
Abstract
Background
There is a substantial mental health treatment gap globally. Increasingly, mental health treatments with evidence of effectiveness in western countries have been adapted and tested in culturally and contextually distinct countries. Findings from these studies have been promising, but to better understand treatment outcome results and consider broader scale up, treatment acceptability needs to be assessed and better understood. This mixed methods study aimed to examine child and guardian acceptability of trauma-focused cognitive behavioral therapy (TF-CBT) in two regions in Tanzania and Kenya and to better understand how TF-CBT was perceived as helpful for children and guardians.
Methods
Participants were 315 children (7–13), who experienced the death of one or both parents and 315 guardians, both of whom participated in TF-CBT as part of a randomized controlled trial conducted in Tanzania and Kenya. The study used mixed methods, with quantitative evaluation from guardian perspective (N=315) using the Treatment Acceptability Questionnaire (TAQ) and the Client Satisfaction Questionnaire-8 (CSQ-8). Acceptability was assessed qualitatively from both guardian and child perspectives. Qualitative evaluation involved analysis using stratified selection to identify 160 child and 160 guardian interviews, to allow exploration of potential differences in acceptability by country, setting (urban/rural), and youth age (younger/older).
Results
Guardians reported high acceptability on the TAQ and, using an interpretation guide from U.S.-based work, medium acceptability on the CSQ-8. Guardians and children noted high acceptability in the qualitative analysis, noting benefits that correspond to TF-CBT’s therapeutic goals. Analyses exploring differences in acceptability yielded few differences by setting or child age but suggested some potential differences by country.
Conclusion
Quantitative and qualitative data converged to suggest high acceptability of TF-CBT from guardian and child perspectives in Tanzania and Kenya. Findings add to accumulating evidence of high TF-CBT acceptability from Zambia and other countries (United States, Norway, Australia).
Keywords
Background
Acceptability, or “the perception among implementation stakeholders that a given treatment, service, practice, or innovation is agreeable, palatable, or satisfactory” (Proctor et al., 2011, p. 67), is an important component in intervention design, evaluation, and implementation (Sekhon et al., 2017). Given the substantial unmet mental health treatment need in many low-resource settings globally with healthcare system gaps and human resource limitations, research has focused on adapting (Kaysen et al., 2013; Verdeli et al., 2003) and testing evidence-based treatments (EBTs) with delivery by lay providers (Bolton et al., 2014; Guest et al., 2006; Murray et al., 2015; Rahman et al., 2008). As most EBTs were developed in western, high-income countries, the cultural and resource contexts in which EBT implementation occurs vary considerably. While evidence from randomized controlled trials (RCTs) in diverse countries and regions suggest that EBTs hold promise for improving mental health outcomes, carefully evaluating acceptability is essential. Without understanding acceptability, we risk implementing interventions that may not be culturally relevant or contextually appropriate. We may also miss opportunities to understand aspects of EBTs that treatment recipients find more or less helpful.
In global mental health studies, perceived acceptability of received treatments often has not been directly assessed, rather, consumer (i.e., those who receive treatment, such as clients and guardians) participation rates have been used as a proxy measure (Brooke-Sumner et al., 2015). Research examining acceptability is particularly limited for child-focused treatments. Among notable exceptions, Jordans et al. (2011) found high satisfaction (n = 29,292) in a multi-layered psychosocial care package in areas of armed conflict, using two quantitative items. Murray et al. (2014) examined consumer and provider acceptability for trauma-focused cognitive behavioral therapy (TF-CBT; Cohen et al., 2006). The authors used qualitative methods and specifically asked about aspects within the treatment. Children (n=18) and caregivers (n=16) reported the program was helpful and discussed specific changes in behaviors or feelings attributed to TF-CBT. While most participants stated that they did not dislike anything about TF-CBT, a few reported critiques including lack of transportation, time required, need for capacity building, and greater service availability. Identifying recommendations via acceptability feedback in this way can inform future implementation with the potential to increase reach, impact, and/or sustainability.
The current study assesses child and guardian perspectives on the acceptability of TF-CBT, using a sample of Kenyan and Tanzanian participants from a large RCT of TF-CBT (Dorsey et al., 2020). Broadly, we were interested in acceptability after treatment receipt. Building on Murray et al. (2014), we were interested not only in acceptability of TF-CBT overall, but also in specific treatment aspects that were most helpful or appreciated, dislikes and challenges encountered (less acceptable aspects), and what recommendations consumers might have for future TF-CBT delivery (ways to improve acceptability). We explored if TF-CBT acceptability might differ based on three differences. First, given differences in treatment outcome between Kenyan and Tanzanian participants at the one-year follow-up in the RCT (Dorsey et al., 2020), we examined perspectives by country. Second, as few studies have assessed acceptability of TF-CBT by age, we explored differences between younger and older children. Third, given potential differences in acceptability in urban and rural areas, we assessed perspectives by setting.
Methods
Data come from a National Institute of Mental Health-funded RCT testing the effectiveness of culturally-adapted TF-CBT for youth who experienced the death of one or both parents, in Tanzania and Kenya (Dorsey et al., 2020). The RCT included 640 youth. Participants were randomized to receive TF-CBT or usual care (UC), resulting in 320 youth and one of their guardians enrolled in TF-CBT. UC mostly included services that could affect mental health (predominantly educational support; 140/320 youth in UC) and some mental health care (29/320 youth in UC; 28 were Kenyan). Participants were stratified by country (Tanzania vs. Kenya), setting (urban/rural), and age (ages 7–10; 11–13). The RCT built on a feasibility pilot of TF-CBT in Tanzania (O’Donnell et al., 2014) and research investigating mental health needs of youth who experienced parental death (Dorsey et al., 2015). It represents standing collaborations between UW, Ace Africa Kenya, and the Tanzania Women Research Foundation (TAWREF). We used the SQUIRE checklist for reporting.
Intervention: Trauma-focused Cognitive Behavioral Therapy
TF-CBT (Cohen et al., 2006) is an EBT with empirical support in the United States and growing evidence in African nations (McMullen et al., 2013; Murray et al., 2015). We utilized a culturally-modified version of TF-CBT, Pamoja Tunaweza (Dorsey et al., 2020). Modifications were made based on focus groups before the pilot, with Tanzanian counselors contributing to additional modifications following the pilot (Dorsey et al., 2020). To encourage tailoring to context and group members, we conceptualized TF-CBT fidelity using plain language of “following the recipe,” meaning delivering all elements. We used plain language of “spicing it up” to encourage adaptation that fits with your community (e.g., using known stories, acknowledging cultural norms and exceptions) and group members (see Dorsey et al., 2020).
The program included 12 group and 3–4 individual sessions over 12 weeks (O’Donnell et al., 2014). Child and guardian groups ran concurrently, with shared activities in final sessions. Initial sessions focused on psychoeducation and coping skills, with guardians learning behavior management skills. In between group sessions 4–7, children and guardians participated in individual sessions for imaginal exposure, called the “trauma narrative” (TN) in TF-CBT. Group sessions 5–8 involved developing plans for situational exposure (i.e., trauma reminders), more individual TN work, and processing common trauma-related cognitions. Guardians received counselor and peer support in preparing to emotionally support children around the TN. Group sessions 9–12 delivered grief-specific elements (e.g., resolving ambivalent feelings; redefining the relationship).
Participation in TF-CBT was associated with larger reductions in posttraumatic stress than UC in 3 of 4 study sites (rural and urban Kenya, urban Tanzania) at treatment end. At 12 months follow-up, TF-CBT was more effective than UC in urban and rural Kenya, where adversity and stress were high (Dorsey et al., 2020). In the Tanzanian sites, by 12 months, the UC condition improved at a similar rate to TF-CBT.
We utilized the Apprenticeship Model (Murray et al., 2011) to build local training capacity, following WHO recommendations for task-shifting. Experienced Tanzanian TF-CBT lay counselors served as trainers. The first author (Dorsey) is an experienced TF-CBT trainer with extensive lay counselor training experience. She provided pre-training supports including a 5-day, practice-based Train-the-Trainer training 1 month before the counselor training, with continued planning support. The Tanzanian trainers trained 12 lay counselors (6 Tanzanian, 6 Kenyan) in an in-person, 10-day training that included experiential activities and small-group practice. The first author was present at the training, meeting with trainers before/after each training day and available to assist. Following training, lay counselors practiced delivery and provided TF-CBT under tiered supervision, involving weekly in-person or virtual meetings with Tanzanian trainers who gave feedback on practice, reviewed counselors’ verbal and written reports of sessions, and supported preparation for upcoming sessions. The first author reviewed written reports and supported Tanzanian trainers in addressing any challenges through weekly calls.
Participants
Participants were 315 children and one of their guardians who received TF-CBT in the RCT and participated in the 12-months post-treatment follow-up (Dorsey et al., 2020). RCT inclusion criteria were the death of one/both parents, aged 7–13, scoring above a locally-defined cutoff for PTS by child or guardian report or maladaptive grief by child-report, residing in a family home, child/guardian willingness to participate, and Kiswahili-speaking. Children were excluded when: parent/s died when child was
Demographic and baseline characteristics of participants included in qualitative coding.
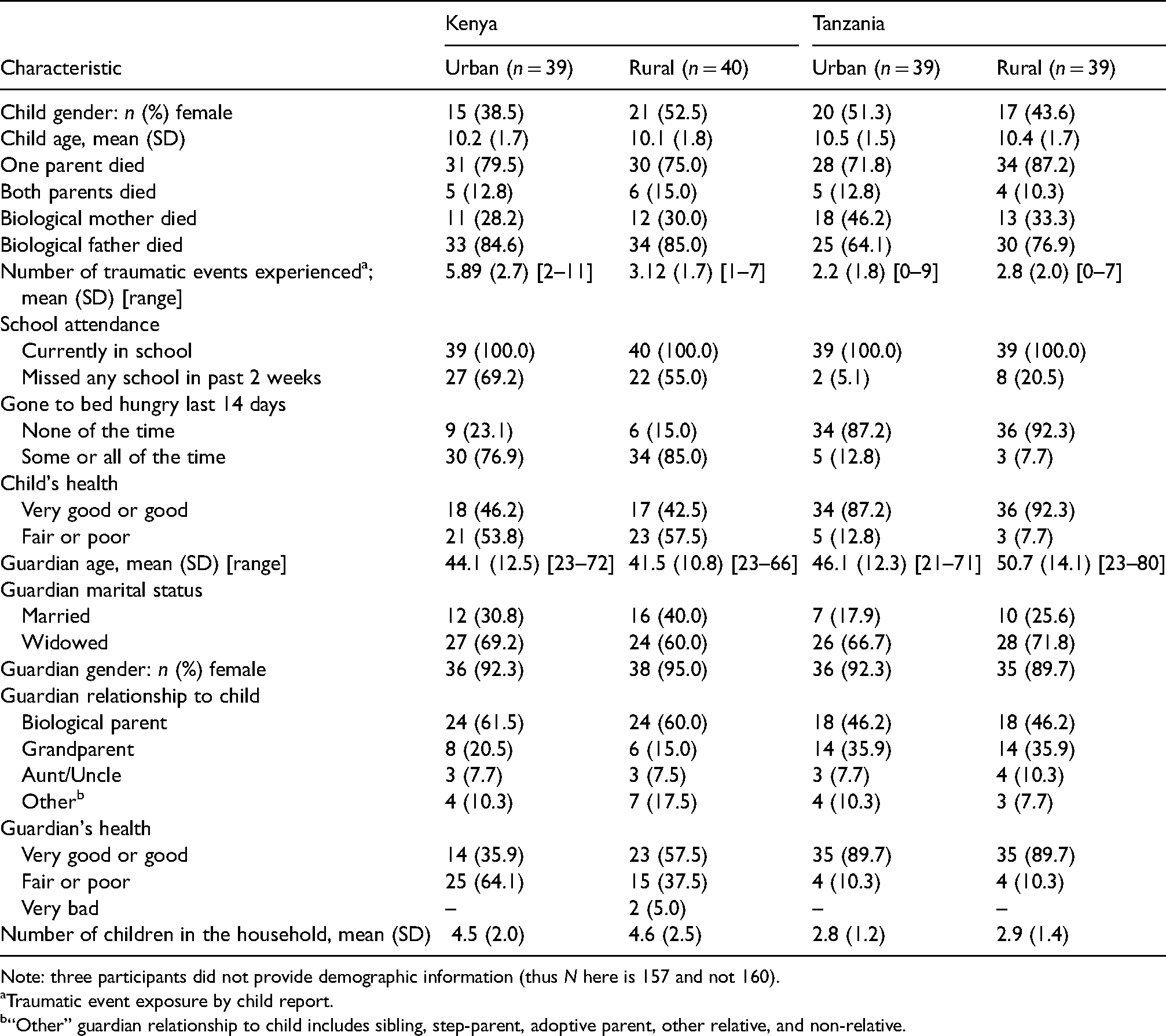
Note: three participants did not provide demographic information (thus N here is 157 and not 160).
Traumatic event exposure by child report.
“Other” guardian relationship to child includes sibling, step-parent, adoptive parent, other relative, and non-relative.
Procedure
All study procedures were approved by the Institutional Review Boards of Duke University, National Institute for Medical Research in Tanzania, and the Kenya Medical Research Institute. Recruitment occurred in five cohorts in each country April 2013–July 2015. Cohorts focused either on an urban or rural area and on younger (7–10) or older (11–13) children. Potential participants were identified by local community members, orphan-serving organizations, and school personnel. The identifying individual made first contact with guardians.
Interviewers had child-interviewing experience and 1-week of study-specific training (e.g., ethical conduct of research, question-by-question practice with feedback, establishing rapport, strategies to reduce social desirability bias—specifying that participant responses have no impact on seeking/receipt of additional services) (Bergen & Labonté, 2020). Interviewers met separately with each child and guardian to obtain informed consent or assent and to administer screening questions, and if eligible, additional questionnaires. Interviewers were masked at baseline and the first follow-up (4 months post-baseline/end of treatment). Treatment acceptability was assessed only at the final, 12 months post-treatment assessment point (16 months post-baseline), as it would unmask interviewers. All guardians randomized to TF-CBT were asked the standard quantitative interview battery from the first follow-up, with added quantitative questions assessing TF-CBT acceptability. A short set of open-ended questions were added at the end for both children and guardians, to allow a qualitative component to our mostly quantitative approach (hereafter referred to as qualitative questions). Interviews were conducted in-person, using paper and pencil. For the qualitative questions, interviewers wrote participants’ answers verbatim in Kiswahili, transcribing answers into English after the interviews. Translated English responses were entered into a database, reviewed, and coded.
Data collection
We were unable to locate existing quantitative measures of treatment acceptability and satisfaction already used in the two countries or in the region (East Africa). We selected quantitative measures with the best face validity. The qualitative questions came from a Zambian TF-CBT study (Murray et al., 2014). For all measures, Kenyan and Tanzanian team members reviewed items for cultural appropriateness. Independent team members translated measures to Kiswahili and back-translated measures to English.
Treatment Acceptability
All guardians reported perceptions of acceptability with the Treatment Acceptability Questionnaire (TAQ; Krain et al., 2005). The eight-item TAQ was modified to include the name of the treatment or referenced “the program.” (e.g., “Pamoja Tunaweza was an acceptable program for my child's feelings and/or behavior”). Respondents rated agreement on a 6-point Likert-type scale, ranging from 0 (Very Unacceptable) to 5 (Very Acceptable). The TAQ has acceptable psychometric properties in U.S.-based samples (α = 0.93; Krain et al., 2005) and acceptable internal consistency in our study (α Kenya = 0.75; α Tanzania = 0.80).
Treatment Satisfaction
Guardians reported treatment satisfaction on a revised version of the Client Satisfaction Questionnaire (CSQ-8; Larsen et al., 1979). The CSQ-8 items were modified to include “and your child/'s” (e.g., “To what extent has our program met you ‘and your child's’ needs?”). In their U.S.-based work, developers noted that scores between 8–20, 21–26, and 27–32 can be interpreted as low, medium, and high satisfaction, respectively (Larsen et al., 1979). We are not aware of non-U.S. studies validating this interpretation. The CSQ-8 has acceptable psychometric properties in U.S. samples (α: 0.83–0.93) (Attkisson & Zwick, 1982). Internal consistency for the CSQ-8 was acceptable in our study (α Kenya = 0.82; α Tanzania = 0.74).
Qualitative assessment
Guardians answered six open-ended questions assessing experiences with Pamoja Tunaweza (Murray et al., 2014). These asked about experiences generally, challenges, TF-CBT likes and dislikes, any changes the family/child/self because of the program, and recommendations. Children were asked only three open-ended questions, assessing likes, dislikes, and (uniquely) if the child would recommend this program to another child who had a parent die (and why/why not).
Analysis
We used a mixed methods design with a QUAN + QUAL structural arrangement, in which the mixed methods function was convergence, with equal weight given to quantitative and qualitative data (Palinkas et al., 2011).
Quantitative Data
We present descriptive statistics to understand guardian perceptions of treatment acceptability on quantitative measures, calculating mean (M) and standard deviation (SD). For both measures, higher scores represent more favorable responses. To explore differences in acceptability, we ran two-sample independent t-tests to compare mean scores (i.e., Kenya vs. Tanzania, urban vs. rural). We present Cohen's d effect sizes for any significant mean differences.
Qualitative Data
As there is no clear consensus on sample size to ensure saturation (Fusch & Ness, 2015), we chose to code qualitative questions for half the participants (n = 160/315 guardian and n = 160/315 child). Interviews were randomly selected after stratifying by country (Kenya/Tanzania), setting (urban/rural), and age (young/old). Two authors (Lucid and Benjamin) began analysis with an initial reading of all qualitative responses, taking notes about the data and meeting before coding to discuss questions and issues (Sandelowski, 1995). Coders were American UW team members; Tanzanian and Kenyan team members were consulted throughout and advised coders to support accurate interpretation of participants’ statements and wording (e.g., providing perspective, returning to the original Kiswahili). Code generation followed a Grounded Theory approach (Charmaz & Belgrave, 2015) and began with coding the same 12 interviews line-by-line. Interviews were randomly selected from each grouping (e.g., child/guardian, young/old, Kenya/Tanzania, rural/urban) and coded using Dedoose v8.1.8. After initial line-by-line coding, the two coders compared and refined codes creating a preliminary codebook. Coding categories naturally grew around the three broad response categories of: (1) positive and (2) negative experiences with TF-CBT, and (3) recommendations.
After coding the initial 12 interviews, the two authors coded 36 additional interviews, taking an iterative step-wise approach to codebook building. To assess if new information was emerging in the data (Guest et al., 2006), we utilized a saturation grid (Brod et al., 2009) in which themes were listed horizontally and new interviews vertically. Authors applied focused coding in addition to line-by-line coding to capture broader emerging themes (Charmaz & Belgrave, 2015). The process entailed taking codes applied frequently during line-by-line coding and elevating them to coding categories applied to larger swaths of data (Charmaz, 2001). We determined saturation had been reached when there were no longer new themes raised during the iterative coding. The authors then met to review code development and settle on a final set of codes based on thematic recurrence.
Inter-coder reliability was examined prior to coding the rest of the data. Initial inter-rater reliability exceeded guidelines for satisfactory reliability (kappa
Results
Guardian Results
Quantitative Results
There was very limited missing data. Results from the quantitative measures are in Table 2. Across our sample, guardians reported high rates of treatment acceptability on quantitative measures. Overall, acceptability was 4.71 (SD = 0.32) on the TAQ (4.71 out of 5, which corresponds to “very acceptable”). Acceptability was 21.73 (SD = 2.23) on the CSQ-8, with U.S.-based guidelines suggesting interpretation as medium acceptability. There was some small, though statistically significant, variability in acceptability across participant groups. Kenyan guardians reported greater treatment acceptability (TAQ M = 4.82, SD = 0.30; CSQ-8 M = 22.44, SD = 2.14) than Tanzanian guardians (TAQ: M = 4.64, SD = 0.32; p < .001; CSQ-8: M = 21.28, SD = 2.18; p < .001). Effect sizes indicated medium effects, using Cohen’s (1988) metrics (TAQ: d = 0.57; CSQ-8: d = 0.54). Treatment acceptability on the TAQ was similar between guardians from urban and rural areas (p > .05); however, acceptability on the CSQ-8 was greater among urban guardians (M = 21.88; SD = 2.22) than rural guardians (M = 21.24, SD = 2.21; p < .05; d = 0.29; small effect per Cohen’s (1988) metrics). Acceptability did not differ between guardians of older or younger children for either measure (both p > .05).
Guardian responses on quantitative measures of acceptability (N = 315).
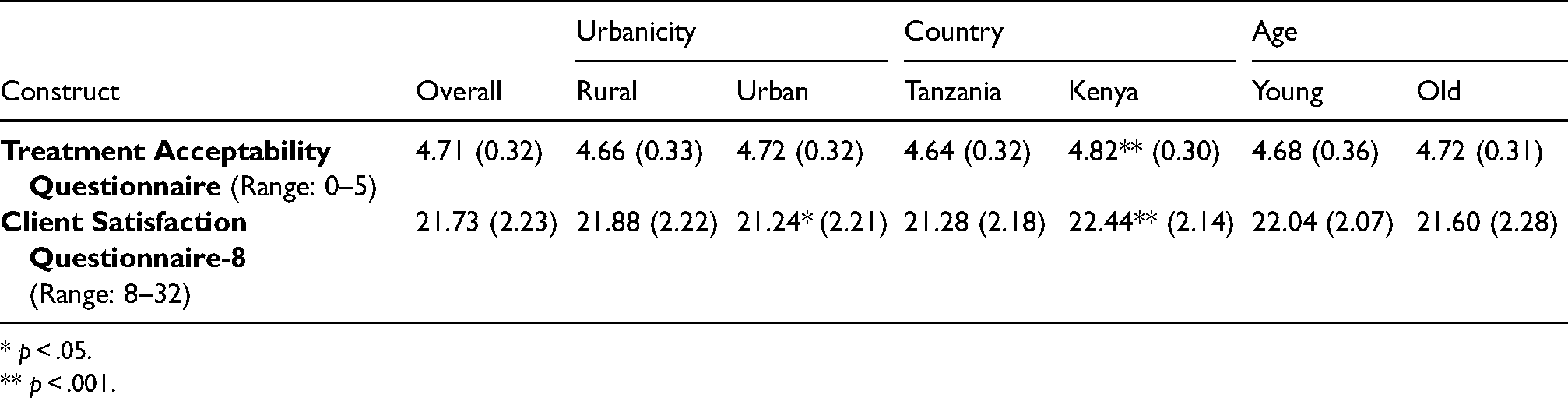
* p < .05.
** p < .001.
Qualitative Results
In response to questions assessing experiences with Pamoja Tunaweza, all 160 guardians noted something positive about TF-CBT. Table 3 includes all coded responses endorsed by three or more guardians.
Coded themes from guardian interviews one year after TF-CBT participation.

TZ: Tanzania; KE: Kenya.
The child had a lot of fear on seeing things that reminds him about his father like, table, chair and the mat his father used while praying, clothes and photos but after the teachings he has changed and he even can use the table, chair and praying mat without any difficulty.
Kenyan guardians more frequently mentioned decreased child avoidance and improved socialization skills/interaction.
It is a program that helps on how to reduce anxiety and bad thoughts and also it educates us on how to live well with orphaned children who feel like their life is not important but through these teachings we learn on how to restore hope and make them feel important and worthy to live.
Before the teachings I was so harsh on children but I have been taught on how to be patient and polite on them and my relationship with my children nowadays has improved so much and I like the way we are living in peace and love.
Second, they mentioned appreciating learning how to cope with the parent/s’ death (71/160, 44%) for themselves and/or their child (including being able to talk more openly). Rural-dwelling guardians mentioned this benefit more often. Liking the refreshments was the third most frequently mentioned, particularly by Tanzanian guardians. Cognitive coping (learning to think in a different way to feel better) was the fourth most mentioned, with Kenyan guardians noting cognitive coping more frequently.
The fifth most frequently mentioned aspects liked by guardians were the relaxation exercises. Kenyan guardians, and guardians who were rural-dwelling, mentioned liking this aspect of the program more frequently. Guardians from both countries and areas also noted that they appreciated other aspects of the program (see Table 3).
Child results
Acceptability
In response to questions assessing their experiences with Pamoja Tunaweza, all children (160/160, 100%) noted something positive. Table 4 presents all coded responses stated by three or more children.
Coded themes from child interviews one year after TF-CBT participation.
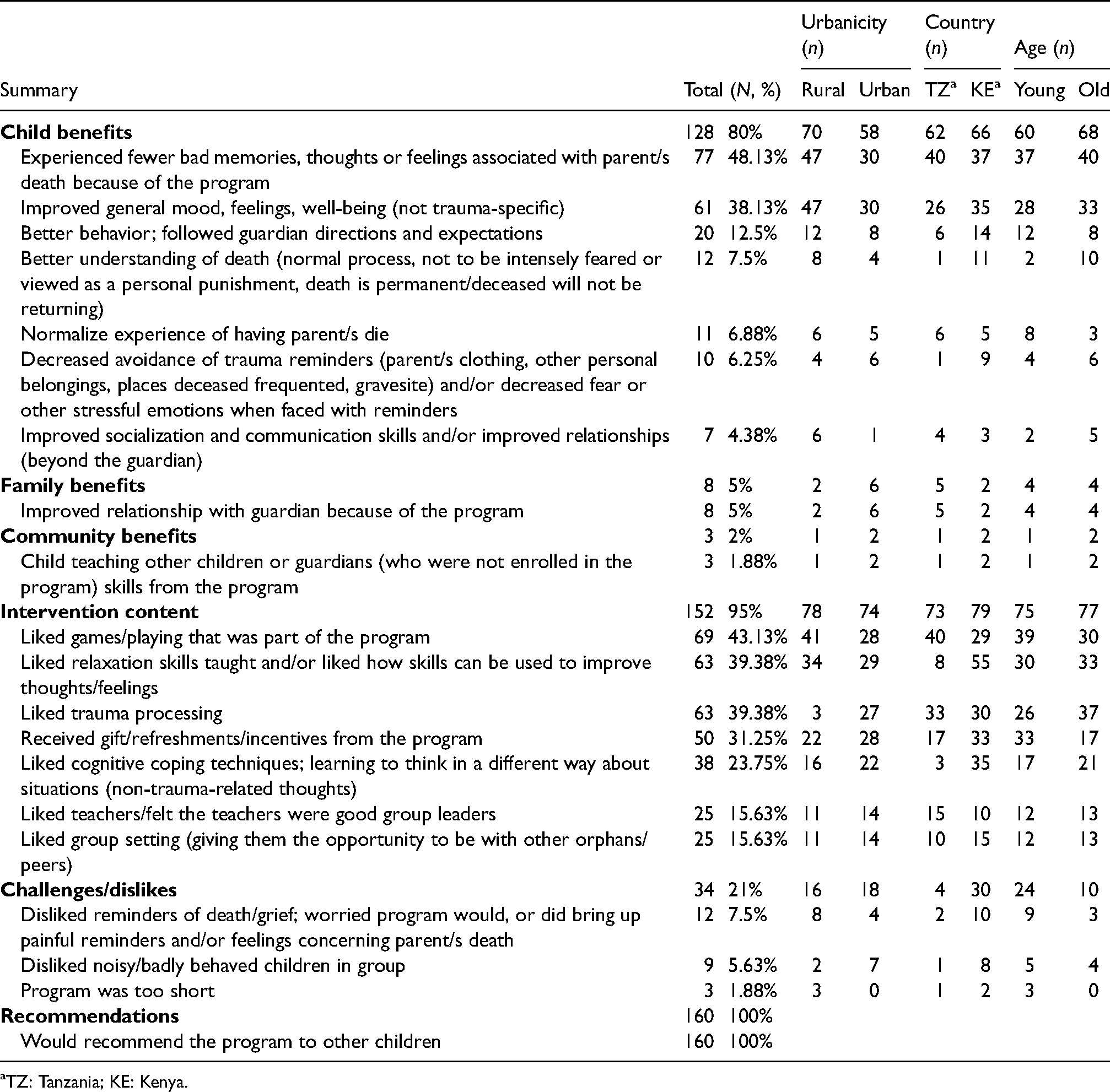
TZ: Tanzania; KE: Kenya.
Improved Child Outcomes
Children frequently cited improvements in their own lives (128/160, 80%). There appeared to be no differences by country, area, or child age in the frequency; however, there were differences in the specific benefits mentioned. Children most frequently mentioned experiencing fewer bad memories, thoughts, and/or feelings associated with their grief as well as general improvements in mood or feelings (not trauma-specific). They taught me how to stay without bad memories of the mother. Also they taught us not to envy, or feel jealousy for those who have both parents alive. Songs, riddles, relaxations. They also taught us to respect people and not to abuse them.
Children from rural areas were more likely to describe experiencing fewer bad memories. The next most frequently mentioned outcomes were improvements in children's own behavior, increased understanding that their parent/s’ death was not something to be feared or a personal punishment, normalization of their experience, and decreased avoidance of trauma triggers.
Family and Community Benefits
A small number of children noted improvements in their relationship with their guardian (8/160, 5%) and community-level benefits (3/120, 2%). There appeared to be no differences by country, area, or child age for family or community benefits.
Intervention Content
Children frequently mentioned intervention content that they liked (152/160, 95%). There appeared to be no differences by country, area, or child age; however, there were differences in the specific content mentioned. The most commonly mentioned aspect was games and play as part of the intervention, with more frequent mention by children from rural areas. The second most commonly mentioned intervention aspect was learning relaxation skills, with Kenyan children mentioning relaxation more frequently. The third and fourth most commonly mentioned aspects of the intervention were learning how to process trauma-related thoughts and receiving incentives (i.e., refreshments, small gifts). “I liked being with fellow children and discussing about how to cope with difficult memories of death of parents.” Receiving incentives was more often mentioned by Kenyan youth and by younger children. Other content is listed in Table 4, including cognitive coping (fifth most commonly mentioned), which Kenyan children more frequently mentioned.
Challenges/Dislikes
Only 34 of 160 children (21%) reported challenges or dislikes, with Kenyan youth and younger youth reporting dislikes more often. There were no apparent differences by setting. Of those who reported dislikes, the most commonly coded dislike was the program bringing up reminders and feelings about the parent/s’ death. “I didn't like mentioning my father who died all the time or talking about him. Also I didn't like remembering his image, the way we used to stay with him, [it] made me feel sad.”
Recommendations for the Future
All child participants (160/160, 100%) said they would recommend the program. Children described the value for normalizing experiences and providing skills to cope: I would recommend because it is good to be together with people of similar situations of losing a parent and finding solutions to reducing thought of the parent's death. These teachings are very valuable lessons for those who are orphaned and they think it's the end of the world.
Discussion
In this mixed methods study, quantitative and qualitative results from Kenyan and Tanzanian guardians and children converge to suggest high acceptability of TF-CBT. To our knowledge, this also is the largest study examining TF-CBT acceptability. Guardians and youth spoke positively about the intervention and noted specific child benefits that correspond to therapeutic goals of TF-CBT. These benefits included improved mood and feelings as well as decreased distress and behavioral impact related to the parent/s’ death (e.g., avoidance, social isolation). Most guardians also noted broader benefits, for their families and sometimes themselves. Both child and guardian participants recalled specific intervention content that they appreciated. Guardians most frequently recalled appreciating the parenting skills and improved ability to cope with death, both for themselves and for their children. Children most frequently recalled appreciating games and play, relaxation skills, and processing trauma-related thoughts. All child participants reported that they would recommend the program to other children. Our study is unique in that there are very few studies of child and adolescent treatments that include large samples and use mixed methods.
Our findings of high acceptability of TF-CBT overlap with those from other studies examining consumer perspectives, including the Murray et al. (2014) study in Zambia where children and caregivers attributed positive changes for the family and child to TF-CBT, noting better family communication, fewer problem behaviors, and greater ability to talk about traumatic events. Specific TF-CBT elements noted in our study also overlap with themes from other qualitative studies in mostly western countries examining TF-CBT consumer perspectives, including the therapeutic benefit of talking about traumatic events (Eastwood et al., 2020) and learning skills for reducing stress (Lange et al., 2020). In qualitative studies in Norway (Dittmann & Jensen, 2014) and Australia (Eastwood et al., 2020), youth who received TF-CBT noted that although talking about traumatic events could be difficult, it was one of the most helpful and transformative aspects of treatment. In these studies, youth consumers shared that talking about traumatic events was less distressing and more comfortable when therapists were perceived as empathetic, knowledgeable, and authentic. Findings from our study add to accumulating evidence from smaller qualitative studies in Zambia (Murray et al., 2014), Norway (Dittmann & Jensen, 2014), Australia (Eastwood et al., 2020), and the United States (Okamura et al., 2020) that facing up to traumatic events can have therapeutic benefits.
However, even in our sample where TF-CBT therapeutic benefits were acknowledged, talking about the parent/s’ death was the most commonly reported dislike by children (7.5% of youth) and the second most commonly reported dislike by guardians (8.13%). In many cultural groups, speaking about individuals who have died is discouraged and sometimes unacceptable, particularly if what is said might be negative. Yet, at the same time, children impacted by parent/s’ death often need support around specific aspects related to the death itself or surrounding context (e.g., negative interaction, not able to attend the funeral), that are challenging to provide without understanding the child's experience. Thus, we conducted early focus groups and a small pilot to understand child, guardian, and counselor perspectives (O'Donnell et al., 2014). We cannot determine whether the percentage of children and guardians who disliked this aspect is greater than would be encountered in a different cultural context. However, child and guardian statements seemed to reflect what we commonly see with TF-CBT, that talking about traumatic events can bring up emotions like sadness or fear. In our study, participant statements about disliking this aspect did not seem to mention that talking about the parent/s who died was unacceptable or inappropriate.
In our study, there was little data to support meaningful differences in acceptability by area (urban or rural) or child age. There are often concerns about acceptability of treatments in rural areas (vs. more urban locations). Research from rural areas in the U.S. has highlighted concerns related to cultural acceptability of treatments and their alignment with rural community norms (Bryant et al., 2013), as well as challenges with maintaining privacy and confidentiality in smaller rural communities (Bryant et al., 2013; Murry et al., 2011). Urban guardians did report higher acceptability on one quantitative measure; however, scores for both groups were in the “medium” range (from U.S. studies) and similar, suggesting that while scores were statistically different, there might not be meaningful differences. The only difference noted in our qualitative analysis was in intervention content, and in a direction that supports greater acceptability in rural areas (e.g., rural guardians mentioning liking trauma-specific elements more). We also did not see differences by child age, which provides some consumer-perspective support for clinical outcomes from TF-CBT efficacy and effectiveness trials (including ours; Dorsey et al., 2020), where age has not moderated treatment outcomes (Kane et al., 2016).
There did, however, appear to be some differences in acceptability between countries. These differences were seen across the quantitative and qualitative analyses. Quantitatively, Kenyan guardians reported statistically greater acceptability on both measures than did Tanzanian guardians (although scores may not be meaningfully different). Qualitatively, there were also differences in the types of benefits discussed by guardians. Interestingly, given differences in treatment results from the RCT where the TF-CBT condition outperformed UC in Kenya but not in Tanzania (Dorsey et al., 2020), Tanzanian guardians more frequently mentioned community-level benefits (e.g., sharing knowledge with community). We cannot definitively explain why the UC group in Tanzania improved similarly to the TF-CBT group. However, these findings of guardians reporting sharing in the community—along with other, separate qualitative coding conducted to understand the RCT results—suggest country-differences in sharing with community-members who did not receive TF-CBT. These qualitative coding efforts involved having a coder masked to RCT results and country code counselor-completed TF-CBT session reports for any mentions of sharing. Analyses indicated that Tanzanian counselors were twice as likely as Kenyan counselors to encourage children to share intervention content with other children. Additionally, Tanzanian counselors were also 25% more likely to note that children shared intervention content with other children in their community. Collectively, these findings demonstrate how consumers and counselors might differentially see some treatment benefits (e.g., chance to have one's community benefit from an intervention delivered to only a few).
In terms of recommendations for the TF-CBT program, guardians’ primary recommendation was ensuring the program continued after study completion. Guardians also recommended including support for non-mental health needs (e.g., food, school fees). In a prior study by our team (Woods-Jaeger et al., 2017), counselors delivering TF-CBT described their own stress and compassion when encountering families’ unmet needs and their own desire for more support for families. In our collaborative TF-CBT research, communities develop a “standard-of-care” protocol, compiling formal (e.g., health centers) and informal resources (village leaders). This protocol includes options counselors and interviewers can use when needs and concerns arise. However, our findings suggest more attention is needed within the intervention itself. There is an increase worldwide in recognition of the detrimental impact of social determinants on mental health, with calls for incorporating awareness of social determinants into mental health care (Shields-Zeeman et al., 2019). In a recent qualitative study of top problems experienced by youth in Nairobi, Kenya, 35% reported an economic problem (Wasil et al., 2021). As a field, we need options for addressing mental health problems that can also attend to social determinants.
These analyses should be viewed within the confines of several limitations. Interviews took place 1 year after intervention. This timing was intended to keep interviewers masked to participants’ study condition. However, given the delay, it is possible that clients’ recollections were impacted with time. We attempted to control for social desirability, but social desirability bias may have impacted participants’ desire to report more positive acceptability. Additionally, Kenyan and Tanzanian team members were consulted during coding, but formal member checking was not conducted with research participants. Finally, to our knowledge, the TAQ and CSQ-8 have not been validated in East Africa. In the absence of formal validation, we cannot be assured of their ability to truly capture acceptability. To partially mitigate these challenges, Tanzanian and Kenyan team members assessed the original English and Kiswahili translations to ensure wording was understandable and meaningful. Scores converged with qualitative analysis, which could inform others’ confidence in their use.
Conclusion
Acceptability was high among Kenyan and Tanzanian guardians and children. Our findings add to accumulating evidence of acceptability from Zambia and other countries including the United States, Norway, and Australia. Study implications include support for scaling up TF-CBT in these communities. Next steps include studying how to further improve acceptability, and specifically how to better address social risk factors within TF-CBT treatment sessions.
Footnotes
Acknowledgements
We wish to thank project staff who were all funded by the NIMH grant. This includes staff from the University of Washington, Duke University, TAWREF, and Ace Africa, specifically Luililiaeli Mfangavo, Simon Joseph, Suzan Kitomari, Leonia Rugalabamu, Cyrilla Amanya, Anna Koons, and Kelly Thompson. We are indebted to all the community partners, counselors, and interviewers in Tanzania and Kenya. Their hard work, dedication, and high integrity made this research possible. We gratefully acknowledge the ongoing support of the Ministries of Health and of Education in both countries. We also acknowledge Judy Cohen, a developer of TF-CBT who was a consultant on this grant, and Laura Murray, a global TF-CBT researcher and expert. Both Drs. Cohen and Murray supported this work. We appreciate Julie Nguyen and Lucy Liu's assistance with proofreading, formatting, and editing of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. Shannon Dorsey has received payment in past years for providing TF-CBT training and consultation. She has grant funding focused on TF-CBT as a MPI and as a Co-I.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a National Institute for Mental Health (NIMH) grant to the first and last authors (R01 MH96633). Haley A. Carroll was supported by a NIMH T32 (T32 MH116140-02) and a NIMH K23 (K23 MH127308-02).