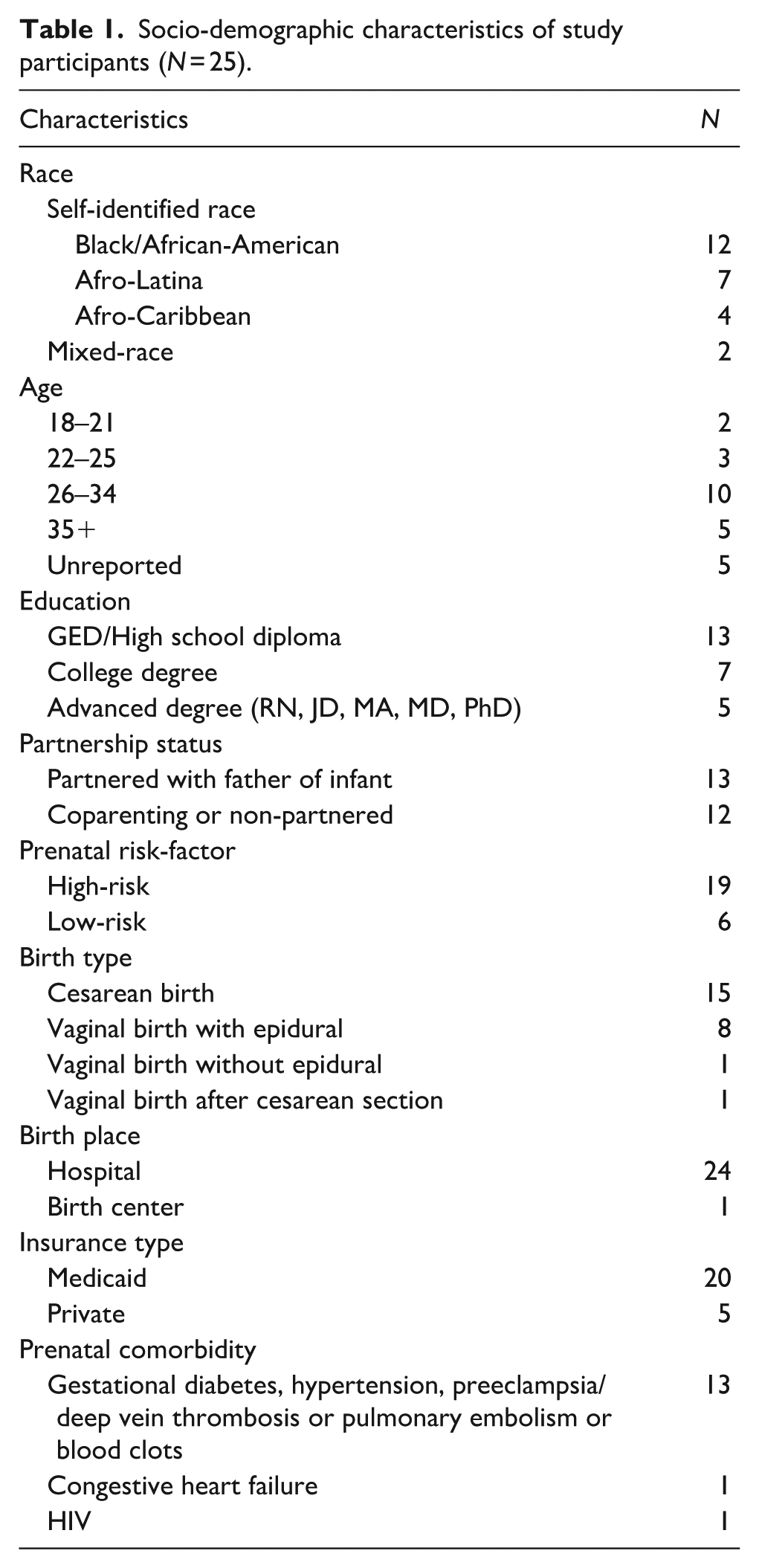
Table 1 illustrates the sociodemographic characteristics of the study participants.
Socio-demographic characteristics of study participants (N = 25).
Results
Twenty-five respondents consented to complete the interview process, with no dropouts from the study. Nineteen of the 25 study participants self-reported high-risk prenatal complications. Ten of the participants stated maternal age as 35 years or older (e.g., some studies have examined how maternal age increases high-risk prenatal complications due to bodily “weathering.”) 27 No follow-up interviews were needed or carried out, as respondents reported feeling comfortable sharing their responses and approving of their respective deidentified transcript file.
Since these interviews were based on self-reflections of their prior pregnancies and birth experiences, we allowed study participants to self-report if they received high-risk prenatal diagnosis or low-risk prenatal diagnosis, and for them to describe to us (as researchers) their interpretation of such determinations in their own words. We noticed that regardless of having a low-risk or high-risk pregnancy, respondents still expressed experiencing adversity, discrimination, and trauma during clinical encounters. Our results also showed how participants described their perception of the rationale for having c-section. In cases of emergency or unplanned c-sections, the rationale was based on what is best for the fetus. Our aim, however, was to focus on the mother’s perceptions because the mother’s perception is often neglected. Thus, even if the c-section was necessary to save both the mother and fetus, our results showed how Black women still experienced racial discrimination, stigmatization, stereotypes, and biases at clinical encounters.
Figure 1 also illustrates a conceptual model of our results with special consideration to the lived experience of race and racism were intersected with maternal-aging 27 on allostatic loads. 28 High-risk prenatal complications among the study participants were specifically self-reported as gestational diabetes, hypertension, preeclampsia, or blood clots. One participant discussed having congestive heart failure and another participant reported contracting HIV during the second trimester. Among these high-risk prenatal complications, 15 of the 25 study participants had c-sections. We also did not collect data on obesity or BMIs; however, we did allow the participants to describe any pre-existing health conditions or concurrent prenatal conditions through their lived experiences. Though both vaginal and c-section births were represented among study participants, all participants discussed their perspectives of c-sections either directly happening during their birth experience or indirectly from another’s individual personal narrative.

A conceptual model for illustrating the overlap between medical racism and obstetric racism on racialized birth trauma.
To better understand how patients define and describe such conditions in their social world, we allowed the participants to self-report on how they defined and named their high-risk or low-risk prenatal diagnosis, using their own words.
Eight themes from the interviews are reported (see Table 2), in the viewpoint of the study participants (acronym as SP).
Summary of results.

VBAC: vaginal birth after cesarean.
C-sections described as “cutting on”
We observed that respondents described c-sections as “cutting on,” or “being cut on,” representing how the body “goes under the knife.” We noticed study participants used the word “cut” in reference to cesarean section, and in doing so they named how the body is literally cut open for the fetus to be delivered. Thus, we use this language interchangeably with obstetric terminology to capture the perceptions of c-sections at the micro-level of analysis as the patient’s perspective.
One participant shared her perception of the financial incentives that she perceives as the underlying “agenda” for the stark incline of c-sections, stating: Cutting is a business. These doctors think they have to work fast and get to their next patient. They cut and get them babies up out of you.—SP7
This same study participant shared how the birthing techniques used to handle her high-risk circumstance during delivery at a birthing center differed from how she perceived them in a hospital-setting, stating: But the birthing center went out of their way to find other methods [to prevent a c-section]. Natural methods to get the body naturally functioning again without having to cut.—SP7
Social stressors that contribute to prenatal stress
Additional social stressors outside of the clinical encounter also show up during viewpoints of the prenatal care experience. This is particularly important for Black women dealing with high-risk prenatal status and exposure.
My child’s father was dealing with being incarcerated and the police. Helping him and our family made my pregnancy so stressful, I could not sleep wondering if we would be ok.—SP4 I was evicted during my 1st trimester. There was no way I could tell my doctor that we were staying with different relatives every other week. —SP25 Dealing with domestic violence and I kept wondering if I would lose my pregnancy. I cried almost every night.—SP6
Lapse in communication between doctors
A vaginal delivery was requested by this study participant (in which her female-OBGYN supported the request). This request was, however, overridden by the senior (White male) physician, who supervised physicians (to whom the female-OBGYN reported). This sudden clinical/surgical decision was also not communicated to the patient, until the day of her birth, which triggered additional trauma.
I had a fibroid that had to get removed during my birth, which was a part of the plan. I knew that they would be cutting me open to remove the fibroid and that I would still be able to have the VBAC. But somewhere along the way, the senior male doctor made the decision to tell my OBGYN that I should have a c-section, and they told me this at the last minute.—SP1
Intergenerational role of race and racism
The prevalence of c-section deliveries also spanned across several members of the family lineage, as evidence of intergenerational reproductive health disparities. Patient-perceptions on the reasons why Black women are more likely to be susceptible to high-risk prenatal status and c-sections were described as influenced by additional social factors, such as socioeconomic status, biases in nationality, and implicit biases.
I feel like when doctors see Black women—they are always ready to cut on us [c-section] and make a dollar because of the money and there is no way that should be the case. Because in these birthing centers, you have more White women from foreign [countries] and from all around the world, like from Europe, to have their babies naturally, maybe because they have money. But why is it we [Black women] always have to get cut on?—SP7
This study participant explained how losing her mother during her second trimester was more stressful in her pregnancy. However, doctors were seemingly more focused on the fact that her mother had gestational diabetes. This is particularly important because the study participant mentioned that her mother did not die from gestational diabetes, but from another cause. It is interesting that her doctors focused on the diet process, rather than the grief process.
My mother had gestational diabetes when she was carrying me. And [the doctors] kept wondering if I also would have gestational diabetes in my pregnancy too. But they also did not understand that I lost my mother during my second trimester, and that caused more stress than anything. Not the diabetes.—SP1
Collective memory and birth trauma
Collective memory focuses on the generation of stories throughout the respondent’s lineage, associations, familial arrangement, and social network. Birth trauma, in this case, was framed as the direct and indirect trauma experienced by this study participant, relating to how these collective memories impact their social and mental health. For example, this specific respondent described how her cousin’s traumatic birth experience also impacted on her own birthing trauma. It is important to note that social support (though necessary) was not the issue, but rather reduced social isolation in the lived experience of a potential c-section. Collective Memory, in this vein, remained a psychological trigger in the study participant’s perception of giving birth at the clinical encounter. This makes us wonder what additional indirect health experiences are faced by racially minoritized groups. Also, how these occurrences (among family members) further contribute to the collective memory 31 of obstetric racism. This quote also highlights how a patient may perceive the haste to perform a non-requested c-section, and how spirituality is drawn upon as a coping strategy at the clinical encounter.
But with my cousin, they were about to cut on her. But me and her [we] held hands and prayed so hard in that room and then the baby came that night, without them having to cut on her. They were getting ready to cut on [her], talking about “we have to get the baby out of you [because] the baby is in stress” and her baby was not [in stress]. The baby came right on out, without the cutting.—SP9
Vaginal birth after C-section and Insurance coverage
Despite having private health insurance, difficulties with insurance network and healthcare providers were experienced, particularly when a study participant requested to have a vaginal birth after C-section (VBAC; which made finding an OBGYN in her network an additional stressor). We did notice that participants described their own understandings on the limitations of VBACs based on anesthesiology and mostly from their associations with how this information is publicly disseminated: So, a lot of these OBs I felt had different intentions, so when I would ask about VBAC’ing and they didn’t support it, I would [not] just stop there. And then . . . So, it was hard to find an OB through the normal channels, like a providers list. Like the Blue Cross Blue Shield, in network people, and just going through the major hospitals and who are their providers. No one there supported a VBAC.—SP14
“Tummy-tucks” as incentives for c-sections
The doctor’s propensity for c-sections, specifically regarding how the procedure was incentivized by the inclusion of additional surgeries (e.g., “tummy tucks”), was explained by this study participant who described her doctor as amazing but also was “warned” about his implicit incentives.
My doctor was amazing. He delivered me when I was born. And he delivered my first child. But this doctor [also] loves to do c-sections, so I was told to watch out for him on that. He will suggest a c-section and offer a tummy tuck as an incentive. I was warned about that about him.—SP3
Trust of one’s own body for autonomous decision-making
The capacity for autonomous decision-making and trust were also expressed, regarding the sense of control over one’s own body. This particularly relates to the notion of efficacy (about birth choice) and how ongoing (postpartum) reproductive healthcare is constrained.
After my birth, I wondered, how do I get back to a place where I can make decisions about my own body. I felt like I had to depend on others to make decisions about my own body.—SP1
Discussion
Racial birth trauma is a critical aspect of our results. We defined racial birth trauma as a term to translate the results from our study, which reconnects the Black patient’s lived experiences occurring during pregnancy and birth as potential explanations on the impact of their mental health occurrences. The term bridges the gap between maternal and child health research and mental health/social psychological health research. Racial birth trauma was coined, defined and developed in collaboration with the quotes from our patient data, the literature, and our data analysis. To prevent researcher bias, during the NVIVO coding process, we generated codes for both positive health experiences (e.g., enjoying the birth experience) or negative health experiences (e.g., experiencing racism). However, majority of the study participants expounded on their lived experiences with racial discrimination during clinical encounters, particularly regarding c-sections. Additionally, hearing or witnessing racist health experiences that happened within their social/familial networks further caused them additional social and mental stress.
We further contextualize our results through a social scientific framework (see Figure 1, conceptual model) to illustrate how medical racism can exacerbate pre-existing health conditions and further overlap with obstetric racism, impacting the lived experience and considerable high-risk prenatal diagnosis. By examining patient narratives of high-risk pregnancies and c-sections, we observed how Black women’s experiences are latent with psychological trauma that can occur from these medical procedures, particularly surgical procedures (that already have their own complexities). Again, these are based on patient perceptions as their interpretation of what they knew or did not know to be reported in their medical records. Being “cut on,” for example, directly connects to the intergenerational trauma experienced by Black women during childbirth, as Black women were historically subjected to experimental procedures without anesthesia. Many of the participants described how their own biological mothers, grandmothers, aunts, and so forth also experienced traumas from c-sections. This showed us that there is a lineage of trauma throughout families that is all too often unacknowledged as part of racial birth trauma, regardless of whether a Black woman decides to have a biological child.
Based on our results, we observe how the overlap of obstetric and medical racism contributes to Black women’s adverse reproductive health experiences (see Figure 1). Results also showed even when participants requested an epidural or desired (or planned) for a c-section, it was still rooted in a lived experience of adversity as described by the participants themselves. We coded for positive experiences in birthing among Black woman, but noticed sentiments of racial trauma and racial discrimination, particularly in the context of urban cities amid a diverse region, where residential segregation and high racial clustering reduce access to high quality health services. This has implications for urban cities and other diverse regions within the United States where Black populations cluster. When Black women requested Black female OBGYNs, these clinicians and providers were still vulnerable to the institutional arrangements (upheld by structural racism) that privileged senior White male physicians. In other words, there were Black women who specifically requested Black OBGYNs and Black clinicians, but (1) such Black providers and clinicians were still susceptible to the institutional arrangements of being undermined by the more Senior White Male providers and (2) there was/is a shortage in Black providers for sufficient racial concordance.
Few studies show how the structure of reproductive medicine inflicts trauma on Black bodies, by undermining the lived experiences of Black women, such as the case with Shalon Irving. 3 We argue that failing to examine the lived experiences of c-sections across high-risk and/or low-risk pregnancies may overlook the connections to maternal morbidity/mortality, 35 infant morbidity, 19 and ongoing health complications15,29 such as any postpartum traumatic health occurrences that occur from race, medical racism, and obstetric racism. C-sections can also be a result of maternal morbidity or ongoing health complications; thus, it is worth acknowledging this complex, potentially multidirectional implication via the lived experience. We contend that the plausibility of these results is due to structural factors, including racism, sexism, ablism, hegemonic medical oppression, and social class discrimination that pre-exposes Black women to social determined health disparities and medical conditions, and intergenerational psychological traumas. 28
For example, a population-based study observed a sample of n = 3,956,112 women in the United States who delivered live births in 2016 12 showed that among this cohort (based on six categories of racial groups, such as White, Black, American Indian or Alaskan Native (AIAN), Asian, Native Hawaiian or Other Pacific Islander (NHOPI), and mixed-race) about 31.8% of total births resulted in c-sections, with Black women having the highest c-section rate. 12 Similarly, a retrospective, longitudinal study was conducted to observe racial differences among women (N = 28,493) who gave birth by c-section between 1980 and 2001. 13 Results showed that Black women were 1.48 times more likely to have a c-section than their White counterparts. 13 This longitudinal study highlights an issue of concern that underlines how structural factors can often the increase of pre-existing conditions, stemming from medical racism and can perpetuate obstetric racism.
One of our themes revealed systemic barriers to accessing preferred birth options due to insurance limitations. Research should examine policy-level inequities, provider availability, and how insurance status affects maternal care pathways. Healthcare systems and providers should advocate for equitable access to VBAC and, if appropriate, birthing centers, especially for Medicaid recipients and high-risk patients. This includes improving referral networks and expanding coverage options.
Our results also underscore the psychological and emotional aftermath of birth experiences, especially among minoritized populations. 36 Research should investigate postpartum recovery, bodily autonomy, and the rebuilding of trust in both self and healthcare systems. Clinicians should prioritize shared decision-making and affirm patients’ bodily autonomy. This includes validating their experiences, offering choices, and supporting emotional recovery after birth. Finally, our findings highlight how racialized birth trauma is not isolated but passed down through generations, shaping expectations and fears around childbirth. Research should explore intergenerational narratives, systemic racism in obstetric care, and how these experiences influence maternal health outcomes and decision-making. Healthcare providers must be trained in anti-racist and trauma-informed care in order to better recognize the historical and familial context of patients’ experiences. This can improve trust, communication, and culturally responsive care.
Patient-blame, also referred to as “victim blame” or “mother blame,” for high-risk prenatal status is also a serious ethical consideration. Applicable to women with low-risk pregnancies, studies highlight how individual health behaviors perpetuate a social climate of patient-blame, 37 where doctors put the brunt of prenatal issues on the women’s lifestyle choices. We argue that in failing to contextualize how lifestyle choices are also influenced by social structures and adverse clinical encounters, how medical structures perpetuate psychological trauma. 31 Achievement of low-risk pregnancy, for example, is usually rationalized through health factors such as genetics and health behaviors such as diet and exercise. 12 This arguably contributes to patient-blame instead of structural and environmental examination. 37 Blaming mothers, despite the alarming racial differences in c-section rates, 7 also does not tell us why reproductive disparities remain.
As the magnitude of reproductive health outcomes is conventionally captured through statistical data,12,13 a critical gap that has yet to be investigated are the patient-narratives present behind the numbers. 10 Meaning, the lived experience of c-sections among Black women is neglected as a legitimate source of data in reproductive medicine. Studies on c-sections, framed as either an option of self-election (patient-choice) and/or a medical emergency (physician-recommendation), 9 are rarely examined through the lived experience of racially minoritized patients. Therefore, we argue that the field of reproductive medicine needs to go to greater lengths to investigate (and contextualize) the patient-narratives behind the numbers.
We also notice how having a high-risk prenatal status7,14 reduces the physical agency of a birthing person, which impacts trust of their own bodies. 33 Black women deal with negotiating and navigating social contexts that have historically socialized medical providers and clinicians to also distrust Black bodies as knowers of their own health ailments.5,6,34 The complexity of trust among high-risk prenatal populations also makes Black women giving birth situated to be entirely reliant on clinical interventions, particularly when one’s trust is needed during surgical procedures, but still seemingly unearned and uncertain.
The historical underpinnings of c-sections5,6 combined with uncertain trust dynamics further reduces agency birthing persons may feel in their lived experiences. This is also critical because Black women (in our study sample) expressed desires to give birth outside-of-hospitals (e.g., birthing centers) but had restricted accessibilities to give birth with midwives and birthing centers, 33 due to high-risk prenatal status. Scott and Davis. 30 developed the Patient Reported Experience Measure of Obstetric Racism (PREM-OB) scale in 2019. This measure quantitatively captures Black women and birthing people experiences of labor, birth, and postpartum care in hospital settings across six domains, including: safety, autonomy, communication, racism, empathy, and dignity. Drawing from their metric, we designed a conceptual model (see Figure 1) for contextualizing patient-narratives of high-risk prenatal status and c-sections, relating to obstetric racism.
Patient perceptions about traumatic experiences during birthing may also serve as an indirect pathway as to how the impact of reproductive health disparities impose on the quality of life and the lived experience. Ultimately, examining Black women’s perceptions of c-sections, as well as how the historical dynamics of c-sections perpetuate less optimal experiences in the present-day context, is of critical concern. For example, Ani 7 found that since c-sections are extremely high for Black women in the United States, this high rate negatively impacts entire Black family dynamics (e.g., longer healing duration in postpartum and family strain on social support systems). Future studies should thus investigate how these “cutting” experiences trigger ongoing psychological harm (for minoritized families) regarding racism before, during, and after surgical procedures.
A conceptual model for obstetric racism and the lived experience
Obstetric racism29,30 functions because of structural racism, in conjunction with medical racism, influencing reproductive disparities. Obstetric racism 29 also arguably ascribed onto racially minoritized bodies during surgical procedures, such as c-sections, potentially perpetuates direct and indirect adverse lived experiences of birth trauma (psychological occurrences). The thrust of this conceptualization is not necessarily about c-sections in isolation. Rather, the key point is that by analyzing c-sections, we can concentrate on how the social structure perpetuates the susceptibility to high-risk pregnancy, rendering Black women’s susceptibility to c-sections. In other words, through an investigation of the lived experience or the patient-narratives, we can gain a heightened understanding of the routes that potentially generate adverse reproductive health experiences. For example, we solely focused on describing the lived experiences and patterns that stood out across a collection of demographics, including socio-economic status (SES) and education levels. The goal, however, was to capture how Black women in our study express specific viewpoints on c-sections, regardless of their demographics and SES. This is important because Black women experience high levels of preventable prenatal and birthing complications, regardless of their SES status.
Questions for reproductive health researchers and providers to consider: applying our conceptual model
Our concept of “medical racism” captures the pre-existing health conditions, as we intentionally decided to not include a circle on “pre-pregnancy health condition” because (1) not every person or woman will decide to become pregnant and (2) to allow for the model to be broad enough so that it can be applied as a potential template for medical trainings. The results from study thus map onto Figure 1. For example, prior experiences and pre-existing conditions are indicative of lived experiences with medical racism. Whereas occurrences during pregnancy and birth procedures are indicative of lived experiences with obstetric racism. According to Davis, 38 obstetric racism is a form of medical racism, but a distinctive type of racism that is defined through obstetric violence, in which clinicians perpetuate reproductive dominance over the autonomy over pregnant and birthing persons. Our figure provides a depiction of how medical racism and obstetric racism overlap through an intersection of racialized gender-based oppression, while both being fundamentally rooted in structural racism. We provided this model as a translation of our study’s results, to be useful for case studies and clinical scenarios for medical training.
Applying the model
Example questions to consider: (1) How is the lapse in communication between doctors an example of obstetric, medical, or both types of racism? (2) How is insurance coverage or lack thereof for VBAC a form of obstetric racism? (3) How do lived experiences contribute to prenatal stressors? (4) What are social and structural forms of racism and how do they perpetuate medical/obstetric racism? (5) Can racism be a pre-existing health condition for exacerbating prenatal health conditions? (6) How can the structure of reproductive health and clinical practice also be held accountable in the perpetuation of prenatal stressors? (7) How can research teams design reproductive health studies that capture the lived experiences of marginalized birthing people? (8) How can the public dissemination of data and information shape or misshape reproductive health disparities? (9) How can high-risk pregnancies among marginalized women be prevented? (10) How can we contextualize pregnancy and birthing outcomes so that we are not patient blaming for individual health behaviors? (11) How can we reduce c-sections and/or connect hospitalized birthing procedures to mental health trauma? (12) How can lived experience of c-sections among marginalized groups be understood as a legitimate source of data?
Strengths and limitations
Regarding recruitment, the first author drew from her network affiliation as a Miami native, thus, we acknowledge any recruitment bias in our limitation section. However, this is also why the study design was respondent driven to capture referrals outside of the hospital setting, and from patients in other areas across the South Florida region, such as in North Miami where there are larger concentrations of Black groups. This is also a substantial strength of the study, as Black perspectives in South Florida are often marginalized in larger samples and among White and Hispanic individuals, particularly among Hispanics who self-report as White or are White presenting in the South Florida region. Our sample size is one of the strengths of this study because we were able to engage an often underprioritized population. 20 For instance, we reached saturation regarding the perceptions among a specific group of women; and if our sample size were to increase, this would not negate the fact that Black women still have the highest prevalence for c-sections out of all racial groups in the U.S. context. 12 Our sample size thus captures the granular nuances that are often missed in quantitative studies on the lived experiences and perceptions of c-sections.
In terms of limitations, we acknowledge that there is a shortage of nurses 20 and nurses play a critical role in alleviating or perpetuating these dynamics, and we recognize the importance of nurses and their impact on patient health outcomes. 39 And, although nurses play a role, we also solely focused on the patient’s lived experiences with their clinicians during the birthing procedures and/or their reflections of other women’s experiences in their families and networks. We also acknowledge that our study population is concentrated in South Florida, and due to insurance laws varying state by state, the findings may shift across the U.S. context. In some instances, participants felt comfortable sharing their insurance coverage for both private and public options, as they specifically requested providers who were racially or culturally similar as themselves. However, even in these cases, our data showed that the recommendations of these providers were still susceptible to being undermined by more senior White male providers. In other words, while South Florida is a culturally diverse geographical location, the institution of medicine has a shortage Black and Latinx providers for minoritized patients to select from when making decisions about their prenatal and birthing care. Thus, racial concordance was not collected in the data and thus was difficult to determine in this study. Another limitation we also note is that we did not initially seek to examine high-risk pregnancies or c-sections. Rather, this dataset was initially on a broader representation of viewpoints regarding the lived experience of reproductive health issues. However, this specific study was designed from the latent results based on the first author’s prior study. 10 The overlap between medicine and legality is indeed a serious circumstance, particularly in terms of policy dynamics across the nation (and in South Florida where our data were collected). In this vein, while we focused on the lived experiences of participants in this region, we aimed to frame our results using medicolegal paradigms and policy to contextualize the micro experiences within macro dynamics.
We are aware that our study neglects to examine the medical benefits of c-sections. C-sections, we recognize, have often saved the lives of both the mother and fetus17,19 which is indeed necessary in reproductive medicine. Though studies have examined the medical benefits of c-sections, we were clear that this was not the aim of our article. Instead, our objective was to concentrate on Black women’s perceptions c-sections, as it relates to high-risk pregnancies and seeks to illustrate how our findings can apply to a conceptual model on obstetric racism based on our results.
Conclusion
Rather, the much deeper key concern is that our findings were able to illustrate perceptions of lived experiences of Black with high-risk pregnancies and the social and clinical environments that uphold these inequities. The focus remains that regardless of desired birth plans, Black women were more susceptible to receiving high-risk prenatal diagnosis which overruled how they navigated their birthing choices.
Facilitating and enabling social processes that ultimately reduce racism as a fundamental cause is also of significant importance for reproductive equity. The social determinants of health thus require deeper contextualization that recognizes how these birthing processes —are not just social,—but also historical. Meaning, Black women have been historically subjugated as medical-subjects to develop this surgical procedure)5,6; thus, Black populations require specific conceptual models that can illustrate why and how health outcomes and psychological racial traumas persist across the life course.
Results from our research can further inform public health policymakers, clinicians, scientists, hospitals, and health leaders. Integrating a social scientific frame on obstetric racism (see Figure 1) thus impacts the ways in which hospitals can improve the quality of patient care for Black women and additional minoritized groups at the clinical encounter. Future research however needs to investigate how Black women navigate obstetric racism across various regions in the U.S. context regarding climate change and environmental injustice. Quantitative investigations, 8 alongside qualitative studies, would allow for a more comprehensive framework regarding the degree of these disparities and can ultimately measure the plausibility of our conceptual model on obstetric racism.
The connection between birth trauma and c-sections performed on Black women’s bodies has rarely been connected to medical and psychological racial trauma in empirical studies. Our results show that a conversation on reproductive disparities should encompass how medical structures also contribute to mental health complications in the lived experience among Black women and across the postpartum period, including maternal depression and/or anxiety. 40 Ongoing studies should explore how stigma, patient shaming, and birth type contribute to birth trauma and how c-sections (planned or unplanned) contribute to postpartum depression. There should be a call to action to specifically encourage clinicians to be trained on medical racism and obstetric racism, while encouraging and offering marginalized patients to seek out mental health services after birthing experiences. We also hope our conceptual model can be utilized for interrogating the overlap between medical racism and obstetric racism and used in clinical trainings for providers, clinicians, and health researchers going forward.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251409927 – Supplemental material for Cesarean Sections and Racial Birth Trauma: A Qualitative Analysis for Obstetric Racism among Black Women in the United States
Supplemental material, sj-pdf-1-whe-10.1177_17455057251409927 for Cesarean Sections and Racial Birth Trauma: A Qualitative Analysis for Obstetric Racism among Black Women in the United States by Shameka Poetry Thomas, Praise Iyiewuare, Tiara Ranson, Leah Goldenberg and Kyrah K. Brown in Women's Health
Footnotes
Acknowledgements
We would first like to acknowledge our study participants who so generously shared their perceptions and health experiences with us. We would also like to acknowledge our research team at the University of Miami where the data were collected; and the local community organizations who support Black experiences in maternal health, particularly in the South Florida region and throughout the United States.
Ethical considerations
Ethical approval was obtained from our Institutional Review Board 2018 (IRB#20180221), including informed consent to participate in written format, with an optional verbal consent. Our continuing report was submitted and approved in 2019 (CR#00010707).
Consent to Participate
Both written and verbal consents were approved by the IRB.
Consent for publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the University of Miami’s Research Award. The Ohio State University College of Medicine provided support of the medical illustration and medical graphic used for Figure 1.
Author contributions
All of the listed authors contributed to the data analysis and writing process of this scientific publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are only available upon request due to the sensitivity of the study participant’s health experiences. Medical graphics are readily available for publishable format and public usage. Please contact the corresponding author to request data accessibility and/or medical graphic details.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.