
Abstract
Mobile phone interventions are evidence-based methods for preventing obesity among Latino adults and school-aged children; however, few such interventions exist to improve the obesogenic behaviors of children in the developmentally critical preschool years (ages 2–5). Focusing on this age group is important since over one-quarter of 2- to 5-year-old Latino children are overweight or obese. Moreover, most documented interventions target mothers exclusively, ignoring the influence that other caregivers such as fathers and grandparents have on the environment and the child’s behaviors. We describe the development and refinement of a theory-informed mobile phone intervention using an iterative, user-centered approach that supports healthy weight-related behaviors in preschool-aged Latino children by engaging mothers, fathers, and grandparents. The resulting intervention, Familias Unidas, Niños Sanos (FUNS), is a culturally centered bilingual (Spanish/English), 12-week, web-based mobile phone intervention grounded in family systems theory. Through three to four weekly text messages and links to web-based interactive multi-media content, caregivers of 2- to 5-year-old Latino children learn evidence-based practices to support specific child behaviors in three domains: healthy eating, media viewing, and physical activity. Development of specific messages is grounded in social cognitive theory. Participants can connect with a virtual coach and other participants. The prototype received high levels of acceptability and usability among members of the target audience and is ready for feasibility testing. The systematic process of development and refinement of the intervention can serve as a model for other mHealth interventions, addressing the ongoing critique of the general lack of theoretical application in such intervention work.
After decades of rising obesity rates in the United States, emerging research suggests stabilization and even a decrease in childhood obesity prevalence among some racial/ethnic groups (Cunningham et al., 2022; Rafei et al., 2022). However, the upward trend in obesity prevalence has not reversed for Latinos (Ogden et al., 2022). The preschool age (2–5 years) is a critical period in the developmental origins of obesity during which higher-than-expected weight gain increases the risk of adolescent and adult overweight. These trends present an important public health challenge, since Latino children have a high prevalence of obesity, and Latinos account for a large and growing proportion of American youth (Ogden et al., 2022). Although relatively fewer young Latino children are overweight or obese, compared with older children, the ages of 2 to 5 offer a critical window for intervention (Pan et al., 2014; Taveras et al., 2010). Establishing healthy weight-related behaviors for young Latino children has critical implications for obesity-related comorbidities and health disparities throughout the life course.
Early childhood interventions can shape long-term health behaviors and weight outcomes for young children (Hammersley et al., 2016). Parent-focused interventions delivered in person have been shown effective in establishing healthy weight behaviors in young Latino children (Arredondo et al., 2018; Ayala et al., 2010; St. George et al., 2022; Tovar et al., 2023; Ullevig et al., 2023). Parent-focused behavioral interventions for childhood obesity prevention aim to support the development of positive parenting practices surrounding obesogenic behaviors. These include, for example, developing the skills to refuse children’s requests for foods advertised on television, setting and enforcing limits on screen time, and offering foods multiple times. The interventions that have proven effective on at least some intended outcome have been culturally adapted and are delivered by culturally consonant health educators. Specific features that make parent-focused interventions effective for establishing and maintaining young Latino children’s healthy weight behaviors include group learning, problem-solving, and support strategies that are essential for behavior change. However, the widespread dissemination of these effective parent-focused interventions delivered in person is made difficult by significant barriers including time and cost for delivery, need for transportation, and English-language proficiency (Arai et al., 2015; Ghai et al., 2014; Jensen et al., 2012).
Moreover, most early childhood obesity interventions focus exclusively on mothers, an oversight that precludes leveraging familial mechanisms to shape early childhood weight-related behaviors. Overwhelming evidence demonstrates that fathers, grandparents, and other caregivers play a direct role in food selection, grocery shopping, meal preparation, feeding, and the physical activity and inactivity (e.g., TV watching) of young children (Guerrero et al., 2016; Marr et al., 2021; Mena et al., 2015). Family members indirectly influence child weight-related behaviors by undermining maternal-driven dietary and activity changes in the home food and activity environment and by role modeling (poor) dietary and physical activity behaviors (De-Jongh González et al., 2021; Villegas et al., 2023); as such, engaging multiple caregivers in obesity prevention interventions for young children is essential. The involvement of multiple caregivers may be particularly relevant for Latinos, given both their well-described emphasis on the cultural values of familism and collectivism (Ramírez et al., 2018) and their relatively high rates of multigenerational caretaking (Bengtson, 2001).
Mobile health (mHealth), the use of mobile and wireless devices to improve health outcomes, health care services, or health research, has the potential to address many of these challenges. mHealth interventions can provide significant reach and engagement of a large population, leverage increasingly prevalent and powerful smartphones, and offer diverse modalities (i.e., text, voice, video) to deliver practices and resources to support behavior changes. Systematic reviews of pediatric obesity mHealth interventions provide some evidence of utility by promoting the use of behavior change techniques such as goal-setting, self-monitoring, reminders, feedback, tips, and advice (Turner et al., 2015).
Current pediatric obesity interventions using mHealth have several limitations. The mobile component is often just one aspect of a multicomponent program that requires in-person sessions and thus suffers the same transportation and time barriers as usual care interventions. Another limitation is delivery of content in one language, ignoring the widespread preference for the hybrid “Spanglish,” the growing use of English among U.S. Latinos, and the linguistic diversity within families (Krogstad & Gonzalez-Barrera, 2015). Moreover, despite the general description of Latino-targeted interventions as “culturally-tailored,” the specific features that make such interventions culturally consonant are rarely described, beyond linguistic choice. There is a need, therefore, to unpack this “black box” of cultural tailoring through well-theorized, operationalized, and tested messages.
In addition, mHealth components or interventions typically focus on influencing the behavior of a specific individual, and thus do not incorporate the group-based behavior change techniques—group learning, problem-solving, and support strategies—that have been the cornerstones of effective parent-focused pediatric obesity interventions (Militello et al., 2012). Furthermore, this focus on a single individual in a family fails to capitalize on the reach and engagement potential of mobile technologies, missing the opportunity to engage other family members whose roles influence children’s weight-related behaviors (X. Wang et al., 2022).
Another critique of existing mHealth interventions is the lack of explicit theory guiding their development (Chib & Lin, 2018; Gomes et al., 2021). Although plentiful theory guides interventional techniques to accomplish behavior changes relating to diet, theoretically driven approaches to the intervention design process itself—the integration of multiple forms of theory—are largely absent. For example, the design process may draw upon theories of persuasion, marketing, and information processing in addition to principles of behavior change to create an appropriately participatory and engaging intervention (Jessen et al., 2018; Kelders et al., 2012). In addition to theories about the intervention components and individual behavior change, dynamic contextual factors are highly relevant to the user interaction that dictate engagement with, and, ultimately, effectiveness of the intervention.
Objective
To prevent and control obesity among preschool-aged Latino children, we designed an interactive mHealth intervention that used culturally and contextually appropriate caregiver strategies to support evidence-based, age-appropriate behaviors. This article describes the development of a theory-informed intervention, Familias Unidas, Niños Sanos (FUNS), corresponding to Stage 1a of the National Institutes of Health Stage Model for Behavioral Intervention Development (intervention generation) (Onken et al., 2014). During this phase, we sought to evaluate the acceptability and usability among the intended audience.
Methods
This project followed a user-centered design approach consistent with best practices (Perales-Puchalt et al., 2022; Vilardaga et al., 2018; Whittaker et al., 2012). We describe the five stages of design.
Stage 1: Selection of Design Principles for Intervention Design
We first determined key principles for designing the intervention.
Intended Audience
We began by considering the home environments of and sources of social influence on preschool-aged Latino children. In this study, multiple caregivers including mothers, fathers, and grandparents are the intervention targets.
Family Interaction Theory
Building on our design decision to include multiple caregivers with distinct familial roles, our second design principle was consideration of how these distinct family caregivers interact with each other and with the young children in their care. Applying a family systems perspective, we considered the multiple and complex subsystems that influence behaviors associated with childhood obesity, including the home and family environments (Halliday et al., 2014; Novak et al., 2023).
A simplified way of understanding the family unit’s influence on weight-related behaviors during early childhood may include caregiver weight status and their own eating behaviors, the types of food available in the home, and specific child feeding practices by a caregiver (i.e., restricting foods by mealtimes, amounts, or types; or, conversely, pressuring consumption of specific foods or quantities). However, child and family member interactions surrounding weight-related behaviors are dynamic. For example, the caregiver’s feeding practices may vary based on the child’s food preferences and temperament (i.e., pressuring a picky eater to finish the food served on their plate). There may be consensus or disagreement between family members on a child’s eating behaviors, such as the types or amounts of foods the child should consume. The generational or gendered hierarchy of family members caring for the child may affect the relative influence of the caregiver on the child’s behaviors; for example, grandparents may be permitted to be more indulgent or stricter than parents; mothers may be taken less seriously than fathers, or vice versa. Young children’s weight-related behaviors also are influenced by the strategies used by caregivers to control other behaviors. For example, caregivers may use a “special” food treat as an inducement to stop crying, or as a reward to reinforce a positive behavior. In turn, these diverse family and home environment contexts and specific caregiving strategies influence the child’s development of appropriate self-regulation of hunger, potentially reducing attention to fullness cues and self-regulation of intake in favor of responding to caregivers’ cues. Although this is not an exhaustive list of the multiple ways in which the family unit may influence early childhood weight-related behaviors, it highlights the multiple and complex opportunities to intervene with family-based prevention and management programs.
The intervention design integrated these family dynamics and influences on child weight-related behaviors. Specifically, we sought to positively influence the home and family environment to support healthy weight-related behaviors of preschool-aged children by (a) aligning caregiving practices with national pediatric guidelines (described below); (b) facilitating intra-familial consensus on healthy child weight-related behaviors; and (c) minimizing the use of food or treats to manage children’s behavior.
Behavior Change Theory
At the individual behavior change level, the intervention design was guided by principles of Social Cognitive Theory, principally via observational and social learning strategies (Bandura, 2002). These theoretical components were operationalized and translated into strategies that shaped the key content and activities of the program (Figure 1).
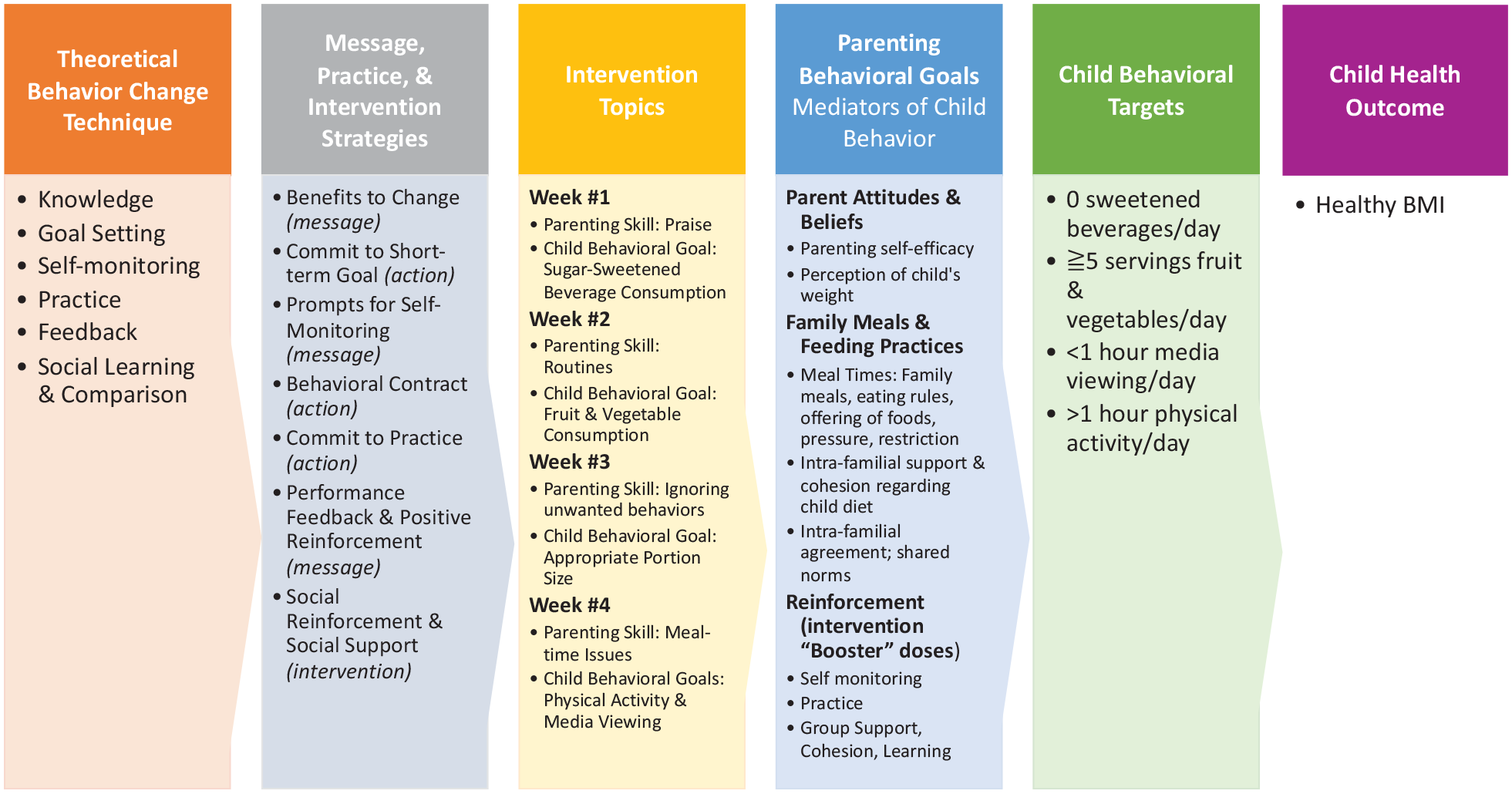
mHealth Intervention Logic Model.
Stage 2: Platform Selection and Vendor Collaboration
Most mHealth interventions rely on a single modality (i.e., text) and deliver messages only to individual participants who have signed up for the intervention. Recognizing the important role of social support, some mHealth interventions have included cooperative or competitive social network components (Fiks et al., 2017; Militello et al., 2012). However, these have required participants to use two wireless modalities (e.g., mobile phone texting and a separate social media platform such as Facebook), which can reduce participant engagement, especially among low-income and ethnic minority populations (Gonzalez et al., 2021; Manganello et al., 2016). Moreover, the social networks usually comprise other intervention participants, with similar roles and behavior change goals—likely strangers prior to the intervention. Since intra-family caregivers are essential intervention targets, and we conceptualize the dynamic relationships among these as part of the motivation for the intervention, we needed a platform that could facilitate community and communication both within a family unit and with other intervention participants such that grandmothers could connect with other grandmothers. Thus, an important design decision was the selection of a platform that includes an online community.
Another important technological dimension—again stemming from the overarching principle of the family system which emphasizes multigenerational participants—was the need to incorporate multiple message modalities to address the distinct needs and preferences of multigenerational, multilingual families wherein family members potentially had different levels of education, literacy, and health literacy. We wanted to provide content that could meet participants at their levels of literacy and health literacy, and engage them long enough to sustain behavioral effects (Muir et al., 2021). This requires multiple modalities, a “transmedia” approach (Jenkins, 2006; H. Wang & Singhal, 2016).
For this study, then, we leverage a robust mHealth platform that allows us to deliver the multimodal intervention components exclusively via mobile phone. Specifically, we selected the Chorus application, a mobile platform that provides texting, a web application, and an online community. Users interface with Chorus by clicking on a hyperlink embedded in a text message sent to their phone. Web-based interactions include prompts and clicks (e.g., “click on the ‘next’ button to continue,” “click below to watch a brief video,” “click on the ‘picture’ box and upload your image”). Chorus has been approved by the Office of Information Security at the University of California, Los Angeles, for collection and storage of personal health information. The single, unified platform offered by Chorus features relatively intuitive content creation (Arevian et al., 2018).
Stage 3: Evidence-Based Foundation
While the ultimate intended outcome of this intervention is the healthy weight of preschool-aged children, consistent with behavior change theory and a family systems framework, the specific goals of the intervention were to modify caregiving behaviors that influence those outcomes in three distinct behavioral contexts. Specifically, we looked to the American Academy of Pediatrics (AAP) guidelines for healthy eating (three specific behaviors: limiting consumption of 100% fruit juice to 4 ounces per day; avoiding sugary-sweetened beverages altogether; and aiming for five servings of fruits and vegetables per day), media viewing (limiting screen time to 1 hour or less per day), and physical activity (incorporating one hour of physical activity per day) in preschool-aged children (Barlow & Expert Committee, 2007).
To help caregivers support these behaviors, we incorporated multiple strategies. For example, we began by providing education about the AAP’s guidelines. Then, we helped to build caregivers’ health literacy by teaching them how to read nutrition labels.
Drawing upon effective early childhood obesity interventions, we integrated caregiving practices to support healthy weight-related behaviors. These practices align with family systems and transactional parenting theories that address the importance of how caregivers influence children’s innate hunger and fullness cues; respond to child food preferences and temperament; and may or may not have concordance with other family members around eating practices and food choices for children. The intervention emphasized the common ways in which caregivers may unintentionally override fullness cues by controlling or pressuring children’s intake. Caregiving skills to praise and manage children’s behaviors without the use of food or sweets also were emphasized.
Stage 4: Prototyping: Integration of Theory, Platform, and Evidence
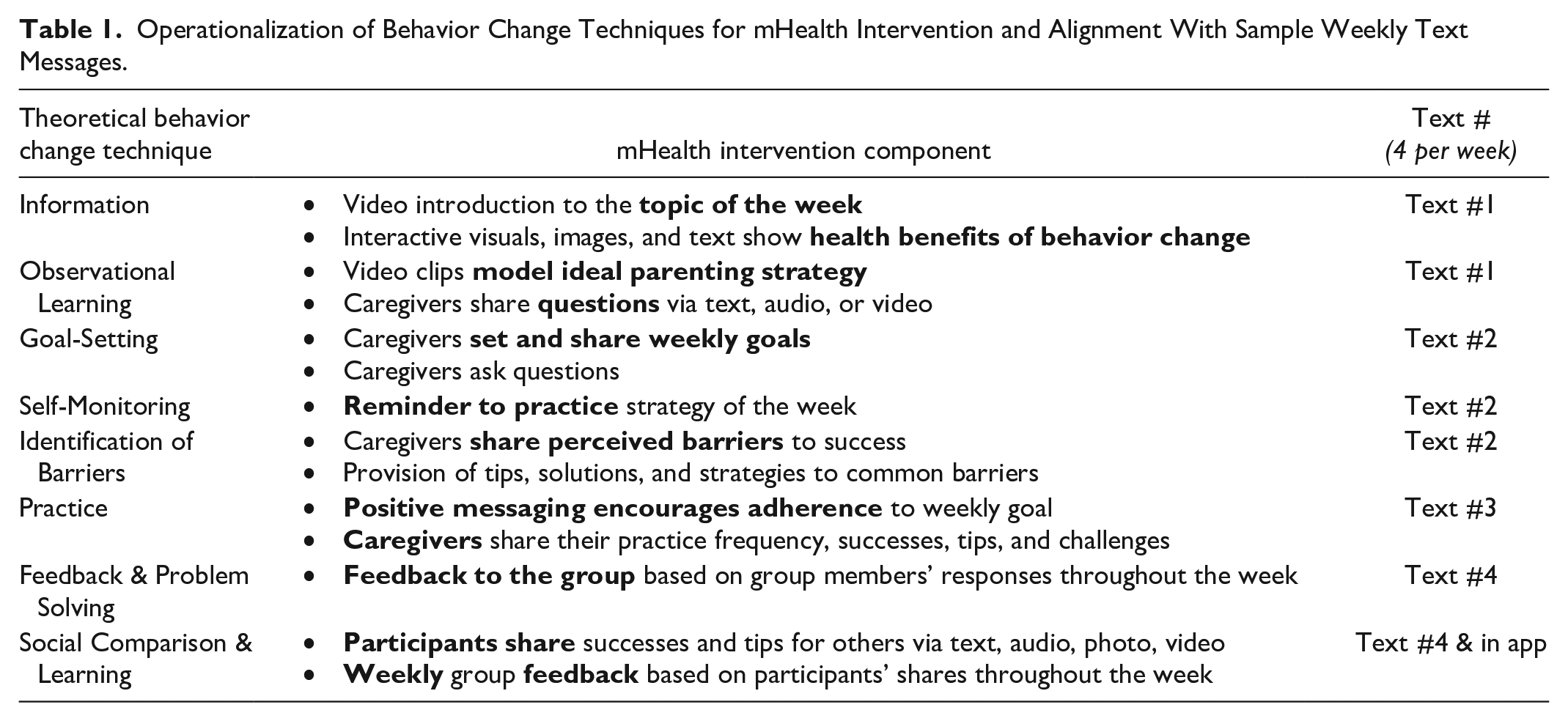
Using the principles and results from the prior stages, we built a prototype. We determined that the intervention should last four weeks, each focused on a specific caregiving strategy (Figure 1, weekly topics). Each week, caregivers received four text messages to support the targeted topics (Table 1); clicking on the embedded link would navigate caregivers to the interactive content including images, text, videos, and prompts. Caregivers shared their goal(s), perceived barriers, questions, tips and strategies that could be helpful to other participants. In addition, caregivers received strategies, and group feedback on changing unhealthy behaviors. The content shared by caregivers was summarized and sent back to participants each week.
Operationalization of Behavior Change Techniques for mHealth Intervention and Alignment With Sample Weekly Text Messages.
Stage 5: Acceptability and Usability Testing
The specific aim of the acceptability and usability testing stage is to ensure that the ways distinct components of the intervention are put together will be acceptable to and usable by the intended audience (Whittaker et al., 2012). We conducted focus groups with mothers, fathers, and grandparents who care for 2- to 5-year-old children. The sessions were conducted in-person or by phone in English or Spanish depending on participant preference and were audio recorded and transcribed.
Sample, Recruitment, and Data Collection
We conducted a total of eight focus groups with mothers (N = 11 English-speaking; N = 36 Spanish-speaking) and grandmothers (N = 5 English-speaking; N = 16 Spanish-speaking) and a total of 20 in-depth interviews with mothers, fathers, and grandmothers. Participants were recruited from two partner WIC (Women, Infants, and Children) centers in East Los Angeles, where low-income Latino families with children aged 0 to 5 years receive various social and medical services. Eligibility criteria to participate in the study included male or female adults who (a) self-identify as Latino; (b) are the mother, father, or grandmother of a 2- to 5-year-old child; (c) speak Spanish or English; (d) own a smartphone; (e) are willing to receive and interact with text messages on parenting, dietary, and physical activity strategies for young children during a focus group; and (f) have the ability to understand the study and participate in a focus group. Participants received a US$25 gift card.
The open-ended interview guides were designed to assess six specific domains related to acceptability and usability: (a) the linguistically and culturally appropriate terms (e.g., formal or informal terms to address intervention participants); (b) acceptability of sharing text, pictures, videos, and audio to support group learning strategies; (c) preferred group strategies for learning (e.g., group feedback); (d) ease of using interactive texts; (e) ease of completing prompted tasks pertaining to the web-based application (e.g., uploads and replies using texts, images, videos, and audio files); and (f) ease of navigation of the interactive texts and online content.
Focus group participants were first asked to share their thoughts and experiences with the use of digital applications to support health and then about using a phone-based application to support healthy weight behaviors of young children. Then, participants were sent a simple text message with a link to the proto-typed web-based application and given a few minutes to open the link, review the multi-media content, and interact to advance the content. Participants were asked about the usefulness of the skill and topic; the appropriateness of word choices; preferences for visuals (specifically, digital/cartoon versus photorealistic); ease of using icons to advance each message, play the video, and reply to closed- and open-ended questions; and preferred ways of interacting with other caregivers for support. We also asked specific questions about intervention design such as message frequency.
For the purposes of analyses, we combined the qualitative data (N = 93 participants). Most were mothers (65%); the average age of mothers was 35 and 61 years for grandmothers. Consistent with national and regional demographics, approximately two-thirds were of Mexican origin.
Ethics Approval
The study was approved by the UCLA and WIC Institutional Review Boards.
Data Analysis
Focus groups and interviews were audiotaped and professionally transcribed and analyzed in the original language using pragmatic approach to grounded qualitative analysis (Glaser & Strauss, 2017). Two authors independently conducted multiple read-throughs of the transcripts to identify emergent themes and synthesize the data into the a priori domains of acceptability and usability. The two authors then met to discuss their findings, and differences were resolved by consensus.
Results
This section focuses on Stage 5 of the user-centered design. First, we summarize the main themes. Then, we describe how those results informed efforts to adapt and refine the intervention.
Theme 1: About the Intervention
In general, participants were highly supportive of the intervention guiding principles, including the focus, modality, and need to engage fathers and grandmothers. Parents appreciated the opportunity to discuss the challenges of parenting little kids. There was enthusiasm for discussing healthy lifestyles, and strong awareness of the general roles of physical activity and nutrition in promoting children’s health. However, participants were unsure about specific ways to promote healthy behaviors and wanted a deeper understanding of how family caregivers can support healthy development. The idea of an intervention delivered via mobile phone was strongly endorsed. All were experienced using mobile phones for a variety of purposes, including for some health behavior coaching. Both cartoon and real-world images (i.e., photographs) were positively received; a combination was encouraged. The most emphatic comments in response to questions of usability came with respect to the use of multiple distinct modalities; video content was specifically called out as being useful.
Theme 2: Intervention Tailoring
The second emergent theme relates to the dimensions of the intervention that participants would like to customize for themselves—the tailored components of the intervention. There were three distinct preferences for message tailoring components: format; time of content delivery; and level of interactivity. With respect to format, some participants preferred text-based over web-based content. Participants also expressed different preferences for timing: Some preferred receiving the messages first thing in the morning so that they could focus on the ideas and perhaps put some into action throughout the day. Others preferred messages at the end of the day, so they could prepare for the next day.
Interactivity came up in the context of the coaching call. One part of the prototype intervention was a mid-week live coaching call delivered to the entire cohort of participants remotely. There was general enthusiasm for the didactic portion (the coach delivering information), and participants reported they would be willing to watch a recording of the session if they were unable to attend live. However, there was less enthusiasm for the idea of active participation: While a few participants said they would participate in a virtual video and voice meeting, others would participate only via audio, and there was a general lack of interest in live active engagement.
The different levels of interactivity also related to participant preferences in sharing progress and receiving feedback. The intervention aims to help participants learn optimal caregiving behaviors, identify their own current behaviors, set goals for adjusting these to support their child’s weight-related behaviors, and monitor progress. As such, the prototype integrated the opportunity for participants to report goals and progress within the application, and then to compare their progress with that of others in their cohort. There was widespread support for the individual-level tracking, and in terms of usability, participants were enthusiastic about interacting via a combination of open-ended and multiple-choice questions. However, the comparison with others was less universally supported. Some participants were concerned that they (or others) may be made to feel badly about their own progress. Others saw competition in a positive light and could imagine being motivated by such comparisons; some saw the opportunity to provide positive social support to cohort members who were struggling.
Theme 3: Message Tone
The third theme relates to the tone of the messages. We consider this a significant and important component of the cultural tailoring needed for effectively intervening with Latino families. Participants expressed specific cultural and linguistic preferences in response to questions about specific stylistic conventions. Beyond differences in the Spanish-language formal and informal address, there were specific linguistic formulations that were preferred by participants, and which helped to make the intervention more culturally consonant. These distinctions in general did not vary by language preference of the participants.
Final Product
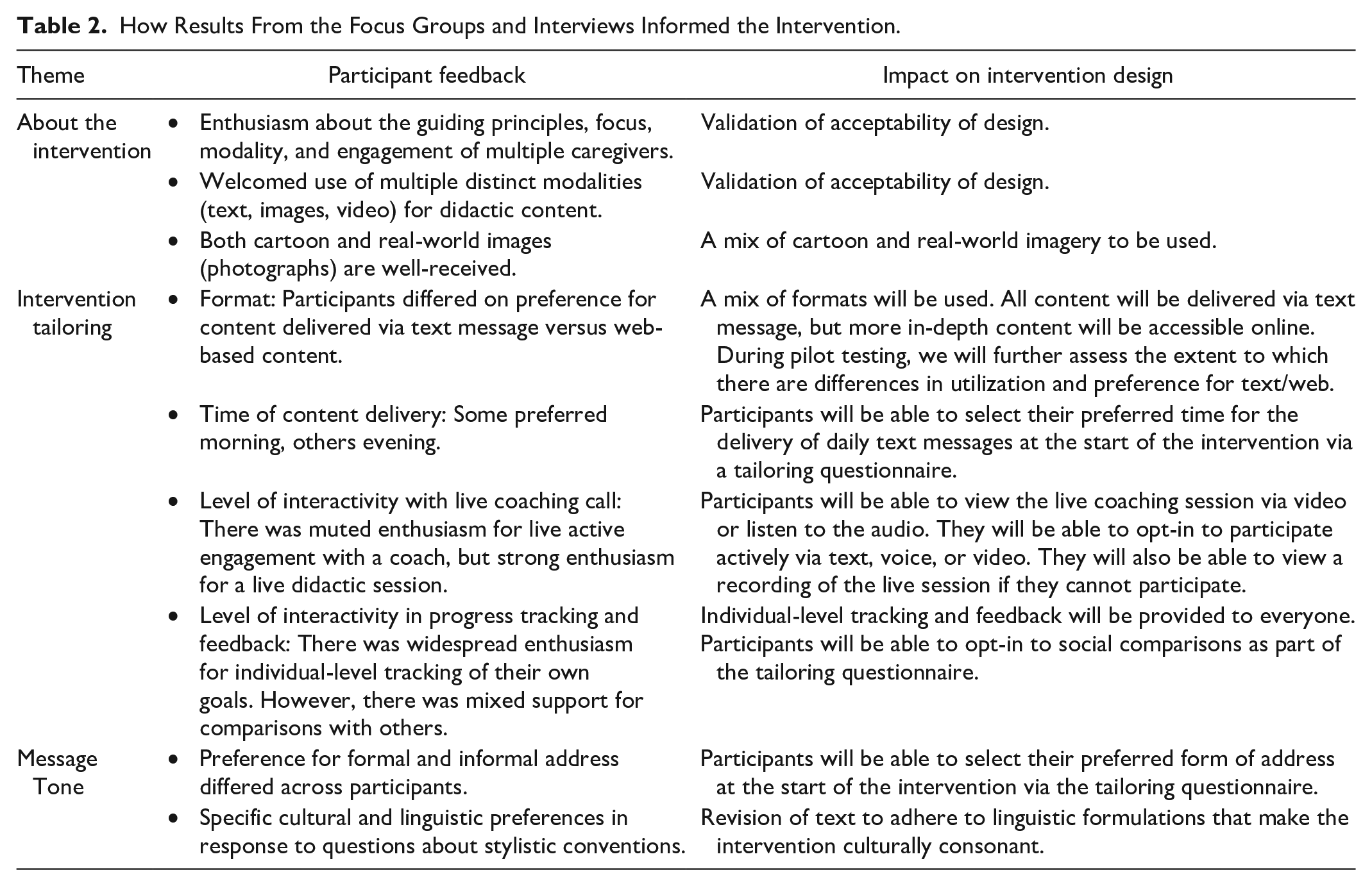
In response to findings, we revised the prototype intervention with the following decisions (Table 2): (a) end-of-the-week feedback and progress; (b) including message delivery time in the tailoring menu at the time of enrollment; (c) using both open-ended and multiple-choice questions; (d) using a variety of images including cartoon-like and real-life images; and (e) providing caregivers the flexibility of joining audio or audio plus video during mid-week coaching sessions (Figure 2).
How Results From the Focus Groups and Interviews Informed the Intervention.
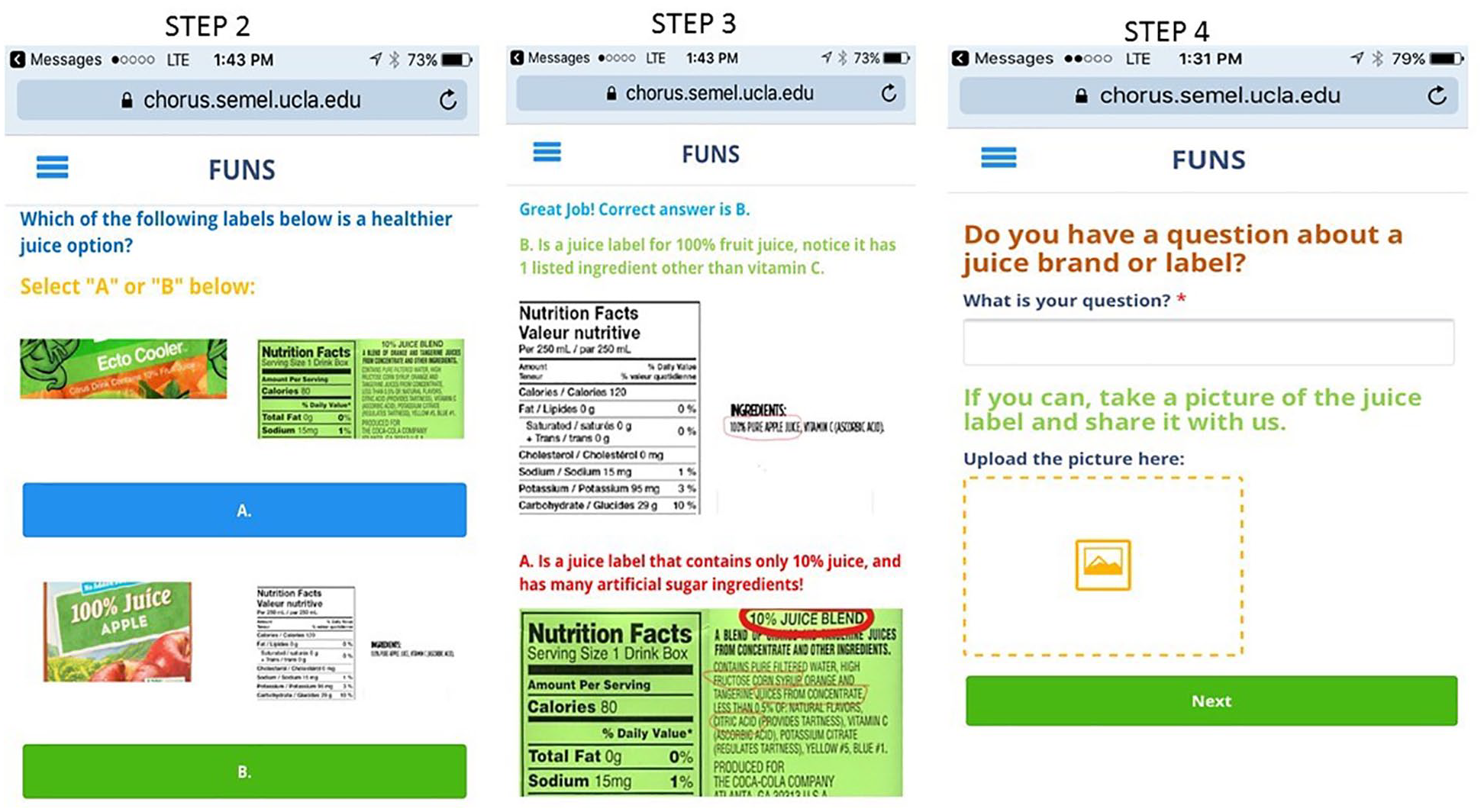
Screenshots of the Familias Unidas, Niños Sanos (FUNS) mHealth Intervention Prototype.
Discussion
The resulting intervention merges the evidence-based components and strategies of both in-person and mHealth childhood obesity interventions. In so doing, we maximize the opportunities afforded by advancements of web-based mHealth platforms that can address various levels of literacy, health literacy, and mobile phone proficiency, and capitalize on the high mobile phone ownership among Latinos to address the methodological and knowledge gaps of stand-alone mHealth interventions targeting weight outcomes in Latino preschool children.
Evaluating the acceptability and usability of the Familias Unidas, Niños Sanos (FUNS) intervention provides evidence that there is an interest among Latino caregivers of young children to use smartphones to support parenting and healthy weight-related behavior of preschool-aged children. This interest emerged in various ways including unanimous feedback that caregivers would use the application, welcomed, and valued the inclusion of multiple family members, and could learn from the content of the application.
In our exploration of usability, all three types of caregivers reported ease in using the different intervention components. To our knowledge this is the first study to include Latina grandmothers of young children in the development of a mobile phone intervention. This area of research merits further work, since nearly half of grandparents play a central role in caregiving for young Latinos (The Annie E. Casey Foundation, 2023). This project was a first step in bringing families together to learn caregiving strategies to support healthy weight-related behaviors among preschool-aged Latino children.
Results informed the refinement of the intervention components. Caregivers voiced preference for cartoon and “real-life” images, a combination of open-ended and multiple-choice questions, and offering options for delivery timing. Allowing for such tailoring aligns with patient- and family-centered approaches allowing families to design intervention aspects that will provide the greatest utility or value (McGrady et al., 2021). Finally, this study demonstrates approaches to the inclusion of family members in health behavior interventions. Despite overwhelming evidence that family and peer relationships are critical to support disease management and health-related behavior changes, few studies operationalize family and social support. Pediatric Type I diabetes family-focused intervention studies could provide some guidance, especially for how to build family consensus, given the degree of family involvement needed to manage a child’s T1D (Case et al., 2021; Ispriantari et al., 2023).
This study had several limitations. Consistent with our model of effects and family systems theory, we sought to develop an intervention that would incorporate various types of familial caregivers; however, we were unable to recruit many fathers. Recruiting Latino men into health research is a widespread problem and one that deserves more attention (Valdez & Garcia, 2021), and is particularly relevant, as we have highlighted, for child obesity prevention. In recognition of this limitation, as well as of other research suggesting that it is Latina grandmothers—to a much greater extent than grandfathers—who play a uniquely significant role in caretaking for their grandchildren, we decided a priori to focus on recruiting grandmothers. This could be seen as a capitulation to existing gender norms, adding to the burden placed on women in the family. While this is a legitimate concern, addressing multigenerational gender equity issues in caretaking is beyond the scope of this study. We do believe that efforts to include both-gender parents—while not perfectly successful in this study—are essential both for gender equity and child obesity prevention. A second limitation was the uneven engagement with types of content by some caregivers, which might be attributable to the relatively late engagement of members of the target audience in the design process. For example, images used for the content of the prototype were selected by bilingual and bicultural research team members; while they were received positively, Latino caregivers may have provided more meaningful contributions. In addition, the lack of scales for the measurement of acceptability and usability outcomes is a limitation. Social desirability bias in focus group participation may taint our findings that are based on consensus. The individual interviews, however, had concordance with the themes identified in the focus groups, suggesting little evidence of social desirability bias. Finally, we recognize that an education-focused intervention addresses but a single, albeit important, dimension of obesity prevention. To achieve health equity, interventions should consider the environments and social determinants that contribute to obesity disparities.
Conclusion
This study provides preliminary evidence of the acceptability and usability of a mobile health intervention to prevent obesity among preschool-aged Latino children by engaging multiple family caregivers. By paying careful attention to cultural and linguistic preferences and linking theoretical grounding with the application of evidence-based strategies, we developed a prototype intervention that has the potential to address a significant public health challenge. The resulting intervention is ready for feasibility testing (Stage 1b of the National Institutes of Health Stage Model for Behavioral Intervention Development; Onken et al., 2014).
Beyond the intervention itself and its potential impact for health equity, the systematic process we described for the development and refinement of the intervention is a unique and important contribution to the literature on obesity prevention interventions. Our efforts to describe each decision point and stage of the intervention development process are important for unpacking the “black box” that so often is ignored in reports of intervention effects. Through our transparency, we hope to illuminate the many decision points that are involved in designing an obesity prevention intervention, and the ways in which multiple levels of theory and evidence are integrated creatively. We hope the systematic process we describe will serve as a model for other culturally tailored, theory-grounded, and user-centered mHealth interventions.
Footnotes
Author Contributions
A.S.R. contributed to the original grant application, provided input into the intervention and evaluation designs, analyzed the data and wrote the manuscript. G.X.A. contributed to the original grant application, provided input into the intervention and evaluation designs, and edited drafts of this manuscript. M.M. supervised focus group studies and transcription of audio data; analyzed the data; and reviewed drafts of this manuscript. D.G. contributed to the original grant application and edited drafts of this manuscript. A.D.G. conceptualized the intervention, obtained the funding, supervised the study, analyzed the data, and contributed to manuscript writing. All authors approved the final submitted version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Institute of Child Health and Human Development under Award No. R21HD096298 and by the National Institute of Diabetes and Digestive and Kidney Diseases under Award No. P30DK092924. Additional support was provided to Ayala from the National Institute on Minority Health and Health Disparities (U54MD012397, S21MD010690). Contents are solely the responsibility of the authors. We thank Erika A. Hernández for her expertise and support in facilitating the study focus groups.