
Abstract
Background
Clinicians, health care organizations, and families demand better and more accessible children's mental health services with greater patient engagement. The I-InTERACT-North program was developed for children following traumatic brain injury and adapted for a transdiagnostic neurological and neurodevelopmental focus, with a recent transition to a stepped-care model. To date, the program has been exclusively provided within research studies; however, demand for its clinical use is growing. Implementation frameworks provide essential guidance regarding facilitators and barriers of clinical implementation under real-world conditions. Similarly, intersectionality evaluation can provide insights to develop equitable and inclusive health care practices. Informed by the Consolidated Framework of Implementation Research 2.0 (CFIR) and recent intersectionality supplement, the objectives were to examine the perspectives of parents/caregivers and clinical partners involved in the I-InTERACT-North program to identify (a) facilitators and barriers to inform the scale and spread of the program, and (b) equity, diversity, and inclusion (EDI) considerations to integrate in future clinical implementation.
Method
This study used a qualitative descriptive design with focus group methodology. Participants included parents/caregivers and clinical partners. Semi-structured focus groups were conducted virtually. Focus group data were coded inductively and deductively using CFIR 2.0. The team reflected on intersectionality in the data, coding results, and broader context of the program's history.
Results
Positive perceptions of the innovation's relevance and adaptability were echoed across focus groups. Prominent facilitators included the program's adaptability, personalized, flexible format, and knowledge dissemination. Barriers included geography, technological accessibility, and workflow, with participants stressing the importance of tailoring to culture, language, and neurodiversity. Feedback from participants aligned with 10 reflective prompts highlighted within the CFIR intersectionality supplement pertaining to families’ intersecting categories, diverse intervention experiences, and information access.
Conclusions
Identified facilitators of I-InTERACT-North implementation extended across program knowledge sharing and recruitment. Recommendations included directions for clinical and system integration to facilitate scalability.
Plain Language Summary Title
Transitioning a stepped-care mental health parenting program (I-InTERACT-North) from research to clinical care: Recommendations from families and clinicians
I-InTERACT-North is a virtual positive parenting support program designed for neurodiverse children (i.e., Brain Injury, Attention Deficit Hyperactivity Disorder (ADHD), Autism (ASD)). Participation in this program improves parent-child relationships, child behavior, and parent stress. To enhance feasibility and better meet families’ needs during the pandemic, our team adapted to a stepped-care approach. Stepped-care offers effective treatment tailored in intensity and level of therapist involvement to family needs. Using focus groups of parents and clinical partners, the current study identified facilitators and barriers to inform optimal clinical implementation and expansion of the program beyond our institution. Suggestions included strategies to inform more families about the program, build connections with community agencies, and ways to promote patient diversity and inclusivity. Recommendations also pertained to fitting and funding the program. Results overall highlighted the benefit of ongoing work with families to design and inform the program's clinical implementation.
Keywords
Introduction
Clinicians, health care organizations, and, most importantly, families demand better patient engagement and accountability within children's mental health services. In our work as mental health clinicians and scientists, this is particularly salient for children at known risk for mental health concerns due to early acquired brain injury (ABI) and/or neurodevelopmental conditions. I-InTERACT-North is a virtual parenting program based on evidence-supported positive parenting principles and interventions (ESPIs) that promote caregiving skills (i.e., responsiveness and consistency). It also provides psychoeducation regarding the impact of early medical or neurodevelopmental conditions on socio-emotional and behavioral outcomes. ESPIs have been extensively tested for effectiveness in the treatment of early child behavior and are considered to offer universal mental health prevention strategies (Kaminski et al., 2008; Kirkbride et al., 2024; Nowak & Heinrichs, 2008; Schuhmann et al., 1998; Webster-Stratton et al., 2011). I-InTERACT was initially designed for children recovering from traumatic brain injury (Wade et al., 2017).
Our group co-designed and tested a transdiagnostic version informed by these principles, called I-InTERACT-North. This program was meant for children with early medical and neurodevelopmental conditions in place of diagnosis-specific service provision. Several small sample trials demonstrated efficacy across conditions (Burek et al., 2021; Williams et al., 2022). Informed by pandemic experiences, we revised the program to follow a stepped-care model (Deotto et al., 2023). Positive evidence of feasibility, adherence, acceptability, and efficacy in improving parent skills and child behaviors was reported, with strong consensus on the program's relevance for future clinical implementation (Deotto et al., 2023).
In its original full format, I-InTERACT-North combined seven online learning modules with 1:1 parent coaching via videoconference in the family's home. The stepped-care adaptation follows the Bower and Gilbody (2005) model with three steps: (a) guided self-help (podcast), (b) brief parent support, and (c) longer-term support for families with more significant concerns. The initial step includes a 30-min podcast discussing parenting strategies during times of stress. In Step 2, parents complete two online learning modules and two accompanying 1:1 virtual sessions with a therapist who introduced positive parenting and special play time (SPT). SPT involves 5 min of focused parent–child play to practice skills of labeled praise, reflecting, and describing what the child says or does. Following SPT, parents receive coaching in parent–child play directed toward these skills. Step 3 provided families with five additional learning modules and 1:1 virtual coaching sessions with the same therapist. Later sessions present more complex behavior strategies, such as implementing home rules and consequences. Criteria for graduation to subsequent steps are based on increasingly higher score thresholds of baseline child behavior ratings, current top problems, parent mental health ratings, and in-session observation of positive parenting skills. Program intensity is matched to family needs with a collaborative discussion of parent preferences.
Implementation studies of positive parenting interventions have predominantly been conducted within community settings, among children and families considered at-risk due to child maltreatment or household dysfunction (e.g., caregiver mental illness, substance use, incarceration). Salient implementation facilitators identified in well-known community programs, Incredible Years Parenting Program (IYPP) and Triple P, include parent and agency readiness and opportunities for ongoing clinician coaching (Cooper et al., 2022; Côté & Gagné, 2020; Furlong & McGilloway, 2012; Olofsson et al., 2016; Romney et al., 2014; Sanders, 2023; Sanders & Turner, 2005). Common established barriers include a lack of institutional resources and mental health professionals. Family-specific barriers include housing and poverty needs, parent mental health, and transportation.
To our knowledge, there have been no implementation studies of adapted positive parenting programs like I-InTERACT-North within hospital settings for children with early brain injury. Psychosocial intervention implementation efforts in similar adult neurological populations (i.e., stroke, traumatic brain injury) have identified barriers such as clinician time pressures, shortages, inconsistent funding, and intervention accessibility (Wong, 2023).
To guide the implementation of I-InTERACT-North in hospital settings, we conducted focus groups to identify facilitators and barriers from family and clinician perspectives. Initial focus group prompts were guided by a general implementation framework that asked about facilitators and barriers to program scale-up and equity, diversity, and inclusion factors that can optimize intersectionality in intervention adaptation. This study used the Consolidated Framework for Implementation Research (CFIR 2.0) to recode focus group data and examine results through a determinant lens. CFIR 2.0 provides a menu of constructs arranged across five domains that provide a practical framework to help guide systematic assessment of potential barriers and facilitators (Damschroder et al., 2009, 2022). Knowing this information can help guide the tailoring of implementation strategies and needed adaptations and explain outcomes (i.e., What helped? What got in the way?; Nilsen, 2015).
From the outset, the development of I-InTERACT-North has included parents from diverse sociodemographic, child medical, and disability backgrounds who have actively engaged in the co-design of the program (Ford et al., 2022; Williams et al., 2018). Program co-design has led to the virtual and stepped-care format by prioritizing diversity in availability, work schedules, medical diagnoses, and level of need (Deotto et al., 2023; Ford et al., 2022; Williams et al., 2018, Williams et al., 2022). The intervention manual and training prepare therapists to sensitively consider intersectional identities by inquiring about the role of religion, faith, culture, and community involvement to gather a holistic perspective of parenting approaches and family structures, which can then be integrated into program delivery (Wade et al., 2024). To further evaluate how the program might address various intersectional factors concerning disability, race, and socioeconomic status, we leveraged the intersectional supplement to the CFIR framework (Rodrigues et al., 2023). We hoped that even post-hoc, this lens would help us consider facilitators and barriers more broadly to support a more equitable implementation of the I-InTERACT-North program (Cole & Duncan, 2023; Bowleg, 2021). It would have been preferred if this study had been guided by the framework from the outset; however, post hoc re-analysis offered value in demonstrating how implementation frameworks can be used to analyze and interpret participant-driven datasets that reflect broad conceptualizations of program determinants.
The primary study objectives were to examine caregiver and clinical partner perspectives of the I-InTERACT-North stepped-care adapted service model to:
Identify implementation facilitators and barriers to expanding I-InTERACT-North (i.e., co-design strategies to support the program's scale and spread). Reflect on future intersectional considerations for recruitment, scale-up, and implementation.
Method
The study employed a qualitative descriptive design utilizing focus group methodology (Sandelowski, 2010). This approach is appropriate for studying complex processes concerning patient, clinician, and organizational-level factors associated with implementing evidence-based interventions and answering multifaceted questions about intervention acceptability, adaptation, scale, and spread. It can also provide first-hand insight into how knowledge users and clinical partners experience and make care decisions (Hamilton & Finley, 2019). Ethics approval (REB # 100072960) was obtained. We used the consolidated criteria for reporting qualitative studies (COREQ; Tong et al., 2007).
Participants
Parents/caregivers and clinical partners (e.g., senior mental health administrative leaders and clinicians) were recruited to inform program implementation readiness and co-design adaptations for larger-scale clinical implementation efforts.
Parents/Caregivers
We engaged in purposive sampling to recruit parents/caregivers who had participated in the I-InTERACT-North program between 2019 and 2022 and who had consented to be contacted for future studies at one of four Ontario centers: [Holland Bloorview, The Hospital for Sick Children, University of Western Ontario, and Queen’s University]. Inclusion criteria for the current study were as follows: (a) parent/caregiver of a child aged 3–10 years, and (b) prior participation in I-InTERACT-North to any extent (i.e., one or more sessions).
Clinical Partners
Clinical administrators and executive leadership with mental health expertise from pediatric hospitals and community mental health clinics in Ontario, Canada, were invited to participate. We sought to recruit a diverse group of experts in mental health service administration, leadership, and delivery.
Procedures
Recruitment
The research coordinator emailed information letters to parents/caregivers and clinical partners. For parent/caregiver participants, one 2-hr semistructured focus group was held. Two 2-hr focus groups were facilitated to optimize scheduling for clinician partners. All focus groups were conducted virtually (i.e., Zoom videoconferencing). Participants were provided a monetary token of appreciation (a $50 gift card).
Focus Groups
Before the focus group, all participants were provided a single-page overview of the focus group structure and starter questions (see Appendix A). Focus groups were organized and led by an independent co-design facilitator (JR) with a business administration background (MBA) and extensive experience conducting focus groups that promote balanced discussion by applying iterative strategies and minimizing power differentials between the interviewer and respondents. A facilitator independent of the program was selected to minimize bias: she was familiar with virtual interventions but had no prior connection to I-InTERACT-North. A post-doctoral fellow (AD) from our team attended all focus groups to present briefly on the stepped-care model but did not actively engage in discussions to minimize bias. Focus group approaches were informed by the CIHR Strategy for Patient-Oriented Research (SPOR) guiding principles (mutual respect, co-building, inclusiveness, and support). In the design and strategizing phase, the focus group facilitator reviewed the program's feasibility, acceptability, and efficacy data (Deotto et al., 2023) and used it to design the focus group protocol (see Appendix B).
The focus group began with a conversation about participants’ experiences with I-InTERACT-North and general mental health interventions. Then, it focused on perceptions of the I-InTERACT-North stepped-care model, with questions and probes to uncover facilitators and barriers to access, implementation, equity, diversity, and inclusivity. Semi-structured open-ended questions probed perceptions of stepped-care (e.g., How do you feel about the “steps” of the program? Do they make sense to you?), future engagement and scalability (e.g., What are the strengths, challenges, and opportunities for the program? What changes/strategies would you recommend to mitigate barriers and facilitate implementation?), and considerations for equitable access and optimal inclusivity (e.g., How might we redesign elements of the program to improve equitable access and ensure that all families feel included?).
For clinical partners, parallel questions probed generic barriers and enablers to program spread and scale in both inner (hospital) and outer (community) settings, future engagement, and scalability (e.g., What leadership, organizational capacities, and resources can be leveraged? What changes/strategies would you recommend to mitigate barriers and facilitate implementation?) and equitable access and optimal inclusivity considerations.
Co-Design
The specific focus group objectives were translated into a series of questions (see Appendix B) and activities on Miro, an online whiteboard for visual collaboration (https://miro.com/about/). The Miro board was leveraged to keep participants focused on the focus group goals and the discussion progress and was essential for data capture and member checking. The approach allowed for divergence and convergence in the discussion. As participants worked through activities, the facilitator captured each challenge, sentiment, idea, or detail of a narrated experience onto a virtual memo (akin to a “post-it” note), resulting in inductively developed data units. Member checking was done throughout focus groups, during which the facilitator restated and summarized information through the virtual memo notes and then allowed participants to consider accuracy.
Analyses
Qualitative data were inductively analyzed using reflexive thematic analyses using interpretive description (i.e., bottom-up, interpreted from raw focus group data; Thorne et al., 2004; Thorne, 2008) and deductively (i.e., top-down, guided by the CFIR 2.0; Damschroder, 2020; Damschroder et al., 2022). First, during focus groups, the facilitator engaged in in vivo coding, in which codes were developed from participants’ own words and represented the most basic data units. As discussions progressed, memos were inferentially organized into categories, which participants iteratively reviewed for accuracy and consolidation of defining properties.
Inferentially derived categories were then deductively analyzed using the CFIR 2.0 framework and sorted into predetermined theory-based domains and constructs by two researcher team members. Team members worked independently and then came together to reach a consensus. To ensure trustworthiness and rigour, analyses employed prolonged engagement, peer debriefing, and reflexivity (Lincoln & Guba, 1985). Team members independently completed concept-driven, deductive coding for 100% of the data. Regarding inter-coder reliability, 96% overlap was achieved in theme categorization. Minor discrepancies were resolved through consensual validation, where the content of categories and corresponding CFIR 2.0 construct definitions were discussed at length (i.e., prolonged engagement and peer debriefing). Team members employed reflexivity via attention to prior experiences, assumptions, and beliefs that could influence the research process (Lincoln & Guba, 1985).
Focus groups were conducted before the publication of the CFIR intersectionality supplement (Rodrigues et al., 2023). As such, the two coders reviewed the set of reflection prompts provided post hoc. They considered how they might apply to deductive findings, generating a list of applicable prompts deduced from the CFIR 2.0 analyses.
The two team members who led coding reflexively identified their respective positionalities as a white female post-doctoral researcher in child mental health (AG) and a white female, able-bodied neuropsychologist and researcher who provides clinical services for neurological and pediatric populations (AD). The study's first author (TW), responsible for study design, manuscript preparation, and overseeing thematic analyses, identifies as a white female scholar, therapist, and neuropsychologist.
Results
From the larger sample who consented to be contacted for future research, 24 parent/caregiver participants were purposively sampled to achieve maximum variation in parent/caregiver gender, family's described race and cultural background, child's condition and age, and geographic representation. Of those invited, 11 parent/caregiver participants expressed interest in participating, and 9 (8 from the stepped-care model and one from the original program) attended, including two parents who attended with their partners. A subset of focus group participants had completed one initial session from the stepped care model. Although not a full decline in participation, the opinions and perspectives of these participants offer valuable information on potential program barriers and reasons for stepping down. All participants identified as parents, and “parent” will be used for subsequent description. Nonparticipation was due to travel and family illness. As shown in Table 1, children's diagnoses varied, including neurodevelopmental disorders (i.e., ADHD, ASD) and medical (i.e., Stroke, Epilepsy, Congenital Heart Disease) conditions. Despite oversampling, most parents identified as Caucasian (77%), but with representation from Black, Indigenous, and Asian parents, proportionate to national census demographics (Statistics Canada, 2022).
Parent, Child, and Family Characteristics.
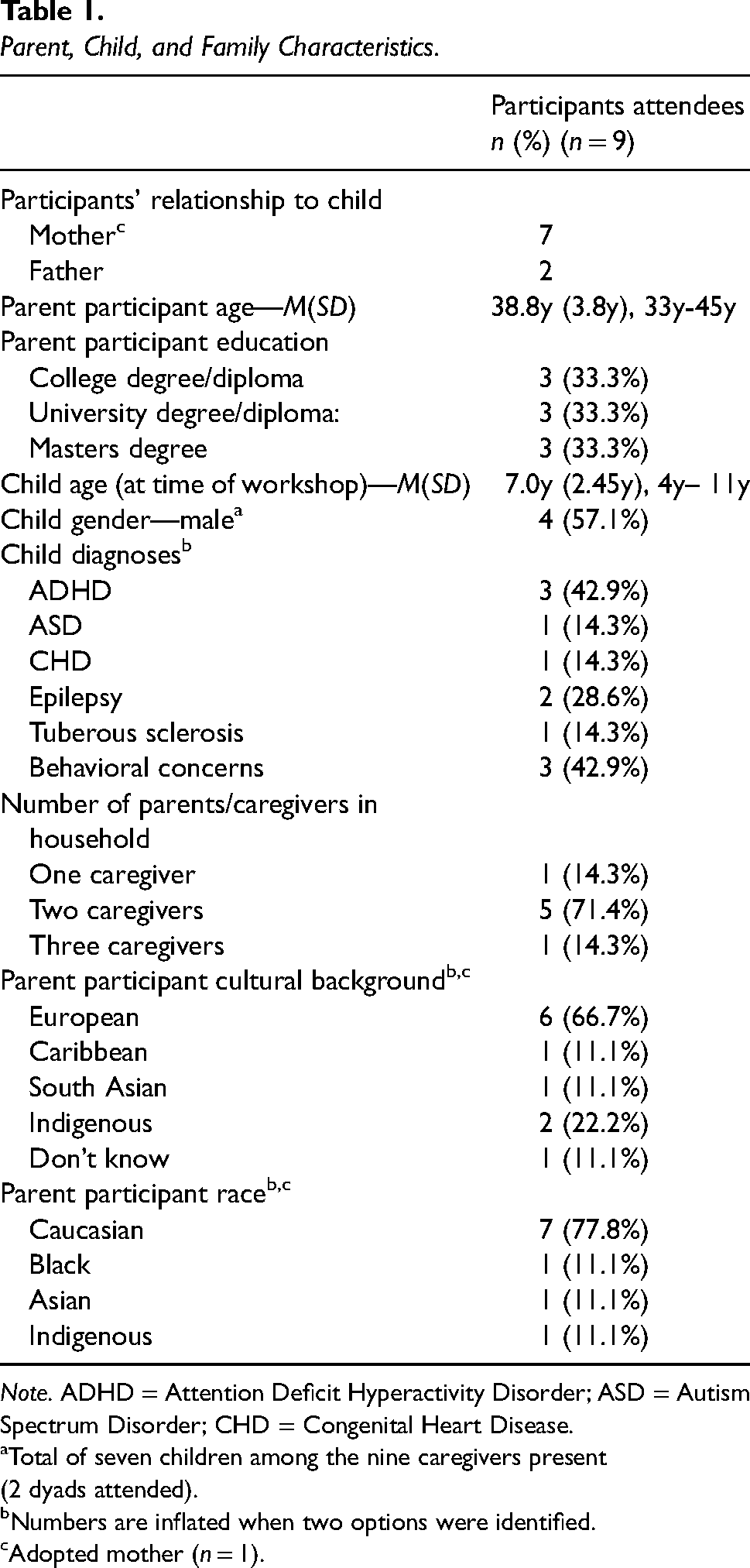
Note. ADHD = Attention Deficit Hyperactivity Disorder; ASD = Autism Spectrum Disorder; CHD = Congenital Heart Disease.
Total of seven children among the nine caregivers present (2 dyads attended). bNumbers are inflated when two options were identified. cAdopted mother (n = 1).
From the larger sample of clinical partners who consented to be contacted for future research, 17 individuals expressed interest in participating, and 15 participants attended (Table 2). Nonparticipation was due to scheduling.
Clinical Partner Characteristics.

Note: Numbers are >N as some clinical partners hold multiple roles
Objective 1: Implementation Facilitators and Barriers to Expanding I-InTERACT-North
Facilitators
As shown in Table 3, there were several identified facilitators with regard to the I-InTERACT-North innovation reflected in comments about the program's adaptability, i.e., “I like the stepped approach, and being able to build on learning,” and personalized and flexible implementation: “Flexibility in step 3 was perfect for us because we had a wide range of issues, and sessions were tailored to that.” Parents also noted that versatile program delivery (i.e., multimodal online and/or in-person session delivery) helped meet the varying family needs and preferences. Also of direct relevance to the Innovation Domain,
Facilitators and Barriers to Inform the Adaptation and Implementation of I-InTERACT-North.

Note. CFIR = Consolidated Framework of Implementation Research.
Facilitators also included current and future partnerships and connections that may benefit program growth (i.e., schools, teachers’ colleges, family physicians, and children's social services). Clinical partners discussed the negative impact of the COVID-19 pandemic on mental health needs among young children, noting that “so many kids could benefit” from this program. Expansion of reach across settings was highlighted, and earlier intervention was also recommended to offer preventative care through partnerships with early intervention centers.
Starting slow was recommended by clinical partners to understand the system and resources needed to optimize scalability and growth. System mapping was also deemed an essential facilitator by clinical partners who encouraged the team to “really think about how this program fits into unique clinical pathways and addresses clinical needs” and to emphasize “what is unique” about the program's contribution to existing services. Participants advised implementation to “start small in one area of [the hospital] to test and apply ideas and deploy strategically so we can learn from each step of the journey.” Clinical partners also recommended starting in clinics with no other competing mental health services. In parallel, partners recommended a therapist training model that is “scalable as the program expands,” considers the diversity of professional disciplines that could be trained and standardizes training to “ensure that the fidelity of the program is maintained over time.” Clinical partners stressed the importance of governance models to facilitate implementation, noting that they “should be top-down and bottom-up,” informed by prior experiences, but also flexible to adjust to the evolution of the program's future clinical implementation. Participants especially asserted the value of “an evaluation framework to support decision-making around program needs and changes as it scales up.”
Clinical partners also discussed preparedness, and the importance of assessing readiness to understand current attitudes, cultural values and what people are prepared for/equipped to take on, with long-term recommendations to collect information that will help anticipate future barriers and facilitators to program delivery. Clinical partners also recommended an agile implementation strategy in which the team would test out and apply ideas in one clinic to test an apply new ideas strategically. The importance of building trusting relationships and teaming was also reflected: “As the program expands into the community, time and effort will need to be invested in building trusting relationships with referral sources.” Clinical partners also emphasized communication facilitators for future implementation to include: “clear, concise communications” and “information feedback to clinical areas about program response and impact.” As the program expands, clinical partners emphasized the importance of “bi-directional communication between hospital and community providers” as well as the significance of building trusting relationships with referral sources in the community. Furthermore, The I-InTERACT-North program was lauded for its co-design principles and continued scale-up through the lens of the family was recommended.
Marketing strategies that facilitate engagement were also encouraged. Participants shared the importance of “generat(ing) excitement early on, with a focus on how people's lives will change” and enabling referring clinicians to be able to “talk about the program and position it positively.” Clinical partners discussed the value of a “commercialization plan which can help articulate the service and its value proposition.” Testimonials were also a recommended central aspect of program promotion that should be included in marketing strategies to ensure that messaging is on point; clinical partners emphasized that “testimonials from families and providers can go a long way.”
Implementation barriers
Several relevant barriers were identified across CFIR 2.0 domains and constructs by parents and clinical partners. Geography was conceived as an essential barrier to consider from a knowledge dissemination perspective, such that “the rural and urban divide makes it harder for families not in the greater Toronto area to know about the program.” Workflow change was also highlighted as a potential barrier in scale-up, as clinical partners emphasized variable full-time clinical staffing, i.e., “it can take longer to get part-time staff up to speed and used to new workflows.” Parents further recognized program accessibility as a potential barrier and provided several recommendations to facilitate for families that may not have access to standard videoconferencing (e.g., Zoom) or computer access. Relevant recommendations included “partnering with community centres such as libraries, telemedicine sites and children's treatment centres” where families may access space and technological support.
Variable mental health communication between clinicians and parents was an identified barrier by parent participants, commenting how mental health and parenting issues are seldom discussed and how “doctors should be having open conversations about behaviour and resources, such as I-InTERACT-North” and that “once kids are doing well/recovering physically, it would be good to address [children/family mental health], and “let them know this program exists.”
Terminology was also identified as a potential barrier to program implementation. Appropriate messaging was indicated as needed to refer families sensitively without placing blame or shame on the family concerns targeted by the program. There was a specific reframing suggestion to change the program's terminology regarding “parent training” to a more positive/less evaluative emphasis on “parent coaching.”
Sustainable funding was also noted to be a potential barrier. Clinical partner participants stressed the importance of identifying a “financial model that will support maintenance” with suggestions to investigate publicly available sources of funding and how “we need to consider what pockets of money [the program] aligns with” given mental health budget limits. Parents also suggested outreach to health directors or health organizations within Ontario, the federal government and First Nations communities.
Cultural representation and language barriers were also reflected in prominent themes and recommendations for tailoring to representing all races and family types in program videos and examples to “ensure that video examples capture differences” in family experience. This was considered pertinent given that parents new to Canada must learn about “Canadian culture and school systems,” which may impact their ability to relate to program content. This also applied to neurodevelopmental diversity representation as well. Parents wanted to ensure that families were not dismissed because of language barriers, and clinical partners recommended that administrators “invest in translation materials upfront into a variety of languages.” Recommendations for adaptation also highlighted the continued expansion of existing transdiagnostic content, including updates to specific program materials, such as videos, to ensure program applicability to children of varying diagnoses and cognitive abilities. Tailoring implementation processes were also deemed central as they pertained to language and program materials.
Parents’ limited time and resources were also discussed potential barriers with participants citing that successful implementation involves interventions that “consider parent confidence, time, and childcare needs and how they may influence a family's ability to engage,” Engagement strategies included: setting family expectations: “collaborative discussions early on to talk about the goals of the program and what transitioning out of the program will look like,” as well as to consider what additional continued resources are available to program graduates. Relatedly, clinical partners recommended ongoing co-design including “think about implementation and scale-up through the lens of the family” to optimize access to knowledge and information.
Objective 2: Intersectional considerations for recruitment, scale-up, and implementation
As presented in Table 4, participants’ reflections and advice aligned with ten reflective prompts within the CFIR intersectionality supplement (Rodrigues et al., 2023). In reflecting on intersectionality and diverse patient experiences, participants highlighted that the stepped-care format allows flexibility in tailoring the intervention to specific family needs and a wide range of patient-identified concerns. The adaptability and versatility of the transdiagnostic stepped-care model were identified as a structural intervention component sensitive to family background and preferences. Parents provided further recommendations to facilitate information access to meet diverse needs, including multimodal (i.e., hybrid) online and in-person session delivery and concise session summaries (e.g., transcripts) of session content. Further efforts to address implicit or explicit assumptions included suggestions to reduce language barriers, with clinical partners advising investment in material translation upfront. Expanding program materials and online content was deemed essential for inclusivity; demonstration videos were described as somewhat outdated and represented an idealized portrayal of program skills for initial learning. Participants underscored revising the videos to present diversity and variability in race, ethnicity, ability/developmental levels, and family structure for increased relevance and to ensure the capture of differences in experiences. The call to adapt content for broader age ranges, especially younger children, was also directly relevant to intersectionality prompts, encouraging administrators to comprehensively understand the diverse patient experience.
Intersectionality Supplemental CFIR Prompts.

Note. CFIR = Consolidated Framework of Implementation Research.
Intersectionality prompts were relevant to participants’ recommended improvements in marketing strategy and appropriate messaging. Specifically, parents and clinical partners advised that program leaders consider structural and geographic inequities that can impact program participation opportunities. Attention was brought to the urban and rural divide, where families outside the hospital area may have fewer opportunities to learn about and access the program. Community partnerships were deemed essential to marketing and future program delivery to facilitate referrals, technological support, and space access.
Within the hospital, participants discussed child mental health in the context of acute and routine medical appointments to champion holistic care and serve families from the lens of prevention and early intervention. Attention was brought to the organization's assumptions held by hospital staff that could impact scalability. Clinical partners recommended that therapist training models consider the diversity of professional disciplines (e.g., psychologists, neuropsychologists, social workers, etc.). Clinical partners also noted the importance of preparedness and assessing readiness to understand current attitudes, institutional values within and among hospital services, and what people are prepared/equipped to take on. Considerations for sufficient time and space pertained to part-time staff and the bandwidth involved in adapting to new and additional workflows.
Discussion
The current study examined the perspectives of a stepped-care adapted service model among parents and clinical mental health leaders, identifying salient facilitators and barriers to inform program scale and spread. Overall, positive perceptions of the program's relevance, adaptability, and need were echoed across focus groups, and explicit steps were recommended for the program's implementation into clinical hospital settings. Identified facilitators extended across framework domains, guiding knowledge sharing, recruitment, and more extensive clinical integration and scale up.
Parent and clinical partner focus group participants identified few potential/known barriers with overall high acceptability and need for I-InTERACT-North, consistent with wide-scale acceptability of parenting interventions (Kirkbride et al., 2024; World Health Organization, 2022). All participants agreed on the importance of leveraging existing facilitators of the innovation's adaptability and inclusive design, i.e., its emphasis on supporting early mental health promotion and the adaptability of the stepped-care program that offers customizable and precise support and multi-modal opportunities to engage young families (Cross & Hickie, 2017). Participants echoed the importance of fostering and maintaining connections with community centres as potential ways to extend program access. Continued engagement of previous and new participant families was also recommended to inform and optimize long-term program scalability.
Notably, the program aligned directly with hospital-wide precision mental health initiatives, system pressures, and tension for change (Bickman et al., 2016; Delgadillo & Lutz, 2020; Lutz et al., 2020). Clinical partners emphasized that families must be considered at the center of future clinical program implementation. This generally relates to successfully adopting family-centred care and the utility of parents and caregivers as implementation drivers and champions (Barwick et al., 2020; O'Brien et al., 2015). Consistent with prior studies of community parenting programs and hospital-based implementation (Cooper et al., 2022; Côté & Gagné, 2020; Geerligs et al., 2018; Lorien et al., 2020), caregiver and clinical partners discussed the importance of communication in clinical pathways to ensure the program is recommended at the right time, with sensitive discussions and prompt referrals about family mental health needs (Williams et al., 2018, 2019). Recommendations included addressing mental health during regular clinical appointments and potential program integration barriers within current workflows and clinical staffing models. Considering the program's compatibility with existing workflows, available resources, and training were noted as facilitators for future implementation.
Discussion of the implementation process surfaced many implementation strategies commonly identified in community parenting programming, including assessing organizational readiness, collaborative teaming, tailoring to address language barriers, and those specific to parents’ efficacy and expectations (Furlong & McGilloway, 2015; Morawska et al., 2011; Romney et al., 2014). Implementation process facilitators discussed in clinical partner focus groups echoed common recommendations, including bidirectional communication, generating excitement early on, and using agile implementation strategies for individual clinics that can inform needs, clinical flow, and clinical pathways (Damschroder et al., 2009, 2022). Clinical partners also described well-known barriers and facilitators regarding funding and facilitating trust among community partners that may lead to clinical partnerships with community agencies to address needs among younger children and their families, and operational partnerships to facilitate access to space and technological support.
Several valuable insights regarding barriers and potential facilitators were gathered directly from focus groups and team reflections on the essential intersectionality considerations. These included the translation of handouts of core program material and program revisions to reflect broader diversity in race, ethnicity, and family structure. Future initiatives may also consider additional culture-specific adaptations of the I-InTERACT-North program. For example, the PersIN framework demonstrated implementation feasibility in personalizing similar community-based parent–child interaction therapy (PCIT) content to facilitate cultural responsiveness while maintaining the fidelity and efficacy of the original intervention (Yeh et al., 2022). In our study, parents also consistently called for more realistic portrayals of parent–child interactions common among neurodiverse children.
Finally, although access to the technology necessary for virtual program participation has improved dramatically, it remains an access and privacy barrier for many families. To address this, we coordinate program appointments with families at community centers and provide options for in-person sessions, which may involve meeting with families alongside medical visits.
There are several limitations to this study. Although informed by implementation science and participant feedback from prior studies, our focus group guides were not piloted in advance, which may have impacted their scope and relevance. We also kept discussion questions/probes broad without guidance from implementation determinant frameworks. This study was also conducted among participants who engaged in the program offered in research-supported trials and did not engage families who declined to participate in these trials. In the future, insights from participants who participate in the program outside of research and those who decline to participate will be highly beneficial. Our purposive sampling aimed to achieve diversity but was biased in limiting prior program participants. Findings may not reflect the opinions of caregivers involved in other early community mental health initiatives or parents who were missed or declined earlier recruitment efforts. Although positive parenting programs have established efficacy among racialized families (McCabe et al., 2020; Yeh et al., 2022), we acknowledge the impact of longstanding systemic and structural racism in Canada's child welfare system and the disproportionate scrutiny and bias toward parenting practices among Black, Indigenous, and other racialized families (Antwi-Boasiako et al., 2020, 2022; Trocmé et al., 2004).
Notably, the prompts from the CFIR intersectionality supplement were not used to inform the focus group guide because they were published after these data had been collected. However, the prompts were highly beneficial in organizing and considering intersecting factors from participant-driven datasets and pointing to gaps for future work. Moreover, an unscripted approach to focus group facilitation empowered participants to lead conversations and flexibly engage in iterative thematic coding, an essential component of intersectionality work. In the future, prompts could address broader consideration of multiple intersecting identities (i.e., the intersection between disability, race, culture, language, and community) and their relationship to the program's implementation. It will be of value to consider the impact of determinant factors for future program implementation. In particular, considering the large tertiary care pediatric hospitals, organizational leadership, and broader political systems. Finally, examining intersectionality within our team and potential societal biases specific to pediatric mental health and parenting may provide insight into potential influences on future implementation.
Moving forward, the results of the current study are of high value in informing the next steps in implementing the I-InTERACT-North program into clinical care and program scalability beyond its research roots. Our results converge with many common barriers and facilitators to larger-scale parenting programs in the community (Sanders et al., 2000; Webster-Stratton & Reid, 2011). However, results highlight the high acceptability of integrating family-focused interventions like I-InTERACT-North within hospital systems. Such programs can uniquely address intersectional factors such as medical complexity and neurodiversity within specialized populations in a way that community practice does not (Williams et al., 2018; Vyas et al., 2021). Common barriers echoed across child and adult neuropsychological populations (Prigatano, 2013; Stucky et al., 2023; Wong, 2023) highlight priorities needed to expand and innovate training and service expectations for providers within hospitals beyond assessment or evaluation. This may be achieved through increased opportunities for early training, supervised practice, and collaborative practice groups that consider the transdiagnostic relevance of providing early positive parenting support to all medically vulnerable populations. Building from examples in adult neurorehabilitation, the creation of habilitation-focused hubs that combine neuropsychological/developmental assessment and innovative interventions like I-InTERACT-North may be pivotal to address the gaps in intervention implementation outside of research environments (Wong, 2023; Wong et al., 2023). Responding to the recommendations from parents and clinical partners alike, we will continue to embed active patient engagement and ongoing co-design and training opportunities throughout the implementation process and beyond to ensure the program's relevance, sensitivity, and sustainability.
Supplemental Material
sj-pdf-1-irp-10.1177_26334895251346816 - Supplemental material for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North)
Supplemental material, sj-pdf-1-irp-10.1177_26334895251346816 for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North) by Tricia S Williams, Angela Deotto, Andrea Greenblatt, Giulia F Fabiano, Rivka Green, Janaksha Linga-Easwaran, Evdokia Anagnostou, Jennifer Crosbie, Elizabeth Kelley, Steven P Miller, Rob Nicolson, Jennifer Rosart, Shari L Wade and Melanie Barwick in Implementation Research and Practice
Supplemental Material
sj-docx-2-irp-10.1177_26334895251346816 - Supplemental material for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North)
Supplemental material, sj-docx-2-irp-10.1177_26334895251346816 for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North) by Tricia S Williams, Angela Deotto, Andrea Greenblatt, Giulia F Fabiano, Rivka Green, Janaksha Linga-Easwaran, Evdokia Anagnostou, Jennifer Crosbie, Elizabeth Kelley, Steven P Miller, Rob Nicolson, Jennifer Rosart, Shari L Wade and Melanie Barwick in Implementation Research and Practice
Supplemental Material
sj-docx-3-irp-10.1177_26334895251346816 - Supplemental material for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North)
Supplemental material, sj-docx-3-irp-10.1177_26334895251346816 for Scaling up: Facilitators, barriers, and EDI considerations for clinical implementation of a stepped-care early mental health parenting program (I-InTERACT-North) by Tricia S Williams, Angela Deotto, Andrea Greenblatt, Giulia F Fabiano, Rivka Green, Janaksha Linga-Easwaran, Evdokia Anagnostou, Jennifer Crosbie, Elizabeth Kelley, Steven P Miller, Rob Nicolson, Jennifer Rosart, Shari L Wade and Melanie Barwick in Implementation Research and Practice
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by a Canadian Institutes of Health Research (CIHR) Operating Grant (FRN: 178854) and a combined COVID-19 Grant from the Garry Hurvitz-Centre for Brain and Mental Health and Edwin S.H. Leong Centre for Healthy Children.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.