
Abstract
Background
Smoke-free policies are often poorly implemented in schools. The Smoke-Free Vocational Schools intervention aimed to support the routine implementation of a comprehensive school tobacco policy at Danish vocational schools and took place across seven schools. This study aimed to assess and understand the mechanisms—that is, reasoning and behavior change—that shaped if and how policy implementation outcomes occurred.
Method
We applied a convergent mixed-methods design informed by Normalization Process Theory (NPT). The quantitative strand employed a repeated cross-sectional design, assessing implementation mechanisms—Coherence, Cognitive Participation, Collective Action, Reflexive Monitoring—and implementation outcomes at two time points: 5+ months post-policy (T1) and 14+ months post-policy (T2). Additional mechanisms—Change Commitment and Change Efficacy—were surveyed among subsamples who completed questionnaires pre-policy (T0) and at the follow-ups (i.e., T0–T1 and T0–T2). The qualitative strand involved interviews and focus groups with 40 participants to explore the mechanisms and their connections to intervention activities. Integration of qualitative and quantitative findings was achieved through joint displays.
Results
Quantitative analyses included responses from N = 419 participants at T1, N = 452 at T2, N = 209 at T0–T1, and N = 182 at T0–T2. All implementation mechanisms were significantly and consistently associated with the total implementation outcomes score. Coherence encompassed the perceived meaningfulness of the policy, for example, believing the policy was a school responsibility. Cognitive Participation was related to policy legitimacy, for example, enforcement legitimacy beliefs. Collective Action involved practical implementation efforts, for example, enforcement and communication strategies. Reflexive Monitoring encompassed perceived policy impacts, for example, reduced smoking visibility. Change Commitment and Change Efficacy were found to be closely interrelated with the other mechanisms. Moreover, qualitative analysis revealed plausible connections between intervention activities and mechanisms.
Conclusions
This study identified critical mechanisms for implementing school tobacco policies and demonstrated how specific intervention activities can activate these mechanisms, offering guidance for future research and practice development.
Plain Language Summary
Many schools have rules against smoking, but these rules are not always effective in protecting students from being exposed to smoking. In many cases, smoking is banned only on school grounds, which means that students may still gather just outside the school gates to smoke. This makes smoking visible and normal in young people's daily lives. A more comprehensive approach is called smoke-free school hours. With this type of policy, smoking is not allowed at all during the school day—whether students and staff are on or off school grounds. Experts believe that such a time-based rule is more effective. To support schools in implementing this stronger policy, the Smoke-Free Vocational Schools intervention was created. Our study explored how this policy was put into practice at seven vocational schools in Denmark. We looked at the factors—called “mechanisms”—that help schools succeed in making the policy part of everyday life. We gathered information from school staff through surveys, interviews, and group discussions. Staff members described how their understanding and practices changed as the new rules were introduced. Key factors included: (a) seeing the policy as meaningful and important, (b) feeling that schools have a responsibility to address smoking, (c) recognizing that the policy was legitimate and fair, (d) developing practical ways to enforce and communicate the rules, and (e) noticing positive impacts, such as less visible smoking on and around school grounds. Over time, schools became better at embedding the smoke-free school hours policy into their daily routines. The findings shed light on the “black box” of policy implementation—how rules move from paper into practice. These insights can guide other schools and policy makers who wish to create healthier, smoke-free environments for young people.
Keywords
Background
Smoke-free policies can protect people against tobacco use by reducing the availability, exposure, and acceptability of tobacco products (Loring, 2014) and are a key pillar in the WHO Framework Convention on Tobacco Control (Gravely et al., 2017). Considering that most individuals initiate smoking in adolescence (Reitsma et al., 2021), it is relevant to implement such policies in school settings. Yet, school tobacco policies (STPs) are often not implemented with sufficient fidelity, which may explain their limited effectiveness (Bast et al., 2015; Galanti et al., 2014; Jensen et al., 2024; Schreuders et al., 2017).
One issue with previous STPs is their design. Traditional STPs are location-based, prohibiting smoking only on school grounds but allowing students and staff to smoke just outside the premises. This makes it easy to bypass the rules by relocating smoking behavior to areas near the school, such as by the entrance, which still expose students to smoking (Leatherdale et al., 2005; Rozema, Mathijssen, Jansen, et al., 2018; Rozema, Mathijssen, van Oers, et al., 2018; Schreuders et al., 2017). To address these challenges, the more comprehensive smoke-free school hours policy extends the smoking ban to include the entire time spent at school. Several scholars have highlighted such comprehensive time-based policy designs as promising (Mélard et al., 2020; Miyazaki & Tabuchi, 2022; Piontek et al., 2008; Rozema et al., 2019; Schreuders et al., 2017).
As of August 2021, Denmark mandated smoke-free school hours for students under 18, including those in vocational schools. Vocational schools provide practical skills and knowledge for specific trades and professions, emphasizing hands-on learning and collaboration with industry. This policy focus is crucial because smoking rates are high among individuals with vocational education (de Looze et al., 2013; Klinker et al., 2020), and disparities in smoking rates are increasing (Willemsen et al., 2022). While the policy is promising, its effective implementation in Danish vocational schools remains a significant challenge.
The Smoke-Free Vocational Schools intervention was developed to support the implementation of smoke-free school hours into routine practice by testing implementation strategies, also called “activities” (Hjort, Christiansen, et al., 2021). The intervention took place during 2018–2020 across seven Danish vocational schools and lasted approximately 1 year per school (Hjort, Christiansen et al., 2021). The intervention activities, explained in detail in Supplementary Appendix 1 and elsewhere (Hjort, Christiansen, et al., 2021), built on a qualitative before-study on barriers to and facilitators for developing organizational readiness to implement the policy (Hjort, Schreuders, et al., 2021). Also, the activities mirrored general implementation strategies (Powell et al., 2015; Samdal & Rowling, 2015) and specific actions to support STP implementation (Schreuders et al., 2020).
In a previous study (Hjort et al., 2022), we examined associations between the intervention activities and implementation outcomes of the policy. Although we found positive associations between some activities and implementation outcomes, not all activities seemed to “work” as intended. For instance, none of the activities were associated with policy enforcement. More knowledge is needed to understand the implementation process, including how the activities/strategies produced implementation outcomes.
In this study, we applied the concept of implementation mechanisms to understand the functioning of the intervention. Implementation mechanisms are defined as processes through which an implementation strategy operates to affect desired implementation outcomes (Lewis et al., 2020). We combined the idea of implementation mechanisms with a realist evaluation philosophy, which depicts mechanisms as changes in human reasoning and behavior, influenced by a social program (e.g., implementation strategies) and the context (Pawson & Tilley, 1997). Also, the realist evaluation philosophy adds the notion of a program theory. In this study, the program theory constitutes key assumptions underlying the intervention, including the hypothesis that sufficient STP implementation outcomes will result in less smoking (Hjort, Christiansen et al., 2021). Our operationalization is shown in Figure 1.

Operationalization of Implementation Mechanisms in This Study.
Defining and testing implementation mechanisms is a novel inquiry in implementation science (Albers et al., 2020) and is highlighted on the research agenda to advance the field (Powell et al., 2019; Vejnoska et al., 2022). Specifically, studies that apply theory to measure and understand implementation mechanisms are wanted (Lewis et al., 2020; Vejnoska et al., 2022).
Concerning STPs, a realist review proposed mechanisms that explain students’ responses to different policy designs and their implementation (Schreuders et al., 2017). For instance, if the policy does not include clear rules with progressive sanctioning, students can experience the policy as unfair, making them alienated from the school and its anti-smoking messages (Schreuders et al., 2017). Another realist review identified mechanisms that determine enforcement by school staff (Linnansaari et al., 2019). These encompass (1) responsibility—believing that enforcement is a school role and duty, (2) motivation—believing that enforcement has a positive impact, and (3) confidence—possessing appropriate skills to deal with student responses to enforcement (Linnansaari et al., 2019). To the best of our knowledge, no studies have tested how the mechanisms can be triggered.
The Smoke-Free Vocational Schools intervention constitutes a unique opportunity to study the implementation of the promising smoke-free school hours policy. To fully understand how, why, and when the activities/strategies worked to leverage implementation, we must unravel the implementation mechanisms.
Aim
The overall objective of this study was to assess and understand the mechanisms that shaped policy implementation outcomes from the perspectives of staff and managers. This entailed three secondary aims: (1) to assess associations between mechanisms and implementation outcomes, (2) to understand the reasoning and behavior change that constitute mechanisms, and (3) to derive how intervention activities/strategies triggered mechanisms.
Method
Theoretical Framework
Normalization Process Theory (NPT) provides a framework for understanding the social processes that drive implementation in complex adaptive systems, such as schools (Keshavarz et al., 2010; May et al., 2016), and aligns with realistic evaluation (Dalkin et al., 2021). NPT identifies four generative mechanisms that facilitate implementation through individual and group actions: Coherence, Cognitive Participation, Collective Action, and Reflexive Monitoring (May & Finch, 2009). In this study, these mechanisms were operationalized as follows:
Coherence: the extent to which staff and managers find the smoke-free school hours policy meaningful and understand what its implementation requires (i.e., sense-making processes). Cognitive Participation: the engagement of staff and managers, their perception of policy legitimacy, and the identification of program champions (i.e., engagement and legitimation processes). Collective Action: the practical work and changes needed for policy implementation (i.e., enactment processes). Reflexive Monitoring: the formal and informal efforts to evaluate the value of the policy (i.e., appraisal processes).
We named these four proposed mechanisms normalization mechanisms. Additionally, we expanded NPT to include readiness mechanisms, specifically Change Commitment and Change Efficacy, which captured preparedness for future action (Weiner et al., 2020). Table 1 details our operationalization of readiness and normalization mechanisms. For simplicity, we refer to these as “mechanisms” throughout the manuscript, though the Results section further clarifies their roles as actual implementation mechanisms.
Operationalization of Mechanisms in the Study, Including the Qualitative Deductive Coding Strategy and the Quantitative Independent Variables.

Note. All independent variables were assessed on Likert scales from 1 to 5 by “Do you agree or disagree with following statement?”
Study Design
Mixed methods are recommended for examining implementation outcomes (Martinez et al., 2014) and the strategies, mechanisms, and contexts that influence them (Palinkas et al., 2011; Powell et al., 2019). We employed a convergent mixed-methods design, which involved the simultaneous collection and analysis of qualitative and quantitative data, with subsequent integration of findings (Fetters et al., 2013). An overview of the data and design is provided in Figure 2.

Convergent Mixed-Methods Design Applied in This Study.
The quantitative strand employed a repeated cross-sectional survey design at three time points across the seven intervention schools: pre-policy (T0), 5 months post-policy (T1), and 14 months post-policy (T2). The first survey (T0) was administered immediately after the activities but before the policy was put into force. Mechanisms were assessed at each time point, while implementation outcomes were measured at T1 and T2. For each survey, all employees at the schools were invited to participate, including both the same individuals over time and new individuals for each time point. Hence, the design is cross-sectional at T1 and T2, capturing both dependent and independent variables. As implementation outcomes could not be assessed at T0, this design approximates a longitudinal study by examining subsamples of individuals participating at T0 and followed up at T1 and T2, respectively. Reporting followed the STROBE checklist for cross-sectional studies (see Supplementary Appendix 2).
The qualitative strand involved semi-structured interviews and focus groups conducted within the same timeframe as the quantitative data collection, spanning from pre-policy to 14 months post-policy. Interviews were conducted with managers pre-policy and with project coordinators and staff post-policy. Reporting followed the Standards for Reporting Qualitative Research and Consolidated Criteria for Reporting Qualitative Research (see Supplementary Appendix 2).
The quantitative results assessed mechanisms and their associations with outcomes. The qualitative results enabled us to understand the reasoning that constituted mechanisms and their connections to intervention activities/strategies. The integration of results allowed us to better understand the pathways between implementation strategies, mechanisms, and outcomes.
Context and Intervention
In Denmark, vocational education and training is an upper-secondary education for specific trades or industries, combining school-based education with workplace training. There are over 100 vocational educations (e.g., carpenter, hairdresser, office assistant) grouped into four main subject areas. The average age of vocational school students is 24 (range: 15–65 years). The schools participating in the intervention represented all four vocational subject areas and three of the five geographical regions, representing both urban and rural parts of Denmark.
Two public health NGOs—the Danish Cancer Society and the Danish Heart Foundation—were responsible for recruiting schools and delivering intervention activities/strategies at the schools. As detailed in Supplementary Appendix 1, the intervention comprised 10 strategies conducted over 1 year per school. The first 6 months focused on stimulating organizational readiness for policy implementation. For example, the “joint workshop” for staff and managers was designed to create a shared understanding of the policy purpose. In the subsequent 6 months, once the policy was authorized, additional activities supported its integration into routine practice. For example, the introduction of new social school-break facilities aimed to reduce the appeal of social smoking.
The intervention project was reported to the Capital Region of Denmark's Legal Center, reference number: VD-2018-485. Given that the intervention was not a clinical trial, no further ethical approval was needed according to Danish legislation.
Data Collection and Participants
All data collection was carried out between 2018 and 2022. The qualitative data were nested as subsets within a larger quantitative sample, which ensured that it was possible and appropriate to merge qualitative and quantitative results (Collins et al., 2007).
Quantitative Study Population
We collected information on mechanisms and implementation outcomes using electronic surveys. All staff and managers from the participating schools were eligible to participate. The surveys were distributed to all school staff/managers using the school's mailing list. They received written information about the study scope, voluntariness, and processing of personal data. All participants consented before entering the survey.
Figure 2 presents an overview of the study population and response rates at each time point. At T1, the sample consisted of n = 419 respondents; at T2, it included n = 452. While 556 individuals participated in T0, only those who completed either T1 or T2 questionnaires were included in the analysis. The sample sizes for the T0–T1 and T0–T2 intervals were n = 209 and n = 182, respectively. Respondents with missing data on any outcome variables were excluded from the analysis. Variations in the number of participants across analyses were due to missing values on independent variables, including mechanisms and confounders, as detailed in Supplementary Appendix 3.
Qualitative Study Population
We employed individual and focus group interviews. Individual interviews were conducted with one manager and one/two project coordinators per school. The manager was responsible for overall school operations and development, while the project coordinator—appointed by the manager—oversaw STP implementation. Gathering knowledge from both roles was crucial and best obtained through one-on-one interactions. Focus groups with school staff allowed us to explore collective perspectives and organizational discourses (Creswell & Poth, 2018).
Management interviews were conducted before the policy was implemented to understand their perspectives on readiness and preparatory activities, including their expectations and strategic planning. In contrast, data from staff and project coordinators were gathered after the policy was put into force to capture their experiences with actual policy implementation, enforcement practices, and operational challenges.
School managers and project coordinators were recruited by a purposive sampling strategy. Both had in-depth knowledge regarding the implementation of smoke-free school hours. Staff were recruited randomly by a convenience sampling strategy. That is, through the survey at T1. The selection criterion was that their main professional task involved students (e.g., teacher or counselor). This further improved our mixed-methods sampling strategy, as we connected the quantitative and qualitative databases (Fetters et al., 2013).
All interviews and focus groups (n = 23) were moderated by A.V.H., who has extensive knowledge regarding the intervention and is trained in qualitative methods. Around half (n = 13) of the interviews or focus groups took place at the respective schools, while the remaining (n = 10) were conducted online, using Microsoft Teams. We found that online and physically conducted interviews had similar sufficient quality (Janghorban et al., 2014).
Interviews with managers averaged 58 min (range: 54–66), project coordinator interviews averaged 108 min (range: 80–143), and staff focus groups averaged 115 min (range: 109–121). Before participating in interviews, the participants signed informed consent. All data were audio-recorded and transcribed verbatim.
Altogether, n = 40 individuals participated in the interviews or the focus groups, as shown in Figure 2. On average, three individuals participated in the focus groups (range: 2–4).
Variables and Interview Guides
Variables
The independent variables were derived from the validated Normalization MeAsure Development (NoMAD) scales (Finch et al., 2018; Rapley et al., 2018), which measure the four constructs of NPT: Coherence, Cognitive Participation, Collective Action, and Reflexive Monitoring. Designed to evaluate implementation mechanisms from a professional perspective, the NoMAD scales can be adapted for specific contexts by modifying item selection and wording (Finch et al., 2018; Rapley et al., 2018).
In this study, we adapted the NoMAD scales as outlined in Table 1. Specifically, at T1 and T2, we assessed the normalization mechanisms of Coherence, Cognitive Participation, Collective Action, and Reflexive Monitoring. At T0, prior to policy implementation, we measured readiness mechanisms—Change Commitment and Change Efficacy—inspired by the organizational readiness concept (Weiner, 2009) and the NoMAD scales.
The NoMAD allows flexible scoring by averaging items within each construct for comparisons across constructs, groups, or sites. Constructs are measured on 5-point Likert scales, where higher values indicate more effective implementation processes. Each scale in this study was analyzed as the mean of its items.
The implementation outcome measures were defined as four domains: (1) adherence: familiarity with policy entailments, (2) dose: exposure to smoking during school hours, (3) quality of delivery: enforcement of policy, and (4) participant responsiveness: sense of policy implementation (Hjort et al., 2022). Together, the domains reflect whether the STP was integrated into routine practice (Hjort et al., 2022). We coded the domains into binary variables (implemented = 1 or not = 0) and calculated a total implementation score by the sum (range: 0–4). The operationalization is discussed elsewhere (Hjort et al., 2022).
As confounders, we included age, sex, smoking status, and whether staff/managers had a special function concerning health promotion.
All dependent variables, as well as confounders, are detailed in Supplementary Appendix 4.
Interview Guides
The interviews with managers focused on efforts and intervention activities to prepare for policy implementation. The interviews with project coordinators and staff focused on their everyday practices to enforce the policy as well as appraisals of past efforts and intervention activities. To strengthen the mixed-methods integration, we included questions from the quantitative operationalization of mechanisms, where the participant(s) were asked to reflect on items. For example, when asked “are there key people at this school who drive the implementation forward?” the participant(s) elaborated on who and how they drove the implementation forward. Examples of interview guides are available in Supplementary Appendix 5.
Data Analysis
Statistical Analysis
Given the modifications to the NoMAD scales, we conducted validity and reliability assessments. To evaluate validity, we employed confirmatory factor analysis (CFA). Separate CFA models were estimated for the four normalization mechanisms (Coherence, Cognitive Participation, Collective Action, and Reflexive Monitoring) and the two readiness mechanisms (Change Commitment and Change Efficacy). Model fit was considered acceptable if the root-mean-square error of approximation (RMSEA) was below 0.08 (Rigdon, 1996; Xia & Yang, 2019). For reliability, we calculated Cronbach's alpha (α) and omega hierarchical (ωh). The latter is recommended for multi-dimensional factor structures and Likert-scale data (Flora, 2020). For both α and ωh, we aimed for values greater than .7.
Both validity and reliability assessments were performed separately for each time point. Readiness mechanisms were evaluated using data from T0 to T1 and T0 to T2, while normalization mechanisms were assessed at T1 and T2. Mechanisms were analyzed with separate CFAs due to the cross-sectional design.
To examine potential differences in implementation outcomes and mechanisms among schools, we conducted descriptive statistical analyses. Generalized linear models (GLMs) were employed to explore the relationships between mechanisms and outcomes. Logistic regression was used for analyzing binary outcome measures, while linear regression was applied to the continuous implementation outcomes. To account for the clustered data structure inherent in the school settings (Eldridge et al., 2009), “school” was included as a covariate in all models. We estimated both univariate models, which accounted solely for school clustering, and multivariate models, which were adjusted for all identified confounders.
Due to the repeated cross-sectional design, associations were analyzed separately for each time point. Associations between normalization mechanisms and implementation outcomes were assessed using data from T1 and T2, respectively. In the T0–T1 and T0–T2 analyses, readiness mechanisms were considered independent variables at T0, while implementation outcomes were dependent variables at T1 and T2, respectively. This approach allowed us to examine the impact of baseline readiness mechanisms on subsequent outcomes.
All statistical analyses were conducted in R.
Qualitative Coding and Analysis
The coding and analysis process followed four steps—shown in Table 2. This process was guided by Braun and Clarke's reflexive thematic analysis (TA) (Braun & Clarke, 2006, 2021), which is adaptable to various theoretical perspectives.
The Steps of the Qualitative Analysis Process.

Integrated Data Analysis
The integrated analysis intended to provide meta-inferences, that is, a third viewpoint based on both qualitative and quantitative results (Fetters & Freshwater, 2015). Specifically, we aimed to (1) establish whether the proposed mechanisms were in fact mechanisms, namely, related to both activities and implementation outcomes and (2) better understand the mechanisms by merging qualitative and quantitative results.
The first aim entailed that qualitative and quantitative findings complemented each other. The quantitative findings established whether mechanisms were associated with implementation outcomes, whereas the qualitative findings explored links between intervention activities and mechanisms.
The second aim involved merging results. As recommended, we applied theory (Creswell & Plano Clark, 2018) and side-by-side joint displays (Fetters & Freshwater, 2015). Through the joint display analyses, we identified if and how results from each strand confirmed, disconfirmed, or expanded our understanding of mechanisms. Furthermore, the analysis was iterative in that we followed up on confirming and disconfirming evidence. Namely, we used raw item values/answers to interview questions to shed new light on interesting phenomena. For example, an emphasis on legitimacy in the qualitative analysis redirected us to the quantitative data that included a specific variable on legitimacy. Likewise, a quantitative finding of insufficient time/resources redirected us to the qualitative transcripts to interpret why this was problematic. As for presentation, we included visuals for the quantitative results, which have been recommended in recent joint display literature (Guetterman et al., 2021).
Results
The results are presented in three parts. First, we summarize the quantitative analysis and then the qualitative analysis of mechanisms. Third, we present the joint display analysis to elaborate on the mechanisms and their associations with implementation. The qualitative analysis of links between intervention activities and mechanisms is included in Supplementary Appendix 6.
Quantitative Results
The mean ages of staff and managers varied between 47 and 49 at the various time points. Around 65% of the respondents were teaching staff, while the remaining were managers, counselors, or administrative or service personnel. The total smoking prevalence, defined as daily and occasional smoking, was between 12% and 13% at all time points. A detailed overview of characteristics is available in Supplementary Appendix 7.
The CFA yielded RMSEA values from 0.072 to 0.074 across all analyses. The alpha (α) for “Cognitive Participation” was relatively low at approximately .64, while the remaining scales demonstrated sufficient internal consistency, around .80. Likewise, omega hierarchical (ωh) exceeded the desired threshold of .7 for most subfactors, except for cognitive participation (e.g., ωh = .46 at T1). Thus, the structural validity and reliability of the mechanism scales were acceptable.
Descriptive results of the mechanisms (independent variables) and implementation outcomes (dependent variables) are shown in Table 3. Both the mechanisms and total implementation differed significantly between schools (p < .001). Additionally, the total implementation score increased from T1 (2.80) to T2 (2.92). Results stratified by intervention schools are available in Supplementary Appendix 8.
Descriptive Statistics Regarding Mechanisms (Independent Variables) and Implementation Outcomes (Dependent Variables).

Note. All mechanisms were assessed on Likert scales from 1 to 5. Implementation outcomes were coded into binary variables (1 = implemented and 0 = not); the table includes the percentages of “implemented.”
aT0 + T1 and T0 + T2 refer to the subgroups of individuals who participated both at T0 and T1 or both at T0 and T2, respectively. bTotal implementation constitutes a score across the four binary implementation domains.
All normalization mechanisms were consistently associated with both the total implementation score and Participant Responsiveness, for example, odds ratio (ORs) between 2.6 and 4.9 for Participant Responsiveness. The analysis of readiness mechanisms also yielded consistent associations with the total implementation score. None of the normalization mechanisms were associated with Quality of Delivery (policy enforcement). In contrast, the readiness mechanisms were associated with Quality of Delivery at both time points. The results, adjusted for all confounders, are shown in the joint displays (Figures 3–6) and are also available in Supplementary Appendix 9. The crude results are available in Supplementary Appendix 10.
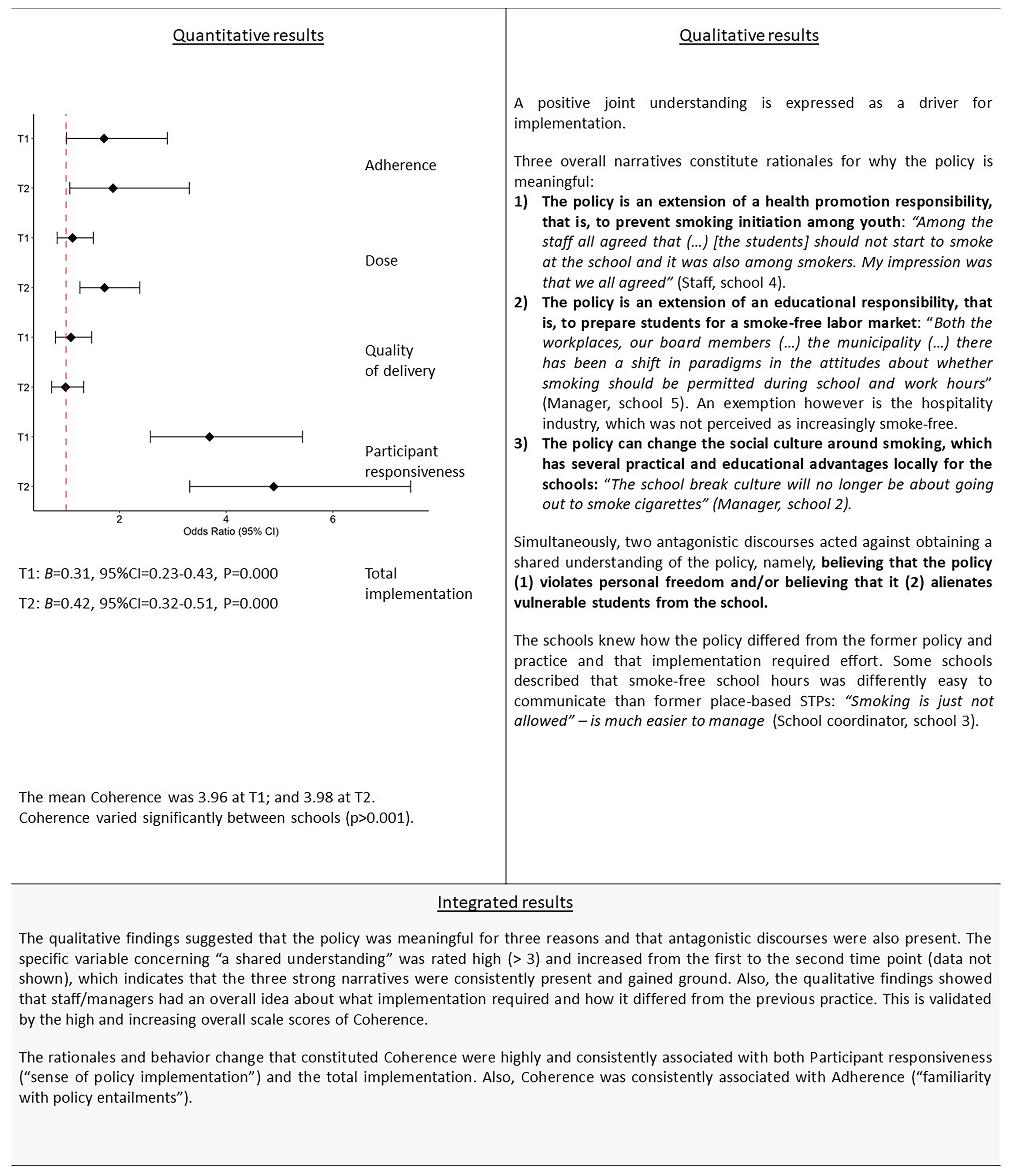
Coherence—Joint Display Integrated Results.

Cognitive Participation—Joint Display Integrated Results.

Collective Action—Joint Display Integrated Results.

Reflexive Monitoring—Joint Display Integrated Results.
Qualitative Results
The key reasoning and behavioral changes that constituted normalization mechanisms are summarized below in Table 4. We were unable to qualitatively distinguish readiness from normalization mechanisms. Therefore, we only included an analysis of normalization mechanisms.
Summary of Qualitative Analysis, That Is, Key Reasoning and Behavior Change That Constitutes Normalization Mechanisms.

Integrated Results
The integrated results for each normalization mechanism are presented in the joint displays (Figures 3–6).
The joint display analyses enhanced our understanding of the mechanisms, with qualitative results revealing specific patterns of reasoning and quantitative results confirming their association with policy implementation. While we could not qualitatively distinguish readiness mechanisms from normalization mechanisms, perceptions of preparedness were noted under Reflexive Monitoring (Figure 6). Consequently, joint displays for Change Commitment and Change Efficacy were not included. The quantitative results are available in the Supplementary Appendixes.
Discussion
Key Findings
This study aimed to elucidate the mechanisms influencing STP policy implementation outcomes from the perspectives of staff and managers. Our findings confirm that the proposed mechanisms are indeed implementation mechanisms, that is, they are associated with both implementation strategies and outcomes. The key findings related to our three aims are summarized in Table 5.
Summary of Key Findings—in Relation to the Aims of This Study.

Interpretation of Results
This study is one of the first intervention-based research to provide evidence on the mechanisms underlying STP implementation, pioneering by linking them to implementation strategies and outcomes. While previous studies have identified similar processes involved in STP implementation (Danielsen et al., 2023; Hjort, Schreuders, et al., 2021; Linnansaari et al., 2019, 2022; Rozema, Mathijssen, van Oers et al., 2018; Schreuders et al., 2020), this research uniquely examined the causal pathways of implementation. As one of the first hypothesis-testing studies in this area, it contributes to both the literature on STP implementation—particularly concerning the promising smoke-free school hours policy—and to the emerging research on implementation mechanisms (Lewis et al., 2020; Vejnoska et al., 2022).
In our previous research, we found positive associations between three specific intervention activities and total implementation score: the joint workshop, established enforcement procedures, and new school-break facilities (Hjort et al., 2022). The analysis of mechanisms in this study suggests that the intervention activities likely activated the identified implementation mechanisms. Consequently, this study posits that these mechanisms were the drivers for implementation.
This study observed an increase in the total implementation score from the initial to the subsequent measurement point, indicating that schools progressively integrated smoke-free policies into their daily practices. This is consistent with the strong associations between implementation mechanisms and the total implementation score, underscoring the effectiveness of these mechanisms in promoting policy implementation. These findings are noteworthy given the limited evidence on effective ways to improve tobacco control implementation in school settings (Wolfenden et al., 2022).
A notable finding was the variability in implementation mechanisms and outcomes across schools, indicating that local contexts and school environments significantly influence policy implementation. Based on qualitative data collected as part of the study (not included in the present analysis), contextual factors such as leadership transitions and institutional mergers at Schools 1 and 5 likely contributed to less favorable conditions for implementing smoke-free school hours. These contextual dynamics may help explain the generally lower values observed for mechanisms and outcomes at these sites (Supplementary Appendix 8). While these interpretations remain tentative, they highlight the potential importance of contextual determinants. This underscores a critical aspect of implementation strategies: their success depends on triggering mechanisms within specific contexts (Pawson & Tilley, 1997). Furthermore, it reaffirms the importance of context when implementing STPs, consistent with recent Danish studies in this area (Danielsen et al., 2023; Jensen, Krølner, Jørgensen, et al., 2023; Jensen, Krølner, Thygesen, et al., 2024).
Our study also highlighted the influence of societal norms on local implementation processes. Specifically, the perception of smoke-free norms was perceived as facilitating the gradual implementation of smoke-free school hours into routine practice. This suggests a bidirectional relationship in which STP implementation can both influence and be influenced by societal norms. This connection has also been demonstrated in previous research on STPs (Linnansaari et al., 2022; Rozema et al., 2016; SILNE-R Consortium et al., 2019).
Differentiating between readiness and normalization mechanisms proved challenging in this study. We believe this is due to their interconnectedness. For instance, our qualitative analysis highlighted the importance of preparing for change, yet this was classified under Reflexive Monitoring. Similarly, a recent qualitative study in Danish vocational schools on readiness to implement smoke-free school hours identified empirical content similar to what we categorized as normalization mechanisms (Hjort, Schreuders, et al., 2021). This overlap suggests that the empirical content of the concepts is closely related.
The lack of consensus on organizational readiness (Weiner et al., 2020) further complicates its distinction from normalization mechanisms. While readiness is commonly understood as preparedness for future action (Weiner et al., 2020), some scholars highlight its relevance also during change processes (Scaccia et al., 2015). Thus, readiness can be interpreted in various ways, some of which overlap with (what we call) normalization mechanisms. In this study, we defined readiness as preparedness for future action (Weiner et al., 2020), measuring it only pre-policy, and categorized post-policy mechanisms as normalization mechanisms—using NPT-based scales for both. Consequently, we suggest that readiness and normalization mechanisms share similar content and function synergistically to enhance STP implementation, with timing as the key differentiator.
Despite this empirical overlap, our quantitative analysis revealed a distinct impact of readiness on implementation outcomes. Specifically, readiness mechanisms were the only mechanisms associated with policy enforcement. These findings suggest that fostering organizational readiness before implementing an STP is critical, even if the empirical content of these mechanisms may be similar to those that operate after the policy is put into force. This is further supported by our qualitative analysis of Reflexive Monitoring, which found that the preparation phase—activities conducted before the policy was put into force—was crucial for successful policy implementation.
Strengths and Limitations
This study employed a repeated cross-sectional design for the quantitative strand. We measured implementation mechanisms at three distinct time points, as these mechanisms were expected to evolve throughout the implementation process rather than occurring solely immediately after the intervention (Hjort, Christiansen, et al., 2021). While longitudinal approaches are ideal for tracking individual behaviors over time (e.g., smoking behavior), cross-sectional designs might be equally robust for evaluating STP implementation (e.g., smoking visibility). We chose a cross-sectional design to maximize participant inclusion, as the analyses from T0 to T1 and T0 to T2 (with around 200 participants) showed that a longitudinal design would have significantly reduced the sample size. We recognize that combining both approaches would have been ideal. However, considering the scope of data and analyses already included in the study, we focused only on the cross-sectional analysis.
To ensure the internal validity of the cross-sectional design, we sought to (1) minimize selection bias and (2) control for key confounders (Mann, 2003; Smith & Noble, 2014). We did not expect selection bias among staff and managers, and consistent response rates across time points indicated that attrition was not an issue. Concerning confounders, we included the most obvious (e.g., smoking status); however, we could not account for all factors that could influence mechanisms and policy implementation. For example, due to the small number of schools, we could not include school-level variables (e.g., school size).
A study strength is the use of validated scales to assess mechanisms and additional psychometric tests for reliability and validity, with the repeated measurement design indirectly confirming test–retest reliability. This design also allowed us to prove consistent associations, reducing the likelihood that findings were due to chance (Mann, 2003). However, a key limitation of the cross-sectional design is its inability to establish causality, which carries an inherent risk of reverse causation.
In the qualitative strand, the NPT framework was employed for both the development of interview guides and the analysis, ensuring consistency throughout. Transparency in the operationalization of interview guides, coding, and use of reporting guidelines further enhanced the congruence in how results were generated. Although NPT provided strong conceptual guidance, distinguishing between mechanisms proved difficult at times, consistent with earlier findings (McEvoy et al., 2014). This reflects the inherent interdependence of the constructs (May & Finch, 2009).
Our approach was informed by Braun and Clarke's six-step TA framework (Braun & Clarke, 2021), which we adapted into a four-step process tailored to the needs of our study. A case-based analysis of the implementation process at each school could have provided deeper insights into variations in implementation. However, we opted for a cross-cutting TA approach due to the extensive data analysis already included in the paper.
Additionally, a qualitative analysis of the intervention as a whole would have been ideal since its overall impact is expected to be more significant than that of individual intervention activities. However, this was not feasible. Moreover, our difficulty in distinguishing between normalization and readiness mechanisms may reflect limitations in our coding framework.
Our qualitative sampling strategy did not explicitly aim for data saturation, which is a recognized limitation (Smith & Noble, 2014). Nonetheless, the large number of interview participants suggests that data saturation was likely achieved.
The strengths of the mixed-methods approach include consistency in (1) design, (2) sampling, and (3) integration of results, which we achieved through a theoretical framework and nested sampling strategy. This integration was crucial for identifying implementation mechanisms. However, an inherent challenge of such design is balancing the depth of qualitative and quantitative findings, which may limit the exploration of (especially) qualitative nuances.
Implications for Practice
This study provides evidence of strategies that enhance the implementation of smoke-free school hours, which can be considered by practitioners seeking to implement comprehensive STPs.
Key implementation strategies include (1) the joint workshop for staff and managers and (2) new school-break facilities.
The joint workshop fostered Coherence by clarifying the reasons for policy adoption and promoting a shared understanding. Additionally, the workshop highlighted concerns about enforcement and the need for clearer rules and responsibilities. Both align with cross-European research on STP implementation (Schreuders et al., 2020). Thus, conducting such workshops for staff before the STP is put into force can serve as a beneficial implementation strategy.
The new school-break facilities fostered Collective Action and entailed the creation of appealing social environments (to replace social smoking). This approach is consistent with strategies that have been effective in reducing occasional smoking in Danish vocational schools (Andersen et al., 2016) and are reflected in the successful Icelandic Prevention Model (Sigfusdottir et al., 2020). Hence, structural and pedagogical initiatives to diminish social smoking might be an effective implementation strategy.
Additionally, the study identified several critical actions needed to implement smoke-free school hours: (1) establishing clear rules and responsibilities; (2) assisting students in adapting to smoking restrictions; (3) ongoing dialogue about the policy; and (4) demonstrating commitment to the policy through leadership and allocating necessary resources. These actions align with recent STP research highlighting the importance of effective change management (Danielsen et al., 2023).
The findings are pertinent to states and institutions aiming to implement comprehensive STPs. The strategies are particularly applicable to vocational schools or similar educational settings, both nationally and internationally, where the student smoking prevalence is high and perceived as problematic.
Implications for Research
This research provides a methodological framework for understanding and investigating implementation mechanisms through a mixed-methods approach, contributing to the emerging literature in this field (Albers et al., 2020; Lewis et al., 2020; Powell et al., 2019). The development of a novel survey for assessing readiness, utilizing NPT/the NoMad scales, adds to the methodological contributions of this study. Future research should build on these methodological innovations by exploring their application in other settings and interventions.
This study highlights the significance of the preparatory phase—building readiness—for the successful implementation of smoke-free school hours. Further research should explore readiness mechanisms in more depth to determine if there is a threshold at which schools are sufficiently prepared to implement comprehensive STPs (Hjort, Schreuders, et al., 2021; Weiner et al., 2020).
Additionally, future studies should investigate how contextual factors impact variations in implementation outcomes and develop strategies to address these factors, emphasizing the need to tailor implementation strategies to specific contexts. For instance, it might be relevant to explore change management practices concerning STPs (Danielsen et al., 2023).
Additionally, we anticipate evaluating the effectiveness—that is, smoking-related outcomes—associated with the implementation of smoke-free school hours. Future research should also examine the potential unintended consequences of STP implementation, such as the stigmatization of individuals who smoke, as discussed in recent Danish research (Glenstrup et al., 2021).
Conclusion
This study elucidated the interplay between implementation mechanisms and strategies in achieving implementation outcomes for the smoke-free school hours policy within Danish vocational schools. We identified key mechanisms that consistently and significantly influenced implementation outcomes and highlighted strategies that triggered these mechanisms. These findings deepen our understanding of STP implementation and provide actionable recommendations for enhancing STP implementation. Additionally, the study introduces methodological innovations for investigating implementation mechanisms.
Supplemental Material
sj-docx-1-irp-10.1177_26334895251377658 - Supplemental material for Unraveling the “black box” of school tobacco policy implementation: A mixed-methods study at Danish vocational schools informed by Normalization Process Theory
Supplemental material, sj-docx-1-irp-10.1177_26334895251377658 for Unraveling the “black box” of school tobacco policy implementation: A mixed-methods study at Danish vocational schools informed by Normalization Process Theory by Anneke Vang Hjort, Charlotte Demant Klinker, Mirte A.G. Kuipers, Charlotta Pisinger and Tine Tjørnhøj-Thomsen in Implementation Research and Practice
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Danish Health Authority.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.