
Abstract
Background
Access to providers and programs that provide medications for opioid use disorder (MOUD) remains a systemic barrier for patients with opioid use disorder (OUD), particularly if they live in rural areas. The Rural Access to Medication Assisted Treatment (MAT) in Pennsylvania Project (Project RAMP) addressed this problem with a multisystem partnership that recruited, trained, and supported rural primary care providers to provide MOUD and implement an integrated care model (ICM) for patients with OUD. Given the demonstrated efficacy of Project RAMP, this article summarizes our recruitment strategies, including feasibility concerns for further expansion into other regions.
Methods
The approach for recruiting implementation sites included two phases: partner outreach and site identification. Once recruited, the Systems Transformation Framework guided planning and implementation activities. Recruitment and implementation activities were assessed with implementation trackers and evaluated by providers via key informant interviews (KIIs).
Results
Project RAMP recruited 26 primary care practices from 13 counties, including nine health systems and two private practice groups—exceeding the original target of 24 sites. There was a median of 49 days from first contact to project onboarding. A total of 108 primary care practices spanning 22 health systems declined participation. Findings from the KIIs highlighted the value of engaging PCPs by connecting to a shared vision (i.e., improving the quality of patient care) as well as addressing perceived participation barriers (e.g., offering concierge technical assistance to address lack of training or resources).
Conclusion
Findings highlight how successful recruitment activities should leverage the support of health system leadership. Findings also emphasize that aiding recruitment and engagement efforts successfully addressed prescribers’ perceived barriers to providing MOUD as well as facilitating better communication among administrators, PCPs, behavioral health professionals, care managers, and patients.
Keywords
Introduction and Background
In rural areas of the United States, opioid use disorder (OUD is a leading cause of preventable illness and death (Hedegaard et al., 2020). The current standard of care for OUD is providing medications for OUD (MOUD), including Food and Drug Administration (FDA)-approved medications such as naltrexone, buprenorphine, and methadone (Substance Abuse and Mental Health Services Administration, 2020). Naltrexone can be prescribed by any provider licensed to prescribe medications, but buprenorphine and methadone have more restrictions. Prescribing providers can be certified to prescribe buprenorphine under the Drug Addiction Treatment Act of 2000 with the completion of 8 h (for allopathic and osteopathic physicians) or 24 h (for advanced practice practitioners) of training from a credentialed organization. Upon completion, providers can apply for a waiver on their Drug Enforcement Administration (DEA) license to prescribe buprenorphine for OUD. Recently, the United States exempted the educational requirement for prescribers intending to treat fewer than 30 patients at one time, but providers must still notify the Substance Abuse and Mental Health Services Administration (SAMHSA) and the DEA of their intent to prescribe buprenorphine for OUD. As a Schedule II medication, methadone can only be dispensed at licensed opioid treatment programs.
Despite efforts to increase treatment access, individuals with OUD remain underserved. For example, in 2002, the FDA approved buprenorphine for OUD treatment (U.S. Food and Drug Administration, 2002), and agencies started encouraging primary care providers (PCPs) to screen patients for OUD and provide MOUD in office-based settings (Codell et al., 2020; Gordon et al., 2020; Substance Abuse and Mental Health Services Administration, 2020; Volkow et al., 2014). Yet as of 2018, more than 57% of rural U.S. counties lacked a buprenorphine prescriber (Ghertner, 2019). In nationally representative samples, only 35% of adults with OUD assessed between 2015 and 2017 received any treatment in the past year (Jones & McCance-Katz, 2019). Studies with claims data indicate substantial variability in coverage based on insurance and state of residence, ranging as low as 11% of adults with a suspected OUD based on claims indicators receiving MOUD among commercially insured patients to 40%–80% of comparable Medicaid patients (Donohue et al., 2021; Morgan et al., 2018). This suggests that the regulatory supports and guideline practices have not sufficiently addressed the MOUD access gap.
Unfortunately, patients bear the accumulating consequences of the MOUD access barriers across systems. Provider-perceived barriers include inadequate access to training (e.g., DATA 2000 waiver training), appropriate referral partners for supportive services (e.g., care management and psychosocial counseling), time/resources to adopt new treatments, and finances to support the MOUD services (Andrilla et al., 2018; Bolinski et al., 2019; DeFlavio et al., 2015; Ghertner, 2019; Hutchinson et al., 2014; Mackey et al., 2009; Manuel et al., 2013). Health system barriers to MOUD adoption include a lack of interested/qualified prescribers, insufficient referral and data-sharing infrastructure between treatment providers, as well as inadequate funding for MOUD-related clinical activities (Haffajee et al., 2018; Madras BK et al., 2020). Moreover, the stigma surrounding OUD and MOUD reduces patient and provider participation in MOUD treatment (Crapanzano et al., 2018; van Boekel et al., 2013). These barriers all contribute to ongoing morbidity and mortality from OUD.
The provision of MOUD alone is insufficient for addressing the scope of the opioid overdose death crisis (American Society of Addiction Medicine, 2020). The traditional addiction treatment models where care is siloed into specialty centers limit access and fragment the provision of overall care (Perrone et al., 2019). Drawing from chronic care models which advocate for treating substance use disorders (SUDs) as chronic health conditions within primary care practices (McLellan et al., 2000; McLellan et al., 2013), ICMs provide a structure where patients receive a blend of specialty medical services, such as MOUD, with behavioral health services (Perrone et al., 2019). The blended services within an ICM are coordinated by case managers who support providers as well as coordinate and track patient care across systems (Brackett et al., 2021). Though traditionally focused on depression and anxiety, data also indicate that ICMs for MOUD help lower costs while increasing patient and provider satisfaction (Archer et al., 2012; Brackett et al., 2021; Unützer et al., 2002).
Recognizing the need to increase access to MOUD and integrated care, a multidisciplinary team at the University of Pittsburgh partnered with the Pennsylvania Department of Human Services (DHS) to initiate the Rural Access to Medication Assisted Treatment (MAT 1 ) in Pennsylvania Project (also known as Project RAMP). Project RAMP was supported by a 4-year Research Demonstration and Dissemination grant led by the DHS and funded by the Agency for Healthcare Research and Quality (AHRQ #: R18-HS025072) that aimed to increase rural access to MOUD by implementing an ICM (Cochran et al., 2019, 2022; Cole et al., 2021). The goal of the Project RAMP ICM was to improve provider capacity to identify, assess, manage, and treat OUD by promoting a team-based approach to patient care and alleviating the PCP from some patient management responsibilities. The Project RAMP ICM provided a structure for connecting PCPs with existing community-based care management, SUD, and mental health treatment resources. PCPs received support to either provide patients with MOUD or then link them to appropriate care management/treatment resources or refer their patients to certified MOUD providers, providers with OUD/SUD treatment experience, or providers able to connect with other ICM services. A prerequisite for effectively implementing Project RAMP was effectively recruiting and engaging providers to participate. Despite repeated calls highlighting the need for improved provider engagement in research and recruitment strategies to facilitate enhanced implementation of evidence-based practices in the community, publications on recruitment strategies remains limited (Department of Health and Human Services; NIH Pragmatic Trials Collaboratory; Nourjah & Kato, 2021; Pinto et al., 2019).
This article has three objectives: (1) describe the recruitment of PCPs and implementation of the MOUD-focused ICM for Project RAMP; (2) describe the results of the Project RAMP recruitment approach in terms of practice engagement and duration of time from “initial contact” to completion of key implementation indicators; and (3) describe the feasibility of this approach to recruit PCPs and develop the MOUD-focused ICMs in other regions, based on provider feedback.
Method
Implementation Framework—Systems Transformational Framework
Project RAMP was guided by the Systems Transformational Framework (Scott & Pringle, 2018) throughout the design, recruitment, pre-implementation, and implementation process. The STF is centered on the concept that all human systems are both complex and adaptive; as such, the process for transforming these systems must involve (1) assessing the functioning of specific system domains, called “levers,” and (2) applying systemic strategies that utilize strong levers within the system to drive change (system transformation) towards the intended outcome. The STF delineates eight levers likely to influence optimal evidence-based practice implementation. The Implementation Team received approximately 6 h of training in the application of the STF.
Recruitment Process
The Project RAMP Implementation Team, based out of the University of Pittsburgh School of Pharmacy Program Evaluation and Research Unit, involved an average of 3.0 full-time equivalents throughout the project. The Implementation Team included persons with public health and data analytic expertise. The Implementation Team worked with the DHS and the Medicaid managed care organizations (MCOs) across the Commonwealth of Pennsylvania to identify potential primary care practices and systems in a set of 23 counties designated as rural by Rural-Urban Continuum Codes (United States Department of Agriculture, 2013) that had OUD prevalence and opioid overdose rates that were above the 2014 national average of 0.9% and 0.0083%, respectively (Han et al., 2015). Ideal candidate practices were those identified as being proximal to a care management entity and/or suitable SUD treatment resources that could support patient care. Care management service providers were located in the Commonwealth's Centers of Excellence (Commonwealth of Pennsylvania Centers of Excellence, 2021) or Single County Authority system, within licensed SUD assessment or treatment agencies, or within the recruited health systems. The Project RAMP goal was to recruit 24 primary care practices across 23 eligible counties over the grant period. These targets were selected to power the primary project analyses (to be reported in a separate manuscript) to detect a difference-in-difference intervention estimate with a 10%–20% increase at .009 desired accuracy (half-width for 95% confidence interval) for 1,000–2,000 intervention beneficiaries and 2,000–3,000 control beneficiaries. All procedures discussed below were considered exempt by the Institutional Review Board of the University of Pittsburgh.
Recruitment for Project RAMP occurred in two phases broken down into four steps, as shown in Figure 1. To determine the duration of the “Recruitment Phase” for each site, we calculated the number of days between initial contact and the onboarding meetings. Consistent with the STF, in the first phase (partner outreach), the Implementation Team engaged leadership from local agencies (governmental and private) providing care management and SUD treatment services and local health system leadership with the objective of developing collaborative relationships that could be leveraged in the recruitment of primary care practices. More specifically, care management and SUD treatment agencies were engaged to develop and implement comprehensive care coordination protocols with the PCPs, thus alleviating expectations on PCPs to provide intensive care management and counseling services in addition to pharmacotherapy. Like PCPs, care management and SUD treatment programs were required to participate in the project's informal health information exchange (HIE), continuous quality improvement (CQI), and performance measurement. Health system leadership was engaged to encourage PCP participation via strong verbal support for MOUD implementation and commitment of system resources to support MOUD provision where possible. Occasionally, initial contact with leadership personnel occurred via facilitated introductions from DHS and the MCO partners. In other cases, the Implementation Team reached out to care management and SUD treatment providers directly via telephone “cold calling.”
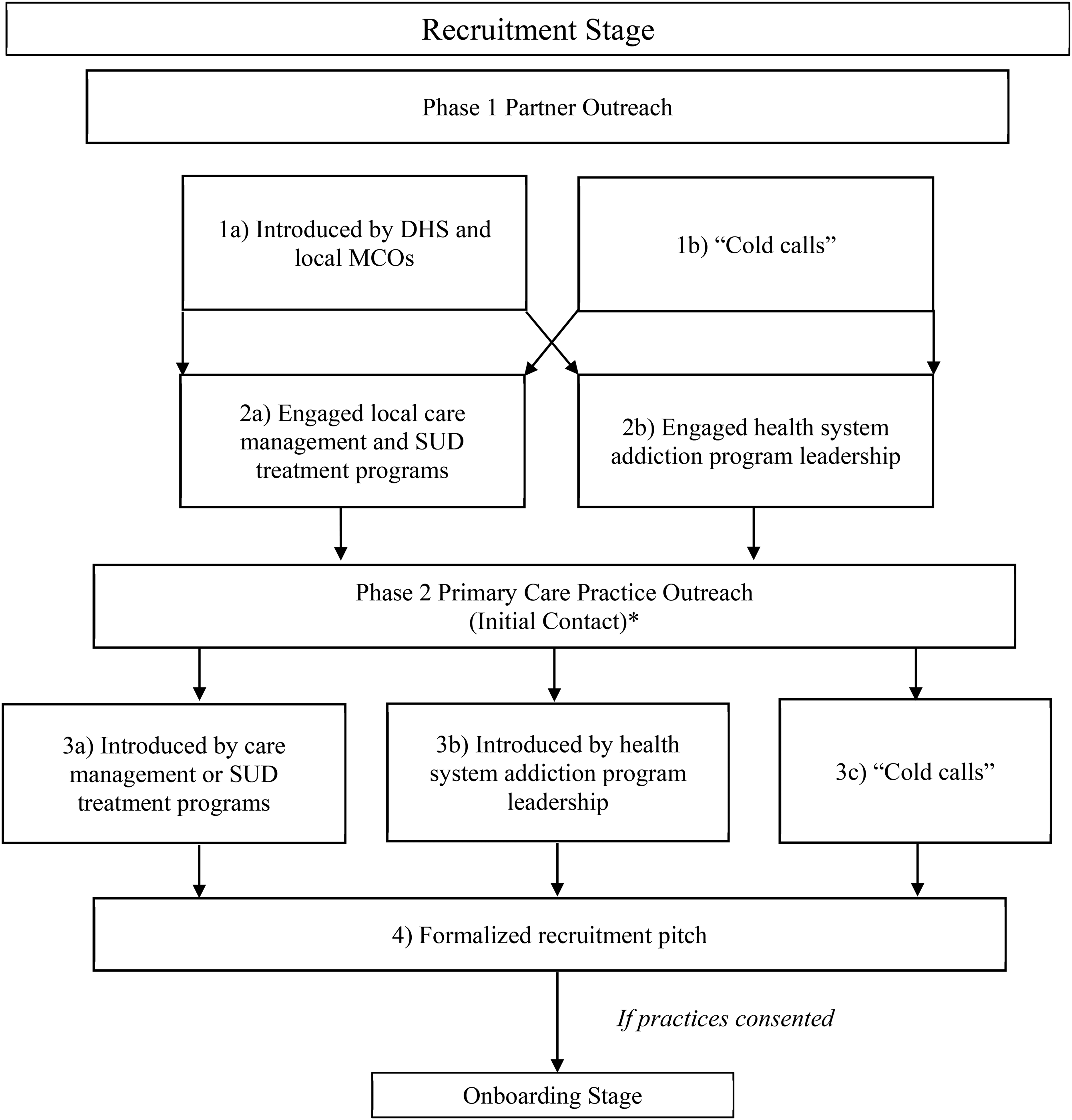
Two-Phase Recruitment Process for Rural Access to Medication Assisted Treatment in Pennsylvania Project (Project RAMP)
In the second phase (practice outreach), leadership or practitioners of identified practices were contacted via introduction by care management or SUD treatment programs, health system addiction program leadership, or via “cold calls.” During initial phone calls with prospective practices, the Implementation Team delivered a short, scripted “pitch” about the project and the general need for improving access to MOUD in rural areas. The objective of these calls was to schedule a virtual or in-person meeting with practice leadership and providers, during which they received a formalized recruitment presentation (and an accompanying packet of factsheets) highlighting the anticipated proportion of patients within their practice suffering from OUD/SUD and the general lack of SUD identification through screening and successful referral to services in the United States. Consistent with the STF, the recruitment presentation emphasized the shared vision between the project team and practices as well as the benefits of enhanced coordination with care management service providers and explained aspects of the RAMP approach to supporting MOUD adoption including (1) an individualized implementation process to improve clinical workflow; (2) HIE/CQI activities to support clinical care improvement; (3) provision of concierge technical assistance throughout the implementation process; (4) teleconsultation with physician experts; (5) revenue generation from program-specific activities (i.e., screening, referrals, MOUD-associated activities, care management, etc.); (6) provision of free DATA 2000 waiver training; and (7) provider participation options regarding giving and receiving MOUD treatment referrals, and the option to provide treatment with extended-release naltrexone (also called naltrexone-XR), buprenorphine, or both buprenorphine and naltrexone treatment. Also emphasized during this time was the potential impact that improving provider knowledge about a patient's SUD treatment status and providing referrals to care could have on patient outcomes (Substance Abuse and Mental Health Services Administration, 2020). Occasionally, the Implementation Team would present a modified version of this recruitment pitch (i.e., adjusting presentation delivery of the pitch for different audiences and/or time slots) for a broader audience at network-sponsored recruitment events (rather than individual practices).
Anticipated questions and answers were gathered from project partners and developed into a frequently asked questions (FAQ) document. After the practice or system verbally committed to participation in the project, participants provided insight into how the program could be integrated into their workflow and result in improved patient outcomes. These insights helped the Project RAMP team to engage new provider groups. Occasionally, project partners provided direct support to the Program Evaluation and Research Unit team in conducting recruitment calls and on-site events at healthcare systems, offering testimonials on outcomes supported with data to encourage participation by prospective providers.
Integrated Care Model Pre-Implementation Processes
Once recruited, Project RAMP's Implementation Team designed an implementation approach based on the STF principles and tailored to each site (Scott & Pringle, 2018), then held onboarding meetings with each practice where “MOUD Champions” were identified. In Project RAMP, MOUD Champions promoted MOUD adoption, assisted in coordinating and completing key project activities, as well as facilitated the recruitment of additional practices (Miech et al., 2018). Champion roles included MDs, DOs, nurse practitioners, physician assistants, medical assistants, practice managers, counselors, network directors, care management support specialists, and administrative staff.
The Implementation Team then administered organizational health assessments to each practice to assess their system levels based on the domains of the STF (e.g., leadership, organizational behavior, organizational structure) (Scott & Pringle, 2018). Practices were also asked to provide patient and staff demographics as well as a summary of current SUD screening and treatment processes. These results informed ICM implementation in terms of protocol development, training, data collection, CQI processes, and evaluation. The STF permitted Project RAMP to address issues within the organizations implementing the ICM, create conditions for successful organizational change, and facilitate MOUD adoption. Throughout ICM implementation, the Implementation Team provided on-demand technical assistance using the Lean Principles of teacher/mentor relationship to offer individualized problem-solving support and additional resources (Womack et al., 1991).
Key Informant Interviews (KIIs)
After completing the MOUD implementation, the Project RAMP Evaluation Team conducted semi-structured KIIs with the MOUD providers and clinical staff to assess the impact of the ICM and implementation team on enabling MOUD services. During the interviews, the team collected data to (1) understand the facilitators and barriers to MOUD adoption in rural primary care settings, and (2) receive feedback on Project RAMP. Providers received US$100 for participating. Qualitative data were audio-recorded, transcribed, and imported into NVivo 12 for data management and analysis. Once the data was coded, the Program Evaluation and Research Unit Evaluation Team utilized both inductive and deductive approaches to identify common barriers and facilitators to MOUD adoption at the project sites, with a focus on facilitators that enabled site providers to implement the ICM and adopt MOUD despite known barriers and challenges. A codebook was created with a priori codes based on the interview guide as well as emergent codes grounded in the data (after a process of open coding the transcripts). Two coders (Bridges and Taber), independently coded three transcripts, then met to discuss coding application agreements and disagreements, then refined the codebook accordingly. The current article focuses only on responses related to motivations to engage in Project RAMP. A more detailed description of the methodology and comprehensive KII results related to implementation outcomes will be reported separately (Bridges et al., 2022).
Results
Recruitment Outcomes
A total of 134 primary care practices spanning 17 health systems, four private practice groups, and 23 Pennsylvania counties were contacted for participation in the first recruitment phase. Of the 134 practices contacted, 108 practices declined to participate. Approximately 540 total contact attempts were made with the non-participating practices to engage them in the project. Only 23 practices provided explicit reasons for declining to participate. The remaining 85 practices were unresponsive to outreach attempts and were ultimately classified as “declining” participation (per the Implementation Team's recruitment policy, at least five outreach attempts had to be made before classifying an unresponsive practice as a “decline”). Of the 23 practices that provided a reason for declining to participate, 48% indicated a lack of interest, 26% indicated a lack of health system support for implementation, including a lack of reimbursement structure, and 26% indicated capacity concerns, including competing priorities in managing other chronic conditions and the time needed for training and implementation.
Of the 134 practices that were contacted, 26 practices opted to participate—exceeding the target of 24 and equating to an overall recruitment rate of 19.4%. The final 26 participating practices included nine health systems and two private practice groups spanning 13 counties across Pennsylvania, with the furthest practice located 240 miles from the Implementation Team. To simplify project activity management and coordinate activities of practices within the same practice or health system, some individual PCP practices were combined into one project implementation “site” and are therefore referred to and analyzed as “sites” moving forward. The Implementation Team managed 17 project sites (composed of 26 primary care practices) from recruitment through full implementation.
The time duration of the recruitment stage varied considerably across sites. Specifically, there was a mean of 65 days and a median of 49 days from first contact to project onboarding. The shortest recruitment stage occurred in 12 days, while the longest recruitment stage occurred in 176 days. Table 1 provides descriptive statistics on the characteristics of the sites recruited. For example, at the time of onboarding (i.e., Pre-Implementation), the 17 project sites had 71 practicing PCPs and 148 full-time equivalents (FTEs) clinical staff. Project sites had a range of 2–10 providers, 3–30 clinical staff, and 1–2 MOUD Champions per site. Nine of the project sites had providers that were already DATA waivered. One site prescribed only buprenorphine, two sites prescribed only naltrexone-XR, four sites prescribed both, and two sites prescribed neither medication despite the PCPs having DATA waivers. Of the 17 project sites, eight sites were conducting some form of SUD identification or prevention screening, but inconsistently applying clinically validated or formalized screening tools or protocols.
Pre-Implementation Characteristics of Project RAMP Sites Assessed at Onboarding

Note. N = 17 sites. MOUD = medication for opioid use disorder; SUD = substance use disorder; SBIRT = Screening, Brief Intervention, Referral to Treatment; FTE = full-time equivalent; N/A = not assessed.
Buprenorphine treatment slots calculated by summing waivered provider limits.
Key Informant Interviews
KIIs were completed with 27 MOUD providers and clinical staff from 12 (of a possible 17) project sites between April 2019 and May 2020 representing a 70.5% response rate. Five project sites declined participation in KIIs due to a lack of interest or time (29.5%). Twenty-five of the interviews were with a single interviewee and one interview had two participants. The average KII was 47 min. The KIIs identified motivations driving providers and staff to engage in Project RAMP as well as ways in which the Project RAMP approach specifically facilitated site engagement and MOUD implementation. Themes and illustrative quotes from providers can all be found in Table 2. The illustrative quotes in Table 2 have also been numbered for ease of reference within the text results below.
Themes and Accompanying Provider Quotes From Key Informant Interviews

Note. MOUD = medication for opioid use disorder; Project RAMP = Rural Access to Medication Assisted Treatment in Pennsylvania Project.
Motivation to Engage in Project RAMP
Many nurses and office managers viewed project engagement and providing MOUD services as part of their job, dictated to them by leadership or physicians. For example, in response to the question, “How did your practice become involved in Project RAMP?” one informant simply stated (Table 2, Quote 1): “Doctor came back and said, ‘We’re doing this.’”
Other providers highlighted the financial incentives associated with being a Rural Health Clinic and National Health Service Corps site, including higher service reimbursement rates and student loan repayment programs for staff (Table 2, Quotes 2 and 3). While providers generally felt that providing MOUD was part of their job, many responses reflected a sense of professional obligation for providing high-quality, evidence-based, person-centered care (Table 2, Quote 4). Because of their rural status, providers felt a heightened sense of professional and personal obligation to fill critical MOUD service gaps in their rural communities (Table 2, Quotes 5–7). While some providers formed these opinions and motivations in part through MOUD exposure in their training programs and at professional conferences (Table 2, Quotes 8 and 9), others were driven to provide MOUD due to personal experiences with substance use disorder (Table 2, Quotes 10 and 11).
Discussion
The goal of Project RAMP was to increase rural primary care patient access to MOUD and integrated care. The present article evaluated the efficacy of the recruitment approach used for Project RAMP to recruit rural PCPs to implement a MOUD-focused integrated care model. We described a two-phase PCP recruitment strategy which included leveraging the support of health system leadership to open doors to network-sponsored recruitment events and provider introductions. Leveraging “early MOUD adopters” within the health system also was important for identifying and gaining commitment in the initial recruitment phase. Results showed that the Project RAMP recruitment approach successfully recruited 26 sites to participate, exceeding the Project's target of 24 sites, and there was a median of 49 days from first contact to project onboarding. Findings from the KIIs highlighted the value of engaging PCPs by connecting to a shared vision (i.e., improving the quality of patient care) as well as addressing participation barriers such as lack of training or resources via concierge technical assistance, training, and expert consultation.
The original recruitment target for Project RAMP was 24 sites; the Implementation Team exceeded that target by successfully recruiting 26 sites from a potential pool of 134 translating to a recruitment rate of 19.4%. The Project RAMP recruitment rate also exceeded rates that have been reported in recent publications on implementation studies in similar settings with a comparable level of intensity in terms of implementation strategies and integration (Ford et al., 2021). For example, a recent publication describing the recruitment rates for a study implementing strategies to improve access to addiction and psychotropic medications reported a response rate of 10.4% in response to recruitment letters (Ford et al., 2021). Other studies reporting higher recruitment rates (e.g., 75%–90%) tend to draw from self-selected participation pools (e.g., sampling from providers who have already agreed to be contacted for project participation) or involve relatively less intensive/complex designs (e.g., brief surveys) (Balio et al., 2022; Varley et al., 2020). Additionally, our findings indicate considerable variability in the time duration of the recruitment stage across sites. These findings may suggest a need for tailored recruitment approaches to successfully recruit and engage rural primary care providers across different sites. Indeed, prior research has indicated that implementing MOUD in rural primary care is more likely to be successful if implementers are attentive to the needs of individual providers, are flexible, tailor recruitment and implementation strategies, and provide ongoing support to meet individualized needs (Nourjah & Kato, 2021; Pinto et al., 2019).
KII findings from the current project also highlight broader systemic problems (e.g., lack of providers in rural counties). While some of the proposed solutions exceed the scope of Project RAMP's purpose, they do offer insight into low-cost recruitment and engagement strategies. For example, advertising existing financial incentives for health systems (e.g., higher service reimbursement rates) and providers (e.g., student loan forgiveness) for providing MOUD in rural counties as a potential benefit to participation is a no-cost way to engage leaders, providers, and clinical staff (Blanco et al., 2020). Furthermore, during the KIIs many providers shared a desire to provide the highest quality care to patients to better serve their communities, fulfill their mission as healthcare providers, and support people like themselves or close family/friends with SUD. This indicates a mechanism of engagement rooted in shared values (e.g., providing compassionate, evidence-based care) and honoring their experiences that go beyond financial incentives or solving logistical hurdles. Such recruitment efforts may prove particularly effective when seeking to identify and engage MOUD Champions early on to facilitate long-term implementation success. Pervading barriers such as internalized stigma that create resistance to any engagement or implementation may prove particularly challenging for projects in the recruitment phase. While the Project RAMP Implementation Team had some success by identifying/employing MOUD Champions, using informal networking opportunities, and having Implementation Team staff trained to handle challenging conversations (e.g., using motivational interviewing techniques, countering stigmatizing beliefs), other strategies such as community-wide anti-stigma campaigns may serve as a fruitful preparatory activity for recruitment (Atkins et al., 2020).
Several limitations should be noted. First, as is common with implementation and research initiatives, the amount of data that was able to be collected in Project RAMP was constrained by limited time, resources, and staffing capacity. Because Project RAMP had site-level benchmarks in terms of recruitment (e.g., recruiting 24 practices) and implementation (e.g., having at least one provider trained in MOUD and one MOUD Champion on site), more detailed staff-level data is not currently available (e.g., MOUD Champion turnover rate). Future projects should consider incorporating multi-level sampling schemes and data tracking for subsequent analysis. Relatedly, only 12/17 sites participated in the KIIs, yielding a response rate of 70.5%; the present findings may be biased to more favorable responses to Project RAMP or not represent the feedback of the remaining who may have had greater time, resources, and staffing constraints. Furthermore, the present article focused on recruitment outcomes. The fact that most practices who opted not to participate did not provide reasons for non-participation is not surprising, however, it does limit our ability to address what the barriers to their participation may have been. Future projects should attempt to garner more detailed non-response data to improve future recruitment efforts. Lastly, this project was conducted before the onset of the COVID-19 pandemic; more recent literature has noted the exceptional impact the pandemic has had on healthcare, public health, and the research systems that exacerbate recruitment challenges (Balio et al., 2022). As workers within these systems continue to confront the direct and residual effects of multiple pandemics (e.g., trauma, burnout), future efforts to integrate evidence-based practices will need to incorporate additional structural and financial supports as well as flexibility around relationship building (e.g., virtual presentations vs. In-person recruiting events) (Balio et al., 2022; Mazurenko et al., 2022).
Replication, Sustainability, and Extensions of Project RAMP
The proposed approach to recruiting practices and implementing MOUD through an ICM could be scaled to other outpatient care settings and systems. As of November 2021, 12 of the 15 sites (80%) that implemented the Project RAMP model and provided MOUD are still providing MOUD using some or most of the system components within the ICM. This continued use of the Project RAMP model is occurring despite the removal of the HIE/CQI process in 2020. The recruitment and implementation strategies for Project RAMP have already been expanded to include 28 additional practices across 12 counties, building the foundation for creating a systematic recruitment and MOUD implementation model to reduce overdose deaths in rural Pennsylvania. Future research focused on characterizing the mechanisms underlying positive organizational changes (e.g., organizational health, provider self-efficacy) (Lewis et al., 2021; Shapiro et al., 2021; Vax et al., 2021) as well as the extent to which organizational or implementation metrics have a demonstrated impact on the patient experience (e.g., individualized care; reduced wait times; appropriate care transitions; wraparound services) is needed. Consistent with recent calls for more patient-centered care (Marchand et al., 2019), future research using these systems to characterize the impact of implementation metrics on patient-reported recovery outcomes (cf., administrative claims data) is needed (Blasi et al., 2021).
Conclusion
There is no one-size-fits-all approach to implementing MOUD in primary care. Engaging providers requires awareness of barriers and facilitators to adoption at the health system, practice, and provider levels. The Project RAMP recruitment strategy was successful, in part, by establishing a strong commitment from health system leadership and individual practices as well as leveraging successfully recruited providers/sites to recruit additional sites. The ICM aided recruitment and engagement efforts by successfully addressing prescribers’ perceived barriers to providing MOUD (e.g., paying providers fees for obtaining DATA 2000 waivers) as well as facilitating better communication among administrators, PCPs, behavioral health professionals, care managers, and patients. Future initiatives to increase MOUD capacity in rural counties should be prepared to (1) leverage the support of health system leadership in recruiting new PCPs; (2) articulate how they plan to address provider barriers via concierge technical assistance, training, and expert consultation; and (3) facilitate connections with local behavioral health providers and develop an ICM for MOUD via case management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality [grant number R18-HS025072].