
Abstract
Background
The perinatal period is a high-risk time for body dissatisfaction and disordered eating. Evidence-based interventions for disordered eating have not been adapted to address the needs of this population. We describe the process of adapting the Body Project, an evidence-based eating disorder (ED) prevention program, for pregnant individuals with histories of disordered eating behaviors.
Method
Our approach is informed by ADAPT, a framework offering guidance for adapting interventions to new contexts, to modify the Body Project for pregnant individuals. Following initial adaptations informed by a needs assessment and stakeholder input, we conducted a pilot trial with individuals who have lived experience relative to our target population (i.e., previously pregnant individuals with ED history, n = 10). Participants provided feedback on the intervention through surveys and a focus group assessing perceptions of the intervention and barriers and facilitators to its implementation as guided by the Consolidated Framework for Implementation Research (CFIR).
Results
Eighty percent of enrolled participants attended five or more sessions (out of six). Across sessions, average satisfaction ratings were 9.28 (1 = poor to 10 = excellent). Most participants (89%) reported improvements in body satisfaction. Approximately 33% reported reductions in disordered eating with the remainder reporting no change due to healthy eating behaviors at baseline. Themes from the focus group are reported aligning with CFIR domains and all final modifications are summarized and reported aligning with the Framework for Reporting Adaptation and Modifications-Enhanced.
Conclusions
Applying implementation science frameworks to structure our process for making and summarizing planned adaptations, we adapted an empirically supported ED prevention program for pregnant individuals with histories of an ED. We made adaptation decisions based on participant feedback while weighing intervention fidelity and scalability. We will formally test the adapted intervention in a subsequent pilot randomized controlled trial versus a time- and dose-matched educational control.
Plain Language Summary
Keywords
Introduction
Body dissatisfaction is a common problem and is a major risk factor for eating disorders (EDs; Stice, 2002). Individuals may be more susceptible to body dissatisfaction than usual during the perinatal (i.e., pregnancy and postpartum) period. The normal physical changes brought on pregnancy, such as weight gain, are often at odds with the “appearance ideal” in Western society that is largely defined by thinness, which can increase body dissatisfaction, and in turn, risk for disordered eating (Stice, 2002). Research has found that over 33% of pregnant women have body dissatisfaction (Roomruangwong et al., 2017) and an increased risk of disordered eating symptoms during the perinatal period, even among women without a history of an ED (Easter et al., 2015). For those with histories of an ED, pregnancy and the related body changes can trigger ED relapse. A prospective study of over 120 women in stable remission before pregnancy found that 25% of women experienced ED relapse in pregnancy or the postpartum, highlighting that this is a high-risk population (Sollid et al., 2021). EDs during the perinatal period are associated with a myriad of negative outcomes for birthing persons (e.g., postpartum depression, Micali et al., 2011; antepartum hemorrhage, Mantel et al., 2020) as well as negative consequences for infants (e.g., preterm birth, small for gestational age, microcephaly, Mantel et al., 2020). Furthermore, disordered eating in mothers is correlated both with disordered eating in daughters (Pike & Rodin, 1991) as well as other psychopathology in offspring (Micali et al., 2014).
These risk factors and adverse outcomes point to an opportunity to intervene in pregnancy to reduce the risk of ED relapse among perinatal individuals. Recent research has concluded that there is a need for an intervention that can be implemented from early pregnancy to prevent the emergence or worsening of disordered eating during the perinatal period (Baskin et al., 2021). However, there is a lack of evidence-based interventions to address body image and eating concerns in perinatal individuals. Prior to developing a new intervention, it is important to consider whether existing evidence-based interventions are suitable for adaptation (Moore et al., 2021). There are interventions with established efficacy in improving body image and preventing disordered eating, which have the potential to be tailored for this population. The Body Project, a cognitive dissonance-based program designed to reduce body image concerns and prevent EDs, is among the most widely studied and well supported ED prevention programs (Stice et al., 2019a).
Most of the research on the Body Project has been conducted among high-school and college-aged women, and there is evidence that the Body Project is even more effective when implemented by peer-leaders (Greif et al., 2015; Kilpela et al., 2014; Stice et al., 2020). Task-shifting services to trained peers or nonprofessionals is a promising cost-effective service delivery model (Simoni et al., 2011). Additionally, there is emerging evidence that virtual delivery of the Body Project may be a novel and more effective implementation approach to support scalability and to extend the reach of this ED prevention program among hard-to-reach populations, reducing onset of EDs (Ghaderi et al., 2020; Stice et al., 2023). Our team has published a needs assessment exploring potential interest in, and areas of adaptation of, the Body Project program delivered to perinatal individuals (Vanderkruik et al., 2022)
Here, we describe the process of selecting and adapting the Body Project for pregnant individuals with histories of an ED with the aim of preventing relapse of disordered eating behaviors in the perinatal period. This work is informed by several implementation science frameworks including ADAPT (Moore et al., 2021) to guide the approach to adaptation, and Framework for Reporting Adaptation and Modifications-Enhanced (FRAME; Wiltsey Stirman et al., 2019) to provide organization for presenting resulting adaptations and modifications of the intervention. ADAPT guidance outlines systematic steps for adapting evidence-based interventions (e.g., the Body Project) to new contexts or populations (e.g., pregnant individuals; Moore et al., 2021). Consistent with this guidance, we made initial adaptations to the Body Project using stakeholder input and subsequently conducted a pilot test of the adapted intervention followed by an exit focus group with participants from our target population. Our adaptation process draws on elements of user-centered design in that our approach is grounded in feedback and input from individual's with lived experience who may have benefited from the program during the perinatal period (Courage & Baxter, 2005; Lyon & Koerner, 2016). The adapted intervention will be formally tested in a future pilot randomized controlled trial (RCT) assessing feasibility, implementation outcomes, and potential effectiveness for reducing the risk of increased disordered eating behaviors and body dissatisfaction in pregnancy and the postpartum, versus a time- and dose-matched educational control. This work ultimately aims to fill the identified gap in interventions to address body dissatisfaction and disordered eating in this perinatal population who is at high-risk for relapse.
Method
This article describes the first phase of a two-phase study that aims to adapt and test the Body Project for pregnant individuals with histories of an ED. Phase I is focused on adaptation and Phase II will assess feasibility and implementation outcomes and explore effectiveness of the adapted intervention through a pilot RCT (N = 60). The pre-RCT adaptation process (Phase I, the focus of this report) includes tailoring the Body Project script to fit the perinatal population's needs, in addition to a pilot trial, followed by an exit focus group with participants. Below we outline our application of Steps 1–3 of the ADAPT guidance, which is also summarized in Table 1. The modifications resulting from this process are reported in line with the FRAME framework in the results section below.
Summary of ADAPT Steps and Key Activities.

Note. FRAME = Framework for Reporting Adaptation and Modifications-Enhanced.
ADAPT Step 1: Assess Rationale for Intervention and Consider Intervention-Context Fit of Existing Interventions
As noted, research shows there are high rates of body dissatisfaction (a risk factor for disordered eating) and ED relapse in perinatal individuals (Easter et al., 2015; Roomruangwong et al., 2017). The prevalence of these issues, coupled with the negative consequences for both birthing people and their offspring, indicates the need for an intervention in early pregnancy that aims to prevent body dissatisfaction and disordered eating in the perinatal period. To our knowledge, there are no existing interventions specifically designed for individuals in early pregnancy with proven efficacy in preventing disordered eating during the perinatal period. Our team conducted a needs assessment with pregnant and postpartum (within one year of delivery) individuals to further investigate the relevancy of and suggestions for an intervention to address body image and eating concerns during the perinatal period (Vanderkruik et al., 2022). Over 50% of participants reported being dissatisfied with their bodies and approximately 80% indicated interest in a program related to body acceptance or expectations about body changes in pregnancy and postpartum. Additionally, participants reported a desire for a group-based intervention where they could engage with peers experiencing similar concerns.
The first author of this manuscript (RV; a PhD-level clinical psychologist) reviewed the literature on existing group-based ED prevention programs. The Body Project, an ED prevention program, was considered as a suitable intervention for adaptation to fit this context as it has been identified as the only ED prevention program that warrants the American Psychological Association's designation as an efficacious intervention (Stice et al., 2013). This evidence-based program aligns well with participants’ suggestions in our previously conducted needs assessment (Vanderkruik et al., 2022) as the program focuses on body acceptance, is delivered in a group setting, can be peer-facilitated, and allows participants to interact with peers facing similar challenges.
The feasibility and scalability of The Body Project is also noteworthy; it has been identified as a model program for how to address barriers to scalability and achieve large-scale implementation and sustainability, reaching over 6 million girls and young women in 139 countries (Mantel et al., 2020). In addition, the ability to peer-deliver the program further strengthens the potential for widespread and cost-effective implementation (Stice et al., 2020). The Body Project has also been successfully adapted to other contexts including men with body dissatisfaction (Brown et al., 2017), college-aged men of sexual-orientation minorities (Brown & Keel, 2015), professional ballet dancers (Gorrell et al., 2021), female college athletes (Stewart et al., 2019), and college-aged women from non-western cultures (AlShebali et al., 2021), among others. Given that the Body Project has the strongest evidence supporting its efficacy to prevent EDs, and its demonstrated feasibility of broad dissemination and implementation, no other interventions were considered for adaptation.
The Body Project is typically delivered as four 1-hr weekly sessions consisting of written, verbal, and behavioral exercises. The sessions aim to induce cognitive dissonance by encouraging participants to challenge the thin-ideal, a theoretically and empirically supported component of ED prevention that reduces this key attitudinal risk factor (i.e., pursuit of the thin ideal; Micali et al., 2011; Stice et al., 2019a). Given the structure of the program, overwhelming evidence base, and potential for scalability, this intervention was selected to be adapted for addressing body image and eating concerns in perinatal individuals. Additionally, since the target population for this current study consists of individuals with histories of an ED or disordered eating behaviors, we also incorporated elements from a treatment intervention (i.e., the Body Project Treatment 8.0 manual; Stice et al., 2019b) into the adapted version of the Body Project.
ADAPT Step 2: Plan for and Undertake Adaptation
An adaptation team was created consisting of a PhD-level Clinical Psychologist with expertise in perinatal mental health and experience conducting research on the Body Project, two bachelor-level clinical research coordinators with experience conducting research in perinatal mental health, and three additional stakeholders offering expertise in nutrition in pregnancy (a registered dietician/licensed dietitian nutritionist), EDs and the Body Project prevention and treatment programs (a PhD-level researcher), and implementation research (an MD-level clinician and researcher). The first author led the initial adaptation of the Body Project intervention scripts utilizing findings from the needs assessment (Vanderkruik et al., 2022), input from the adaptation team, and insights from clinical experience with perinatal individuals. Author E.S. (the developer of the Body Project) advised on the content, structure, and delivery of the intervention. Author S.N. (an obstetric perinatal dietitian) informed the study team about commonly reported issues, comments, and feelings that come up regarding eating and body image during the perinatal period. S.N. also reviewed the adapted intervention scripts and helped to incorporate additional materials and resources relevant to pregnancy. The team also consulted the Community Access, Recruitment, and Engagement (CARE) Research Center at Massachusetts General Hospital to assess ways to enhance the diversity and inclusivity of the program. The CARE team provided suggestions around inclusive language in the intervention scripts, recruitment materials, and recruitment strategies. We then trialed the adapted scripts, “The Pregnant Body Project,” in a pilot group as detailed below in Step 3.
ADAPT Step 3: Plan for and Undertake Piloting and Evaluation
We conducted a pilot trial of the adapted intervention scripts among individuals with lived experience relevant to our target population (i.e., individuals who have given birth and have with histories of an ED). As the intervention will be delivered in pregnancy with the aim of preventing increased risk of disordered eating across both pregnancy and the postpartum, we intentionally decided to enroll participants who have experienced both pregnancy and postpartum for this pilot group. Individuals who have experienced both pregnancy and postpartum have a unique input on what would be helpful throughout the entire course of pregnancy and postpartum, whereas individuals who are currently pregnant individuals may not be aware of body image challenges they will face in later trimesters or after delivery. This pilot study was designed to inform additional refinement of the adapted intervention before conducting a subsequent RCT of the further adapted intervention. Eligibility criteria for this pilot study included people who: (a) are ages 18–45 years old; (b) have given birth; (c) are willing and able to participate in the virtual-group sessions; (d) are able to speak and read English, and (e) have a self-report history of an ED that is not current or ongoing. Participants were ineligible if they reported having a diagnosis of bipolar disorder or mania, a psychotic disorder, an active substance use disorder, or had suicidal ideation within the past 2 weeks. Participants self-reported their mental health history and diagnoses. The eligibility criteria were intentionally broad for the adaptation phase (Phase I) of this work, allowing for a wide range of input and perspectives to be captured in participant's feedback.
Participants were recruited using an online platform used to connect the general public to research studies within the Mass General Brigham hospital system, social media, and targeted email outreach to postpartum women who had previously indicated interest in research participation. Interested participants used a link or quick-response code (QR code; a barcode that can be scanned by smartphones to access as weblink) on recruitment materials (e.g., flyers, social media posts, email blasts) to access and complete an online eligibility questionnaire via Research Electronic Data Capture (REDCap; Harris et al., 2019). Clinical research coordinators contacted eligible participants by phone to collect verbal consent and administer questions about demographics and mental health history. The study was approved by the Mass General Hospital Institutional Review Board (2023P000630). As informed by guidance for facilitation of the Body Project groups, we sought to enroll ten participants for the Phase I pilot study (N = 10). The first author R.V. facilitated the sessions and focus group over Zoom.
The pilot study consisted of six weekly 1-hr sessions of The Pregnant Body Project program. After each session, participants were invited to complete a brief session-specific feedback survey and were reminded of the homework exercises to complete between sessions. Participants rated each weekly session on a scale of 1 (poor) to 10 (excellent). The feedback survey following the final session also included several questions of overall program feedback and perceived impact (see Supplementary Material for standard post-session and post-program feedback surveys). Participants reported how the program impacted their body image on a scale of −10 (my body image is now much worse) to 10 (my body image is now much better) and how the program impacted their eating behaviors on a scale of −10 (I am now engaging in much more disorder eating behaviors) to 10 (I am now engaging in much fewer disordered eating behaviors).
One week after the last group session, a 90-min focus group was completed with participants with author R.V. as the facilitator. The focus group semi-structured interview guide was informed by the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009), which is a commonly used implementation science framework to elucidate barriers and facilitators to implementation effectiveness of an intervention across several key domains (e.g., intervention, external setting, process). As part of the “process” domain, we also invited participants to provide feedback on research study procedures (e.g., reminders for group sessions, survey completion, communication form research study team) to inform any refinements in these research activities for the subsequent RCT. See Supplementary Material for the focus group interview guide. The consolidated criteria for reporting qualitative research (COREQ) was used as a guide for the qualitative data (Tong et al., 2007). Participants received compensation for research-related activities, including $25 for completing each of the session-specific feedback surveys and $100 for their participation in the post-program focus group, allowing them to earn up to $250 remuneration for participation in study activities.
Data Analysis of Pilot. Descriptive statistics were used to summarize demographics of the pilot group participants, post-session and post-program satisfaction, and perceived impact ratings. We conducted a rapid qualitative analysis with purposeful data reduction activities where participant's suggestions where consolidated based on common responses and themes on post-session feedback responses to open text questions, as well as the focus group qualitative data. The focus group was recorded and automatically transcribed using Zoom. Two research study staff members (authors E.W. and C.F.) summarized findings from the feedback surveys and took notes during the focus group, aligning with predetermined CFIR-specified domains. Investigators (authors E.W., C.F., and R.V.) used the matrix method to identify main responses across all feedback surveys and the focus group (Averill, 2002; Gale et al., 2013). Qualitative data analysis rigor and credibility were established by independently reviewing, coding, and mapping of data to the matrix, along with discussions between the three investigators involved in this analysis until consensus was achieved. Rapid qualitative analysis has been identified as a time- and cost-effective approach (Nevedal et al., 2021) that allows for timely adaptations to further tailor the fit and relevance of interventions to the needs of specific populations (Lewinski et al., 2021).
All suggested modifications from participants were compiled and reviewed by the research team. While reviewing proposed modifications, the research team prioritized preserving the active ingredient of the intervention (i.e., maintaining dissonance-inducing activities) and protecting scalability of the intervention. The decisions regarding adaptions were made in collaboration with our stakeholders who have expertise in EDs and the Body Project intervention (author ES) or implementation research (author SB). The stakeholders were able to resolve any questions or disagreements regarding the suggested adaptions to make a final decision. The findings from the first three phases of ADAPT informed final planned modifications and adaptations to the intervention, which are reported in the results according to the FRAME framework.
Results
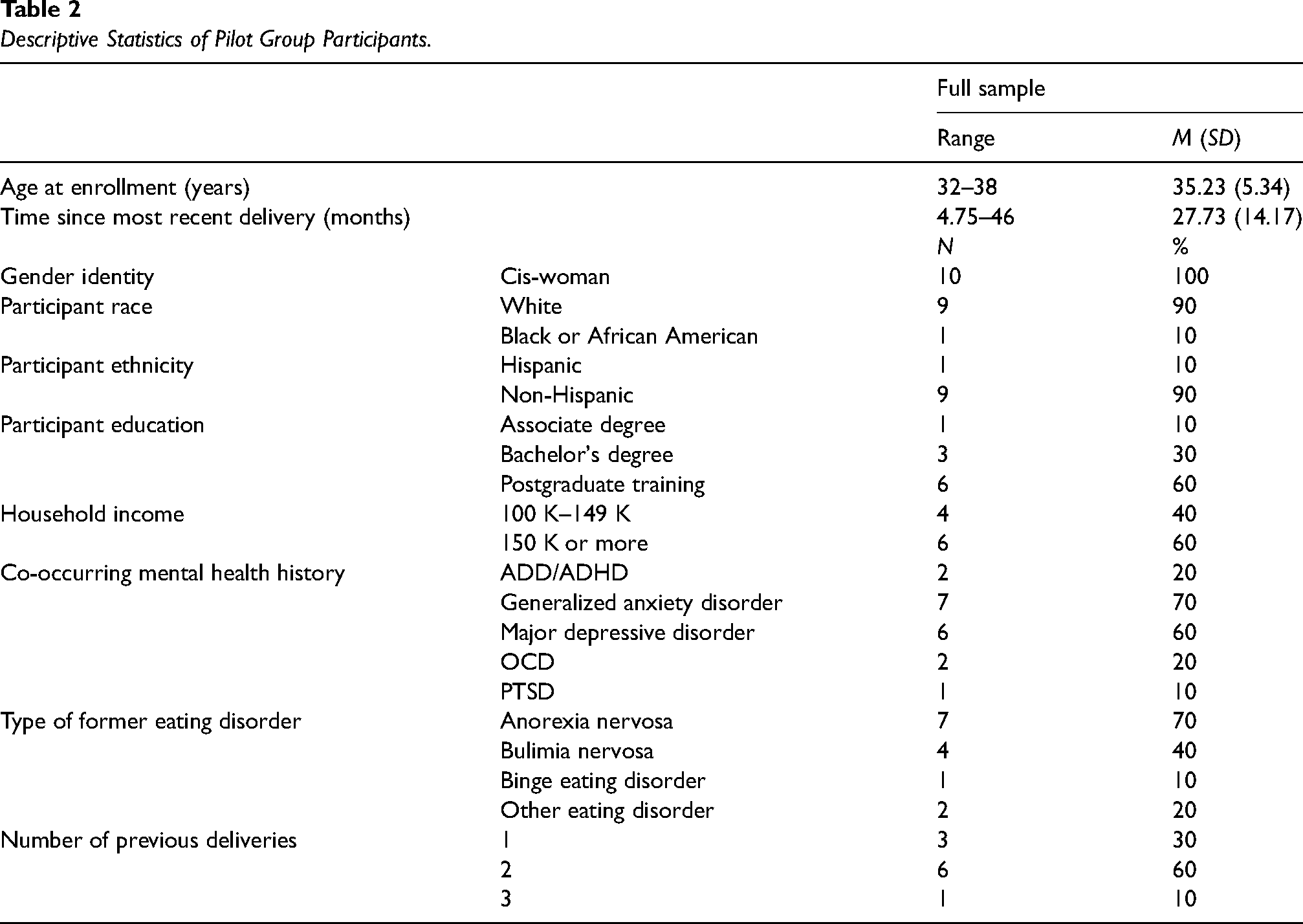
Pilot Study Participants. Over a 1-month recruitment window, 62 inquiries were received. See Figure 1 for study flowchart. Recruitment stopped on September 29, 2023 after 10 participants were determined eligible and consented to participate in the study. Among study participants (N = 10), one was lost to follow-up and never attended any sessions. The majority attended all live group sessions with five participants attending all six sessions, three participants attending five sessions, and one participant attending three sessions. See Table 2 for participant baseline demographics.

Study Participant Flow Diagram
Descriptive Statistics of Pilot Group Participants.
Post-session and Post-program Feedback. Average satisfaction ratings across all six sessions were 9.28 (SD = 0.99, range 7–10). A summary of changes proposed by participants from the post-session feedback surveys (combined with focus group feedback) and our rationale for accepting or declining the suggestions are detailed in Supplementary Material. Most (89%) participants reported that their body image is “better” or “much better” after engaging in the program, the others indicated “no change,” and no participants reported their body image was worse after the programs. Two thirds of participants endorsed no change in their eating behaviors following participation in the program, with many indicating qualitatively that they were “in a good place” with their eating at baseline, and thus there may have not been much room for improvement. The remaining 33% of participants reported engaging in “fewer” or “much fewer” disordered eating behaviors after participating in the program; no participants reported an increase in disordered eating behaviors.
Focus Group Feedback. The focus group began with a discussion of motivators for participation and unexpected experiences with the program. Key motivators included a desire to help others (e.g., wanting to improve the lives of other pregnant individuals) and for self-help or personal growth (e.g., still struggling with body image beyond pregnancy). Additional feedback falling under CFIR domains is summarized in Table 3 and detailed notes regarding modifications proposed by participants are included in Supplementary Material.
Feedback from Focus Group Mapping to CFIR.
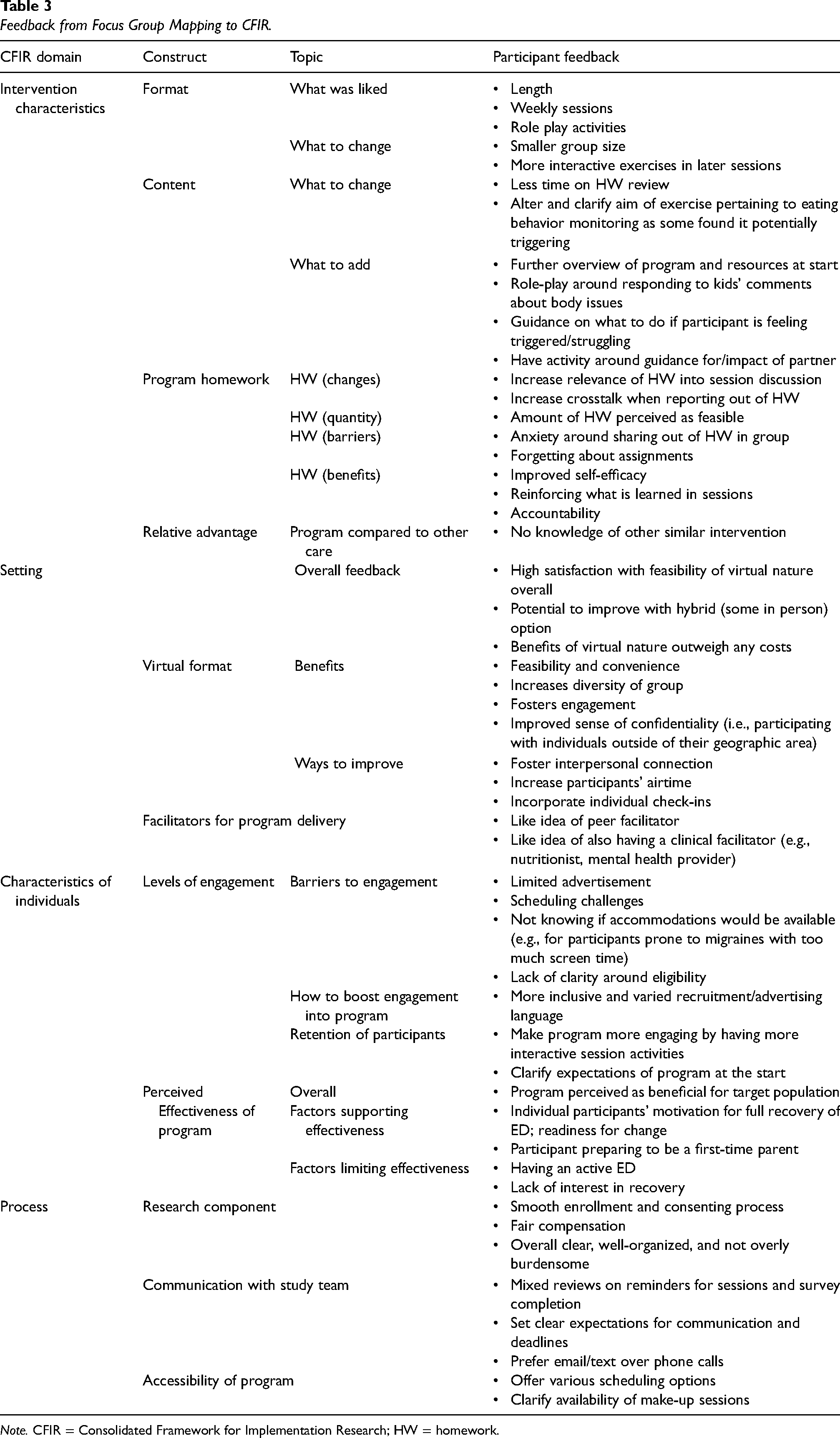
Note. CFIR = Consolidated Framework for Implementation Research; HW = homework.
Final Adaptations Mapped to FRAME. Our compiled modifications, following Steps 1–3 of ADAPT above, are summarized according to FRAME in Table 4. At this phase of work, all modifications are considered “planned” as they were intentionally determined prior to testing the adapted intervention in a future RCT. The research team and stakeholders, following the ADAPT process, participated in the modification decisions. All adaptations were determined to be “fidelity consistent” with the research team's intent of preserving activities that induce cognitive dissonance (i.e., the active ingredient of the Body Project intervention) and scalability.
Summary of Final Planned Modifications Mapped to FRAME.
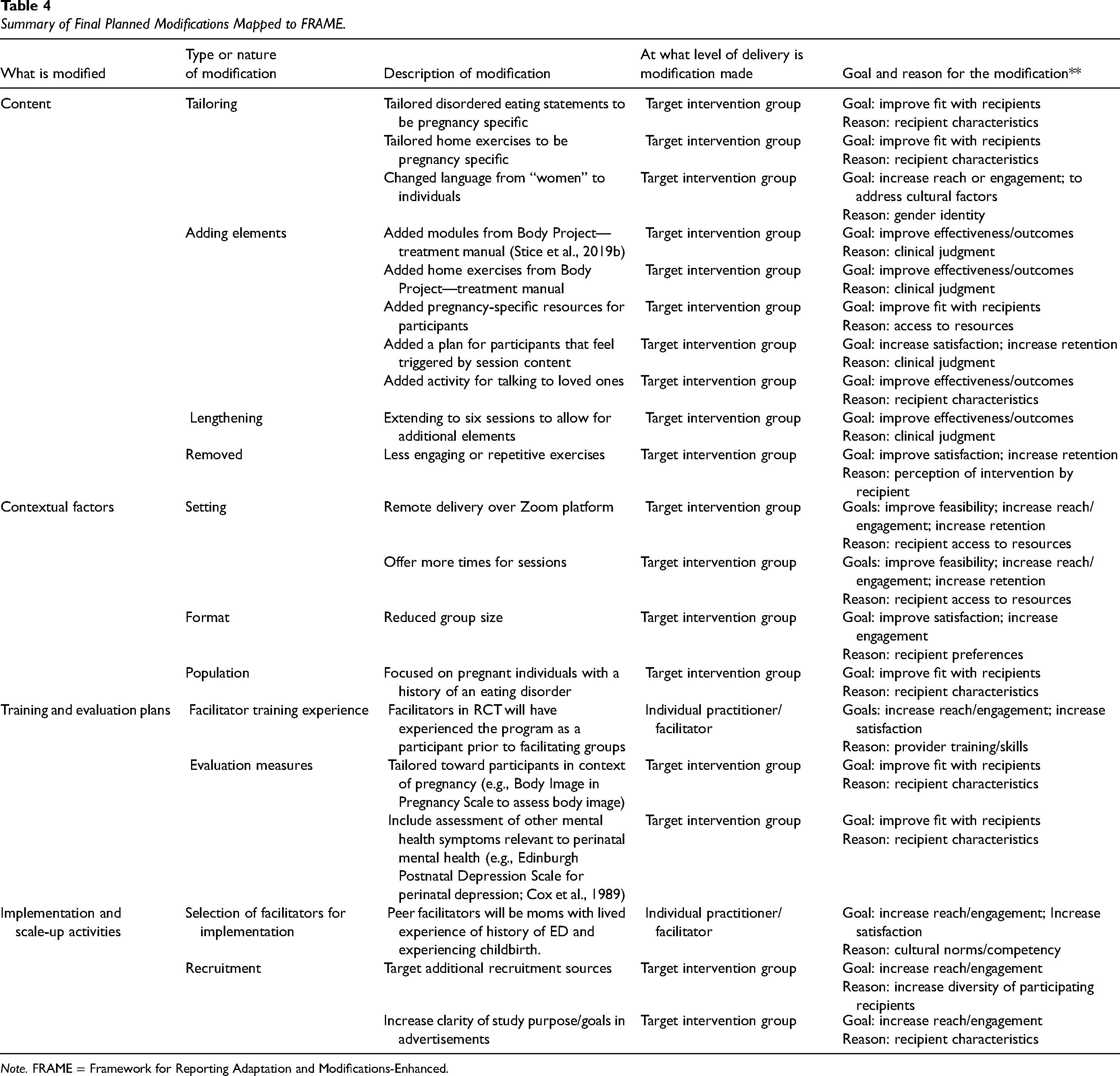
Note. FRAME = Framework for Reporting Adaptation and Modifications-Enhanced.
Discussion
This report describes our application of several implementation science frameworks to guide the adaptation of an evidence-based ED prevention program for at-risk perinatal individuals. Specifically, we utilized the steps described in ADAPT to guide our adaptation process and engaged stakeholders and individuals with lived experience in planning for adaptations of intervention scripts. We then conducted a focus group guided by CFIR among participants in a pilot trial of the adapted intervention to capture feedback on the intervention and its implementation among our target population. All suggestions from participants were reviewed with the research team and expert stakeholders for consideration, and we then mapped final planned modifications to FRAME. At this time, all adaptations and modifications were planned and determined to be fidelity-consistent, with careful attention to preserving cognitive dissonance inducing activities as the active ingredient of the intervention. We plan to further test the adapted intervention in a future RCT comparing the adapted version to an enhanced “usual care” condition to explore the impact of adaptations on implementation and effectiveness of the intervention in pregnancy.
The primary goals for adapting this intervention were to improve fit, satisfaction, and effectiveness with the target population of pregnant individuals who have histories of an ED. Although the Body Project is an ED prevention intervention, we determined it would be important to incorporate in elements of a treatment intervention as well since the target recipients are at elevated risk given their history of an ED. We pulled exercises from the “Body Project Treatment 8.0” manual (Stice et al., 2019b) including an activity where participants discussed the importance of improving body image, as well as activities targeting extreme dietary restriction. Due to the participants’ histories of disordered eating, these additional treatment activities aim to address and target any residual or subclinical symptoms that may remain or go unnoticed. Data collected from our pilot trial indicate high satisfaction ratings among participants, overwhelmingly positive feedback, and perceptions of potential for effectiveness in improving body image and decreasing disordered eating behaviors in the perinatal period. Feedback from the user-centered design (Lyon & Koerner, 2016) also helped to provide further evidence of the utility of and need for this intervention. For example, in both feedback surveys and the exit focus group, participants expressed that the current resources available do not meet the needs of perinatal individuals with body dissatisfaction or eating concerns (e.g., one participant described how an ED group she participated in during pregnancy was too general to address her specific challenges).
Importantly, the user-centered design also detected areas for improvement that we would not have addressed based on the literature and stakeholder expertise alone. Although participants provided thoughtful feedback for improving the program, we were unable to implement all suggestions. When considering which suggestions to accept as modifications, we considered two factors: (a) preserving the active ingredient of the intervention (i.e., maintaining dissonance-inducing activities) and (b) protecting scalability of the intervention. A major consideration in implementation research literature is the importance of identifying “core components” of the intervention and modifying the “form” of the intervention but not the “function” (Perez Jolles et al., 2019; Terrana et al., 2023). For example, participants suggested outlining a clearer plan for what to do during the program if the content feels triggering (e.g., connect with your provider, discuss with the facilitator, etc.). This change improves participant safety and does not negatively impact fidelity or feasibility, so it will be incorporated. Due to similar concerns, another participant suggested having one-on-one meetings between participants and the facilitator a few times throughout the program. Although adding one-on-one sessions may improve comfortability for some participants, and potentially effectiveness, it would also increase the resources (i.e., more facilitator time and effort) needed to deliver the intervention, thus negatively impacting potential for scalability.
Whenever proposed changes were fidelity consistent and did not negatively impact future implementation efforts, they were incorporated, as detailed in Supplementary Material. Our research team had overall strong alignment with regard to deciding which suggested adaptations to accept; however, we engaged stakeholders who are content-area experts in the field as needed for a final decision if there was uncertainty about a given adaptation. The stakeholder's input allowed us to maintain key components of the interventions and appropriately tailor the intervention to the target population, however, engaging stakeholders can add additional complexity as they are not always directly involved with the research procedures and may only be able to provide high-level advice. Researchers may draw on principles of community-based participatory research, for example, guidance pertaining to navigation of differing opinions among research partners (e.g., Mayan et al., 2016). For example, we have incorporated suggestions regarding research study procedures (explored under the “processes” CFIR domain of the focus group) including clarifying expectations for timeframe of survey completion and make-up sessions for the research activities in the subsequent RCT. Expectation setting is an important component of managing the relationship and role of stakeholders and community-partners in the decision-making process for adaptations.
There are several strengths of this study. First, to our knowledge, this is among the first studies aimed at adapting an evidence-based intervention to prevent ED relapse during the perinatal period. Second, the intervention chosen for adaptation, the Body Project, has excellent potential for implementation (e.g., virtual nature, peer-delivery, group-based) and is the most widely disseminated and empirically supported ED prevention program. Third, this work is explicitly mapped onto several implementation science frameworks (ADAPT, CFIR, FRAME) which increases the rigor of the adaptation process and will hopefully enhance efficacy in the target population, paving the way for future implementation efforts. Specifically, ADAPT guided our overall adaptation steps and process, CFIR informed the development of our focus group guide to explore factors influencing implementation of the intervention at multiple levels, and then we mapped all final modifications according to FRAME. Fourth, multiple expert stakeholders provided input on the scripts that was incorporated in the adapted version. Fifth, this adaptation process leverages a user-centered design with numerous points for participant feedback to improve intervention fit with intended recipients. And finally, while a small sample, reported mental health comorbidities appear to align with what is commonly seen among individuals with an ED (Hambleton et al., 2022). It will be important for future research to consider these comorbidities in study samples and transdiagnostic effects when interpreting findings.
There are also study limitations. First, the pilot trial sample was lacking racial and ethnic diversity (90% White, 90% non-Hispanic) as well as socioeconomic diversity (all participants had at least an associate's degree and a household income of more than $100,000). These factors along with the small sample size highlight that these findings may not necessarily be generalizable to a more diverse population. Second, we are delivering this program to English-speaking individuals only which further limits potential generalizability. If feasibility and efficacy are established for this program, we hope to culturally and linguistically adapt it in the future. Third, we only conducted this initial pilot trial with one group. Participants may have been subject to a “group-think” mentality during the sessions or exit focus group, and we may have received different feedback with multiple groups.
Furthermore, while we intentionally invited participants who have already experienced both pregnancy and postpartum, participants were on average over 4 years postpartum and thus their perspectives may not be as accurate to the intended target audience of pregnant individuals. Additionally, we plan to deliver this intervention during early pregnancy with the goal of preventing ED relapse during pregnancy and postpartum; however, some of the effects may diminish by the postpartum period. Given many individuals also struggle with body dissatisfaction during the postpartum period, it is possible some individuals may benefit more from receiving this program during postpartum rather than pregnancy. Thus, we are planning to provide “booster” materials during postpartum to bolster the effects of the intervention and may consider implementation of this program in the postpartum in the future. Finally, we emphasize the potential for broad scalability of the intervention given its virtual delivery by trained nonprofessional peers, however we did not capture the perspectives of potential implementers or maintainers of the intervention regarding the value and feasibility of the intervention. We will explore these perspectives in future research, including collecting feedback from the peer-facilitators implementing the group intervention pertaining to barriers and facilitators to implementation.
Conclusions
We are currently adapting an evidence-based intervention (the Body Project) for pregnant individuals with histories of an ED to prevent ED relapse during the perinatal period. The implementation frameworks utilized as presented in this article served as a helpful guide to inform our adaptation process with an eye toward preserving the intervention's active ingredient and scalability while also considering key factors known to impact implementation. Specifically, ADAPT guided our overall adaptation steps and process, CFIR informed the development of our focus group guide to explore factors influencing implementation of the intervention at multiple levels among participants, and FRAME informed how we reported our final adaptations. In the future, we will further test the adapted intervention in an RCT assessing feasibility, implementation outcomes, and potential effectiveness. By employing a user-centered design, we aim to tailor this intervention program to be feasible, acceptable, and effective for the target population. If the RCT demonstrates that the intervention is feasible and has preliminary effectiveness, we hope to conduct a fully powered efficacy trial. Ultimately, this program aims to improve physical and mental health outcomes for birthing people, infants, and families, thus addressing a critical public health need. This article provides a detailed example of how researchers could approach the adaptation of an evidence-based intervention for a new setting or context as guided by, and mapped to, established implementation science frameworks.
Supplemental Material
sj-docx-1-irp-10.1177_26334895251319811 - Supplemental material for Application of implementation science frameworks to inform the adaptation process of an evidence-based eating disorder prevention program for high-risk perinatal individuals
Supplemental material, sj-docx-1-irp-10.1177_26334895251319811 for Application of implementation science frameworks to inform the adaptation process of an evidence-based eating disorder prevention program for high-risk perinatal individuals by Rachel Vanderkruik, Emily C. Woodworth, Caroline M. Frisch, Stacey Nelson, Madison M. Dunk, Marlene P. Freeman, Lee S. Cohen, Eric Stice and Stephen J. Bartels in Implementation Research and Practice
Footnotes
Acknowledgments
Special thanks to the individuals who participated in the program and provided feedback based on their lived experience.
Availability of Data and Material
The data and materials are not available due to participant confidentiality.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lee S. Cohen, MD—as of February 26, 2024 Research Support: Dr Cohen is an employee of Massachusetts General Hospital, and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–present); Dr Reddy's Laboratories, Inc. (2023–present); Eisai Inc. (2022–present); Otsuka America Pharmaceutical, Inc. (2008–present); Supernus Pharmaceuticals (2021–present); Teva Pharmaceutical Industries Ltd. (2018–present). As an employee of MGH, Dr Cohen works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. Other research support: National Institutes of Health; SAGE Therapeutics Advisory/Consulting: none; Speaking/Honoraria: none; Royalty/patent, other income: none.
Marlene P. Freeman, MD—as of February 26, 2024 Research Support: Dr Freeman is an employee of Massachusetts General Hospital, and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–present); Dr Reddy's Laboratories, Inc. (2023–present); Eisai Inc. (2022–present); Otsuka America Pharmaceutical, Inc. (2008–present); Supernus Pharmaceuticals (2021–present); Teva Pharmaceutical Industries Ltd. (2018–present). As an employee of MGH, Dr. Freeman works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. Other Research Support: SAGE Therapeutics, JayMac. Advisory/Consulting, Data Safety Committees: Independent Data Safety and Monitoring Committees: Janssen (Johnson & Johnson), Novartis, Neurocrine; Advisory Boards: Eliem, Sage; Brainify; Everly Health; Tibi Health; Relmada; Beckley Psytech Speaking/Honoraria: WebMD, Medscape, Pri-Med, Postpartum Support International Royalty/patent, other income: Scale Royalties through MGH Scale, The Massachusetts General Hospital Female Reproductive Lifecycle and Hormones Questionnaire (Freeman et al., 2013).
Rachel C. Vanderkruik, PhD, MSc—as of March 14, 2024 Research Support: Dr Vanderkruik is an employee of Massachusetts General Hospital and works on projects funded by the J. Willard and Alice S. Marriott Foundation and the National Eating Disorder Association. Advisory/Consulting: Dr Vanderkruik consults for the World Health Organization and Soulside, Inc.
All other authors have no competing interests to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Eating Disorder Association (NEDA) Feeding Hope Fund for Clinical Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.