
Abstract
Background
Patients with opioid use disorder (OUD) experience low treatment retention in primary care. Measurement-based care informed by patient-reported outcome measures (PROMs) is an evidence-based intervention to improve OUD outcomes. The study explored the key contextual factors to support the future planning of a PROM-based intervention package to improve primary care-based OUD treatment retention.
Method
A qualitative contextual inquiry used the Practical, Robust Implementation and Sustainability Model to assess the following contextual domains: Perspective of Intervention Characteristics, Partner Characteristics, and Implementation and Sustainability Infrastructure. Data were collected through interviews with system administrators, clinicians, and patients. Prioritized themes were triangulated with focus groups of community members with lived experience or interest in substance use care. Rapid thematic analysis identified emergent themes.
Results
We conducted 21 interviews (6 administrators, 10 clinicians, 5 patients) and two focus groups (22 community members). Fifteen themes emerged which fell into three categories: (1) maintaining patient trust while PROMs are integrated into workflows, (2) perspectives on PROM content and use, and (3) implementation considerations. PROMs were viewed as tools for enhancing communication, tracking recovery in a holistic and individualized way, and informing care decisions at the individual- and system-level. Patients emphasized trust, confidentiality, and potential negative consequences of PROM results being stored in health records. Clinicians highlighted the need for workflow integration and result interpretation support. All groups recommended PROMs be embedded in the electronic health record with collection managed by the integrated substance use treatment counselors.
Conclusions
The qualitative contextual inquiry identified partner perspectives relevant to the implementation of PROMs in primary care settings. The patient desire for trust and confidentiality may be at odds with integrating PROM results into existing systems. Continued engagement with implementation partners in a process of co-creation may improve implementation to support patient-centered, recovery-oriented care and enhance retention in primary care settings.
Plain Language Summary
Many people with opioid use disorder (OUD) receive treatment in primary care, but these clinics are extremely busy, leaving clinicians with limited time to focus on what matters most to patients’ recovery. One way to support better care is to use short questionnaires, called patient-reported outcome measures (PROMs), that help patients share how they are doing and guide conversations during visits.
We wanted to understand what it would take to use PROMs in primary care in a way that works for patients, clinicians, and the health system. To do this, we talked with administrators, clinicians (including substance use counselors), and patients receiving primary care-based OUD treatment. Participants said PROMs could help patients communicate sensitive information and help clinicians notice when extra support is needed. They also felt PROMs should reflect what recovery means to patients, not just drug use or urine tests. At the same time, patients worried about how their answers might be used and who would see them.
Participants emphasized that PROMs need to fit smoothly into busy clinic workflows, be built into the electronic health record, and use existing staff, like the substance treatment counselors, to help with collection.
By hearing directly from patients, clinicians, and community members, we identified what a PROM-based approach would need in order to build trust, measure what matters, and fit into everyday primary care.
Keywords
Introduction
In the United States, the use of nonprescribed opioids, such as heroin and illicitly manufactured fentanyl, are responsible for over $1 trillion annually in economic losses and 75,000 deaths annually, and have contributed to the greatest drop in life expectancy over the past century (Arias et al., 2022; Centers for Disease Control and Prevention (CDC), 2024; Florence et al., 2020). Methadone and buprenorphine are the mainstay treatments for opioid use disorder (OUD) (Cunningham et al., 2020). Methadone is restricted to federally registered opioid treatment programs (“methadone clinics”) and specialty addiction treatment clinics are geographically limited (Joudrey et al., 2020). As a result, expanding access to OUD treatment in primary care became a national priority. An estimated three-quarters of adults visit a primary care clinician each year, and 1%–5% of those patients are estimated to have OUD (Donroe et al., 2020; Levine et al., 2020; Wu et al., 2017). OUD treatment in primary care increased 600% from 2006 to 2014, and by 2009, primary care clinicians surpassed psychiatrists in the number of visits for OUD care (Wen et al., 2019). Beyond increasing capacity, there is strong patient demand as patients often prefer receiving OUD treatment in primary care due to its lower associated stigma and the comprehensive nature of care addressing co-occurring medical and preventative health needs (Barry et al., 2016; Incze et al., 2023).
The effectiveness of primary care-based OUD treatment is well established, however retaining patients remains a persistent challenge. Only 30%–60% of patients stay engaged for at least 6 months, which is the duration recognized by the National Quality Forum as a quality metric benchmark (Cope et al., 2022; National Quality Forum, 2017; Tofighi et al., 2019; Weinstein et al., 2017). Primary care settings are defined by diversity in medical and behavioral conditions addressed, and competing administrative demands often reduce the amount of time available to address OUD in patient visits (Safran, 2003). Improving retention will require strategies that fit the realities of primary care clinics while supporting both patients and clinicians.
Measurement-based care is an evidence-based practice which offers a promising approach to address these issues of patient retention in primary care OUD treatment (Marsden et al., 2019; Scott & Lewis, 2015). The core features of measurement-based care include obtaining data from patients using validated assessments, termed “patient-reported outcome measures (PROMs),” sharing the results of PROMs with the patients and using the PROM data to guide shared clinical decision-making (Scott & Lewis, 2015). In 2015, international experts highlighted the need for a measurement-based care approach to OUD treatment using PROMs across treatment settings and proposed adapting the OUD diagnostic criteria for patients to self-report outcomes (Marsden et al., 2019). Kaiser Permanente Washington then launched a system-wide collection of general substance use disorder outcomes (Hallgren et al., 2024; Matson et al., 2023) and AMNet, a practice-based research and quality improvement network, developed resources and recommended a set of PROMs to support treatment for outpatient addiction medicine treatment (Clarke et al., 2021). While these early efforts suggest that implementing PROMs is feasible, sustaining collection has proven difficult (McCarty, 2019) and the implementation of PROMs in primary care-based OUD treatment remains underexplored (Bradley et al., 2019).
There is a gap in understanding the contextual factors that would support or impede the successful implementation and sustainment of an intervention of measurement-based OUD using PROMs in primary care settings. The goal of this study was to inform the planning and design of an intervention package to collect PROMs to support measurement-based OUD care. To address the gap in the literature and ensure interventions are responsive to the needs of those delivering and receiving care (Mielke, Brunkert et al., 2022), we conducted a pre-implementation contextual inquiry guided by the Practical, Robust Implementation and Sustainability Model (PRISM) of the determinants of successful implementation and sustainment (McCreight et al., 2019).
Methods
Study Design
Our qualitative contextual inquiry design sought to identify and describe the relevant information about the primary care context where the intervention package (PROMs) will be delivered. This information will be used to guide future planning, implementation, and sustainment phases. An intervention package is all components of the intervention including the theoretic foundation, features of the intervention design, intent of the intervention, and implementation strategy components such as training and protocols (Kilbourne et al., 2007). We grounded our approach in Mielke, Leppla et al.'s (2022) description of the six components of a contextual inquiry: (1) choosing a theory, model or framework, (2) identifying relevant contextual factors, (3) involving stakeholders/partners, (4) developing a study design, (5) determining how the context influences the intervention package co-design and implementation strategies, and (6) reporting the contextual analysis.
In our case, dissemination and implementation science theories, models, and frameworks played a key role in the research process by providing a “systematic structure for the development, management, and evaluation of [dissemination and implementation] efforts, linking study aims, design measures, and analytic approaches” (Tabak et al., 2023, p. 492). A determinant framework to specify the contextual factors influencing implementation was most appropriate to support the planning and design of an intervention package (Nilsen, 2015). Thus, to address Mielke, Leppla, et al.'s first component, the research team chose PRISM to guide the research since it includes multi-level contextual domains for both clinical care teams (i.e., leaders, clinicians, staff) and patients in alignment with the study aim. In terms of the second component of Mielke, Leppla, et al.'s contextual analysis, we selected the perspectives and characteristics of clinic teams (across multiple roles) and the implementation and sustainability infrastructure as the key PRISM contextual elements to assess as our interviews and focus groups were time-constrained and there was insufficient time to address all PRISM domains (Glasgow et al., 2024). For Mielke, Leppla, et al.'s third and fourth components, we collaborated with our clinic/community partners to select the following qualitative methods to gather rich information about the context: individual interviews with implementation partners and focus groups with community members. Finally, components five and six are reflected in the presentation of findings relevant to the design of the implementation package and the overall reporting of the contextual analysis, following the Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007).
Setting
The Denver Health and Hospital Authority is an integrated safety-net health care system comprised of a hospital and 11 community health centers serving nearly 25% of the local population in Denver, CO, USA. The system has developed a comprehensive approach to addressing substance use in the target population, including having substance use treatment counselors (herein referred to as “counselors”) embedded within the primary care clinics to support prescribing clinicians and deliver behavioral health interventions for OUD (Bacon et al., 2025). The system is a recognized learning health system (Agency for Healthcare Research and Quality, 2019) with robust infrastructure to track population-level outcomes (Bacon et al., 2025; Prieto et al., 2019).
Study Population
Our target study population included those who would be directly involved with implementation of PROMs: (1) administrators who manage clinical programs, (2) clinicians, including physicians, advanced practice practitioners, and counselors, who provide primary-care based OUD care and therefore understand clinical feasibility, and (3) patients who receive primary care-based OUD care. We also aimed to include input from community members of people with lived experience of substance use (but not necessarily currently receiving care) or who have an interest in the care of people who use substances (Gilgoff et al., 2026). Community members with these characteristics are engaged in a standing community advisory meeting (CAM) hosted by the health system to gather feedback and comments about ongoing quality improvement projects and grant proposals (Bacon et al., 2025).
Data Collection
Our approach was to first conduct individual interviews among the three implementation partners: (1) administrators, (2) clinicians, and (3) patients. We then conducted focus groups with community members who participate in the CAM.
Individual Partner Interviews—Recruitment and Conduct
Individuals from our three implementation partner groups (administrators, clinicians, and patients) were recruited from email outreach and flyers to participate in 60-min semi-structured individual interviews. Participation required English-language proficiency and there were no additional inclusion or exclusion criteria. Administrators and clinicians were recruited via email outreach. Patients were informed about the study by their clinician and either provided permission for the study team to contact them or were provided with the study team's contact information. One investigator (JDP), who provides integrated OUD care in primary care, recruited patients from his patient panel. In addition, eight other clinicians who also provide integrated OUD care were asked to support recruitment by informing potentially eligible patients. Patients who expressed interest were contacted by phone. Each potential participant was contacted up to three times to schedule interviews, or if the scheduled interview was missed, to attempt to reschedule.
At the start of each interview potential participants were screened by the study's authors to verify eligibility, and the study and procedures were described in detail. No participants opted out of participating at this stage and all participants provided verbal consent and interviews were audio recorded. All interviews were conducted via phone or virtually (Zoom®) by a single author (JDP), who has qualitative research methods training. Zoom® AI transcriptions were referenced as needed if the recordings were unclear. Participants received a $30 gift card for participating.
CAM Member Focus Groups—Recruitment and Conduct
The CAM is an existing group that meets monthly, and the topic of the meeting is sent to an email list of community members who requested inclusion in the CAM 1 week ahead of time. Consistent with CAM protocols, we invited the first 25 community member participants who expressed interest to attend the focus group, which was held at the same time as the normal CAM meeting; those who attended received a $35 remuneration and a complimentary lunch. For the focus groups, to reach optimally sized groups for dialogue, community member participants were randomly separated into two equal-sized groups, where the study protocol was explained, and verbal consent was obtained. The groups were not audio recorded as it was outside CAM norms. Therefore, each focus group had a leader (JDP and SB [see acknowledgments]) and two coinvestigators (AG, LK, BF, and KD) who took contemporaneous notes which were used for analysis.
Interview Guide Development
We developed a semi-structured interview and focus group guide based on selected contextual domains from PRISM: (1) the multi-level perspectives of the intervention, (2) multi-level partner characteristics, and (3) implementation and sustainability infrastructure (Table 1). We did not include the PRISM domain of the external environment because it was out of scope of what members of the partner groups could meaningfully address and prioritized domains that would directly inform the initial design of the intervention package.
Working Definitions of PRISM Domains.
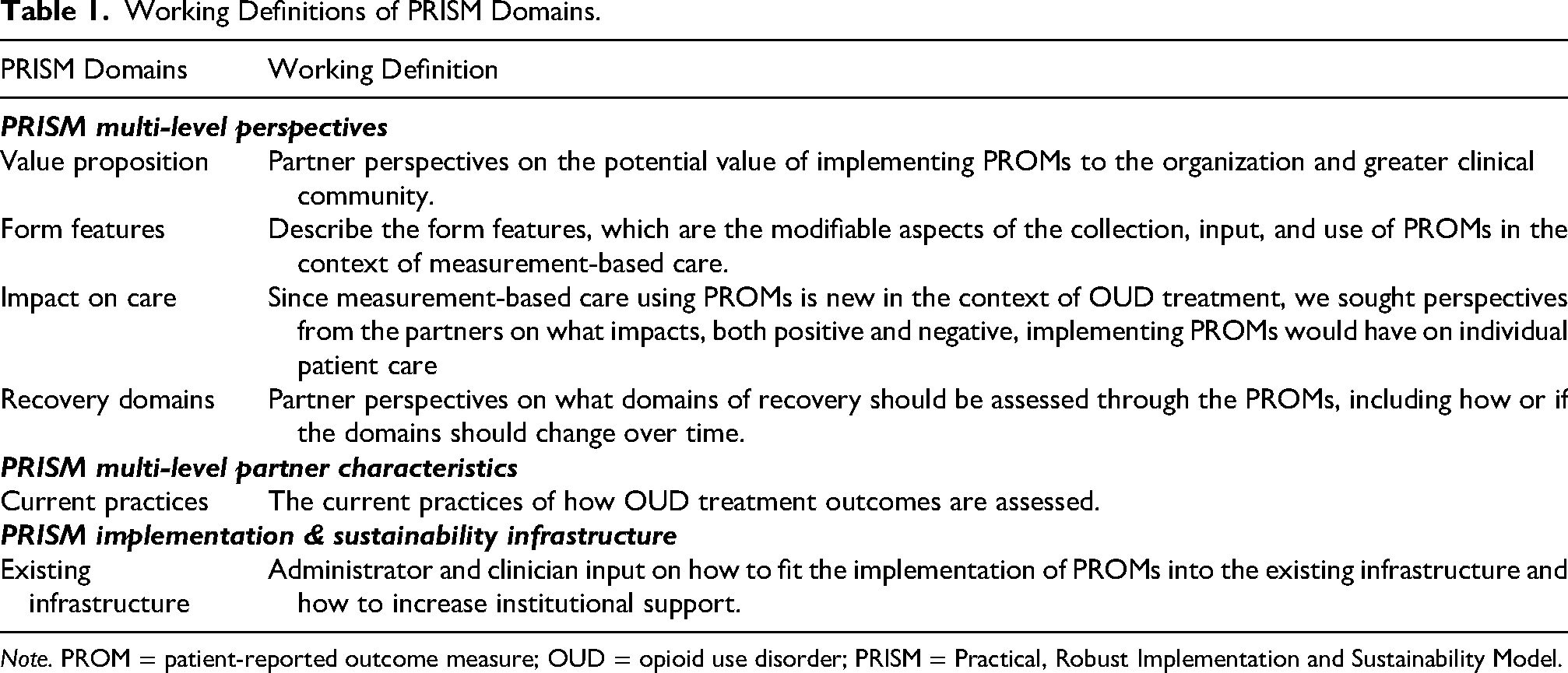
Note. PROM = patient-reported outcome measure; OUD = opioid use disorder; PRISM = Practical, Robust Implementation and Sustainability Model.
We explored PRISM Perspectives of the intervention in four distinct ways. First, we explored the value proposition of the perceived goals (“core functions”) for PROMs for OUD. Second, according to the Form-Function guidance for complex intervention, we also explored the form features since the characteristics of an evidence-based intervention that can be adapted while maintaining fidelity to the core functions (Perez Jolles et al., 2019). Third, we sought to describe potential unanticipated outcomes of PROMs, both positive and negative. Finally, as there are many existing PROMs for OUD care which are diverse in what aspects of recovery are assessed, we sought perspectives from participants on what they felt were the most important recovery domains to assess.
Related to the PRISM domain of “Characteristics” of our three partner groups, the interview guide was developed to elicit how outcomes are currently monitored to understand how PROMs may be integrated with existing outcome monitoring. Questions about the PRISM domain of “Implementation and Sustainability Infrastructure” sought to uncover how to fit PROMs into the existing primary-care infrastructure and how to increase institutional support. The Implementation and Sustainability Infrastructure domains were only assessed among administrators and clinicians, as they relate to the health system infrastructure which is relatively unknown to patients/community members.
Analysis
We analyzed the interview data using rapid thematic analysis and iteratively made refinements to the interview guide (Gale et al., 2019; Hamilton & Finley, 2019). This approach was optimal because our goal was to describe PRISM contextual factors which suited deductive analytic approach. We also needed to iteratively analyze interviews and focus groups quickly to accommodate both the competing demands on research staff and to meet the health system's timeline for integrating a PROM into the health record. Finally, funding constraints required a pragmatic method that allowed for efficient and economical use of team resources (Gale et al., 2019). Rapid thematic analysis took place in three key steps utilizing a matrix template (Schexnayder et al., 2023). First, a researcher (JDP, SL, or AG) conducted initial listening and created a summary document or note-taking of each interview. All interviews and focus groups were independently summarized by a single researcher. Next, a second researcher (JDP, SL, or AG) listened to the interview and reviewed and independently refined, edited, and expanded the summary of the first researcher. Next, these two researchers met to review the summaries and reconcile any differences, identify preliminary themes within each of the contextual domains, and create definitions. Each partner group (administrators, clinicians, and patients) were analyzed separately to identify preliminary themes within each group.
Preliminary themes which were similar between groups were then harmonized by the analytic team (JDP, AG, KA, SL). We held group sessions with the team to read the preliminary theme titles, definitions, and representative quotes. The team held group meetings to review the preliminary themes, combining those which were felt to be similar, and renamed the themes and adjusted the definitions.
The analytic team (JDP, AM, AG, KA) reviewed the preliminary themes and selected those which we felt were most important to triangulate with community members to strengthen the credibility and improve the representativeness of perspectives (Yin, 2011, p. 81). The study team reviewed the now harmonized themes and, through group discussion, identified those themes that were either (A) unexpected or (B) highly relevant to informing the intervention package and (C) related to topics that the community members could provide meaningful insight. Using the same rapid thematic analysis method, we identified emergent themes from the community member focus groups to clarify the themes from individual interviews.
The study team (JDP, AM, AG, BF, KA) identified key themes relevant to the planning and design of a PROM implementation package and applied an additional level of organization by categorizing the themes in two ways. First, the team grouped themes into de novo categories. One investigator (JDP) developed an initial categorization, which was then iteratively reviewed by team members (AM, AG, KA). Once the themes’ categories were finalized, the team collaboratively named and described the categories. Second, themes were organized according to the PRISM contextual domains that guided the development of the interview questions. From October 2023 through July 2024, interviews and focus groups were conducted alongside an iterative rapid analysis. A local institutional review board determined this research exempt.
Results
Of the 29 people who initially expressed interest in participating in interviews, 21 completed individual interviews: 6 administrators, 10 clinicians, and 5 patients. There were 22 community members who presented for the focus group; these were separated into two concurrent focus groups of 11 members each. The relevant demographic, clinical training, and treatment characteristics are presented in Table 2.
Participant Characteristics.

Other races include Asian and African American/Black.
Fifteen themes emerged from the analysis; these were grouped into three major de novo categories: (1) Maintaining Patient Trust as PROMS Integrate into Workflow, (2) Perspectives on PROM Content and Use, and (3) Implementation Considerations. These 15 themes are briefly summarized in their respective categories (Table 3) and are presented visually in Figure 1 including the relationship between themes. We also organized the themes by the PRISM contextual domains that informed the development of the interview question (Supplement eTable1). Figure 2 shows the crosswalk between the PRISM domains and the de novo categories, illustrating how themes align with each domain and category. In the following text, we present the thematic categories and individual themes, accompanied by representative quotes and investigator notes. Theme titles are shown in brackets, and direct participant quotes from individual interviews are attributed.

Visual representation of categories and themes. Dotted lines represent relationships between themes and categories. Created in BioRender. https://BioRender.com/sp5hume

Crosswalk of themes and the PRISM domains and categories.
Themes, Definitions, and Contributing Participant Groups.

Category 1: Maintaining Patient Trust as PROMs Integrate into Workflow
Themes in this category addressed the practical considerations of implementing PROMs, including building trust, integrating PROMs into care, and refining workflows to ensure that measurement supports clinical decision-making without compromising the therapeutic alliance between patients and their clinicians. All participant groups acknowledged that implementation of PROMs would impact the dynamic between patients and clinicians during care. While all groups felt the impact could be quite positive during the actual clinic visit, patients and community members had concerns about possible unintended consequences. Administrators conceived of PROMs as a less judgmental way to obtain information [Standardization Minimizes Judgement] and community members agreed. As one community member said, “questionnaires will be good, as sometimes those going in for the first time are not as comfortable sharing with doctor in that first visit.” Clinicians similarly focused on how PROMs would impact patient visits, indicating their belief that the results would improve the timeliness and efficiency of visits by showing a “red flag” when patients need additional support and help reduce missed opportunities for intervention [Improve Timeliness and Efficiency of Care]. Community members expanded the definition of this theme by imagining PROMs as bridges—tools that could connect patients to new clinicians and increase the efficiency of care.
While administrators and clinicians generally viewed PROMs positively, patients identified potential concerns. Patients generally felt comfortable sharing sensitive information with their clinician, since that is routine in clinical care [Trust and Transparency of Results]. As one patient noted, they already “trust them [clinicians] with my life” (Patient 31). But patients also emphasized the importance of transparency in how results are used to inform current and future care. One patient explained that patients might not give accurate responses if honest responses (e.g., returning to drug use) meant losing access to medications or being given a lower dose. Community members similarly expressed concern that results could negatively influence how future clinicians treat them, for example, not being prescribed pain medications even if they were clinically appropriate.
Measurement-based care involves sharing the results with patients and using the results to guide clinical decision-making. Clinicians emphasized the need for implementation strategies of education, training, and support on how to interpret and discuss PROM results with patients [Improve Knowledge]. PROMs would be a new clinical outcome in this context, and thus support would be needed to ensure that clinicians know how to access results, interpret scores, and how to use the results to make care decisions. But patients put considerably less stock into the scoring of their recovery status and indicated that they did not need to see their scores [Result Review Undesired]. As one patient stated, “As long as I’m not doing drugs, I don’t care about scores” (Patient 8), suggesting that while reviewing PROM results may be a helpful tool for clinicians, they may be of less inherent value to patients. This theme is also related to Category 3 themes describing the implementation considerations (see below).
Category 2: Perspectives on PROM Content and Use
Themes in this category focus on the measurement of outcomes for OUD treatment and how PROMs could help assess the unique experiences, preferences, and goals of patients. These themes emphasize a shift to normalize and routinize outcome monitoring in OUD care. Administrators viewed results as a tool for evaluating system-wide interventions and improving population-level outcomes [Making Routine Outcome Measurement Routine]. “You only change what you measure” (Administrator 73), one administrator remarked, underscoring the idea that system-level improvements hinge on quantifiable data. Community members echoed this theme, linking measurement not just to evaluation, but to service delivery.
Clinicians felt that the collection of PROMs should focus on health-related outcomes [Health-Related Outcomes]. Administrators and clinicians emphasized that PROMs could help add context to the process outcomes, which are routinely collected in the electronic health record [Contextualize Process Outcomes]. The process outcome measures included receipt of medication for OUD (e.g., days of dosing), being retained in care for a specific period (e.g., 90-days or 6-months), and naloxone co-prescribing. However, an administrator noted that these are “not rich data sources of recovery” (Administrator 10) and simply represent the currently available data.
A shared perspective between patients, clinicians, and reinforced by the community members was that PROMs provide meaningful outcomes for patients [Meaningful Outcomes for Patients]. Clinicians and patients alike described how tracking outcomes important to patients helped identify progress that might otherwise go unnoticed. One community member captured this sentiment saying, “It's really important to revel or celebrate what a person has done to achieve improvements or changes to make their life better or more sustainable.” For patients whose recovery journeys often unfold slowly, PROMs could offer tangible reassurance of progress. An administrator stated, “Recovery is not a straight line – it's a circle” (Administrator 7) and PROMs can be impactful at any time in care.
Reflecting the diversity of patient goals, a common theme among all participant groups was that PROMs need to assess the many distinct domains of recovery [Multidimensional Assessment]. Community members reflected that PROMs could assess aspects of a patient's life that go beyond simply asking about the presence or absence of substance use. This ideal of collecting outcome data that is multidimensional and individualized to the patient is juxtaposed to the current practice where patients and clinicians also noted that urine drug toxicology results are the outcome routinely collected in routine OUD care [Urine Drug Test]. Urine drug testing is a guideline-recommended practice and may be deemphasized if PROMs are collected (Substance Abuse and Mental Health Services Administration, 2020). PROMs may also provide important contextual data to aid in the interpretation of toxicology results and would be more applicable for patients whose treatment goals do not include abstinence.
Category 3: Implementation Considerations for Clinics and Teams
These themes represent the pragmatic factors that would influence the implementation of PROMs.
All participant groups agreed that integrating PROM collection into the electronic health record would be ideal [Integrated into the Electronic Health Record]. Collecting PROMs through patient portals or clinical workflows would ensure results of PROMs could be viewed in multiple places in the electronic health record. Additionally, integrating PROMs into the electronic health record could include longitudinal visualization and allow for interpretation in the context of other results, such as toxicology results or medication dosing history. As noted above for the theme “Result Review Undesired,” (in Category 1), it may be that initial efforts for integration in the electronic health record focus on how to make PROMs usable for clinicians.
When considering who should be responsible for collection of PROMs, administrators and clinicians (which include counselors) reported counselors are best suited, rather than the prescribing clinician who is often responding to multiple patient medical needs [Team/Counselor Responsibility]. One administrator put it plainly: “We cannot pile more on primary care” (Administrator 78), with a counselor adding that having counselors collect PROMs might even improve the honesty of responses by reducing perceived power differentials. Indeed, prescribing clinicians (e.g., physicians and advance practice practitioners) reported that they already strongly rely on counselors’ assessments when caring for patients.
All participant groups reflected on the current practices and noted that there was no consistent method for collecting data on patient recovery [No Consistent Collection Presently]. A clinician reflected on their practice, stating, “there is random free-text I put in my clinic note” (Clinician 19) and administrators noted that no system-level efforts have been attempted to collect data about patient recovery. This theme along with the “Improve Knowledge” theme (in Category 1) highlights how capturing PROMs in this context is a new endeavor that would require clinician and patient support to improve implementation. One way to improve implementation highlighted by clinicians and administrators was the importance of integrating the collection of PROMs into existing systems to reduce burden of collection [Leverage Existing Systems]. A clinician emphasized that in a busy primary care clinic, it was important not to slow down clinic flow. Administrators echoed this concern and suggested that integrating PROMs into existing workflows could enhance implementation.
Discussion
This qualitative contextual inquiry addressed how to develop an intervention package to collect PROMs and plan their implementation in primary care settings to support measurement-based OUD care. We identified themes that are relevant to the planning and development of this package in three broad categories: (1) Maintaining Patient Trust as PROMs Integrate into Workflow, (2) Perspectives on PROM Content and Use, and (3) Implementation Considerations for Clinics and Team. The findings offer actionable guidance for the next phase of intervention development. Further, this PROM-based approach could extend to other common substance use disorders managed in primary care, such as alcohol use disorder (AUD).
Themes in the first category encompassed how PROMs may impact care for both clinicians and patients, and how PROMs for OUD are different than other outcomes which are routinely assessed. A consideration from patients was the potential negative impact of PROMs on future care. OUD is a highly stigmatized condition and issues of confidentiality, sharing of results across the system, and concern about other results (e.g., urine toxicology, other) “following” patients have also been identified by others (Benintendi et al., 2021; Stablein et al., 2015). If not directly and proactively addressed, these trust considerations could have unintended consequences which, at minimum, may reduce open, honest responses and could even potentially worsen patient engagement. This finding is related to others’ research focusing on measurement-based care in behavioral health who provided examples on how to create a pathway for collection, storing, and sharing in the electronic health record to increase patients’ trust and willingness to respond (Lewis et al., 2019). The intervention package may therefore need to include restrictions on who can see results, which is a current capability of the electronic health record. Clinicians also emphasized the need to increase their knowledge on PROMs and the scoring. Most PROMs lack established benchmarks or minimally important differences in scores (Pytell et al., 2026) and the health system will need to routinely collect and analyze data to determine which changes in scores are associated with meaningful outcomes, such as retention in care, and integrated with feedback to improve clinician knowledge and skills.
Clinicians and patients expressed distinct perspectives on the utility of PROMs. While clinicians felt PROMs would improve the efficiency of visits, patients did not feel that results were as important for them to see since they know inherently if they are doing well or not. These insights suggest that the next steps in planning this line of research inquiry should address clinician-facing aspects of the intervention package, including choosing PROMs for inclusion, coaching on the use of PROMs, and protocols to integrate PROM collection into the clinic workflows.
Themes in the second category show how PROMs might redefine what “counts” as success in OUD care. Unsurprisingly, urine toxicology is the primary standard outcome assessment identified by the partner groups, and these tests have known limitations (Pytell & Rastegar, 2021). While not directly asked, no group reported that toxicology results or patient retention were unhelpful or unimportant metrics, but rather that results of PROMs could help contextualize these measures. Clinicians also expressed interest in seeing a “red flag” that patients are stumbling in their pursuit of recovery, which may or may not be present in a PROM for recovery that is more dichotomous in nature (“in recovery” vs. “out of recovery”). The intervention package should therefore include initial signals about changes in score to raise clinician awareness, which is similar to the implementation strategy of relaying clinical data to clinicians (Powell et al., 2012).
A key challenge is how to translate the concept of recovery, which is multidimensional and nuanced, into discrete data fields of the electronic health record using PROMs (Neale et al., 2014). There is tension in trying to pick a specific PROM, or concise set of PROMs, for a system-wide intervention package which is applicable to a large patient population while still being relevant to the individual patient. At the same time, any intervention to collect PROMs will need to minimize time to complete and complexity of scoring to reduce the burden on clinicians and patients (Stanick et al., 2021). Interpreting our results through a co-creation lens suggests that future research should focus on early and iterative assessment of candidate PROMs and their implementation before settling on a specific PROM or set of PROMs into the intervention package (Trinkley et al., 2023). Further, future iterations should actively engage external partners (e.g., payors or state-level behavioral health administrators) to determine if the outcomes are relevant from their perspectives and how to increase the value of these outcomes to this partner group.
The third category of themes informed planning and initial intervention package design. The Denver Health system is a local safety-net system which is reflective of sentiment that to improve implementation and sustainment the intervention must leverage existing staff and systems. The initial iteration of the package to collect PROMs will therefore be built using internal systems as opposed to using a third-party application, which requires additional cost. In terms of leveraging existing staff resources, clinicians and administrators explained that it would be best if the integrated substance use treatment counselors were responsible for collection. Several team-based models for primary care-based OUD treatment utilize counselors or other staff to support the delivery of care (Lagisetty et al., 2017; Wartko et al., 2023).
A persistent challenge in primary care is that many clinicians do not initiate treatment after identifying opioid or other substance use disorders. Barriers include limited institutional support, constrained cognitive capacity, and lack of knowledge or skills (Campopiano von Klimo et al., 2024). At the system level, substance use treatment is often not prioritized or incentivized, limiting its integration into routine care. Our findings suggest that PROMs may help address both individual and structural barriers. While this study focused on OUD, the findings may extend to AUD, which shares a significant public health burden, low treatment rates, and the availability of effective medications in primary care (Koob, 2024). Despite an estimated 10% prevalence and one in eight deaths attributable to alcohol, only 10% of individuals with AUD receive medication treatment (Esser et al., 2022; Le et al., 2024; Substance Abuse and Mental Health Services Administration, 2024). Systems aiming to expand OUD or AUD treatment in primary care should consider the role of PROM collection from the outset as a strategy to support clinicians and address common substance use disorders where medication treatment in primary care is both possible and pragmatic.
There are several limitations to our study. First, the target population was drawn from a single, urban safety-net health system of federally qualified health centers that are actively working to integrate OUD care across treatment settings. While this system likely shares characteristics with other US-based safety-net systems with integrated behavioral health care, the findings might not be fully generalizable to other contexts. However, the setting reflects the real-world complexity in which primary care-based OUD treatment increasingly takes place and may provide a starting point for other systems. Second, the use of rapid thematic analysis may increase the risk of misinterpretation or overinterpretation of participants responses. Finally, potential sources of bias include the study team's selection of which preliminary themes from the interviews were presented to community member focus groups, as well as the recruitment of some patient participants from the lead investigator's own panel and their subsequent interviews by that same investigator. These risks could have led to more positive input on PROMs from the interviews. These findings should be viewed as formative, guiding the initial planning and development of the intervention package. Ongoing iterative assessments will be needed to refine the approach and improve the validity of the findings across time.
Measurement-based care of OUD using PROMs marks a shift from “program-centered care” (Rastegar, 2021), where compliance and abstinence were the primary metrics of success, to care that focuses on patients and their perspective on recovery. PROMs are not just tools for assessment, but also a mechanism for a change in focus to be more patient-centered. This approach aligns with principles of learning health systems and creates a foundation for care that is adaptive to patient's evolving needs. Developing an intervention to collect PROMs with attention to these multi-level perspectives, characteristics and the health system infrastructure will support our overarching goals to improve retention in primary care by offering more patient-centered assessments of progress that can bring clinicians alongside patients in their pursuit of meaningful recovery.
Supplemental Material
sj-docx-1-irp-10.1177_26334895261438505 - Supplemental material for Utilizing the Practical Robust, Implementation and Sustainability Model to Explore the Primary Care Setting Contextual Determinants of Implementing Patient-Reported Outcomes Measures to Support Opioid Use Disorder Care
Supplemental material, sj-docx-1-irp-10.1177_26334895261438505 for Utilizing the Practical Robust, Implementation and Sustainability Model to Explore the Primary Care Setting Contextual Determinants of Implementing Patient-Reported Outcomes Measures to Support Opioid Use Disorder Care by Jarratt D. Pytell, Allison Macht, Deborah J. Rinehart, Aiden Gilbert, Steven Lockhart, Lily King, Brittney Fraumeni, Karina G. Duarte, Ingrid A. Binswanger, Karen Albright and Amy G. Huebschmann in Implementation Research and Practice
Footnotes
Acknowledgments
We would like to acknowledge Sarah Belstock, MPH, leader of the Center for Addiction Medicine Community Advisory Members board and Brooke Bender, MPH, Administrative Directory of the Center for Addiction Medicine, Denver Health and Hospital Authority, for their administrative support and facilities to host focus groups.
Ethical Approval and Informed Consent
The study was reviewed by a local Institute Review Board and determined Exempt (#23-0219). All participants provided consent to participate in the research study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported through institutional funding from the University of Colorado School of Medicine. Dr. Pytell was supported in part by the National Institute on Drug Abuse of the National Institutes of Health under Award Number K23DA060358. Dr. Huebschmann was supported in part by the Health Resources and Services Administration under Award Number 5T32 HP42016. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Health Resources and Services Administration.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ingrid Binswanger reports royalties from UpToDate for unrelated content. Dr. Pytell previously received funding from the PhRMA Foundation Faculty Starter Grant for unrelated research.
Data Availability Statement
Preprint Statement
This study and its results have not been published nor previously posted on a preprint server.
Supplemental Material
Supplemental material for this article is available online.