
Abstract
Background:
Adaptation is an accepted part of implementing evidence-based practices. COVID-19 presented a unique opportunity to examine adaptation in evolving contexts. Delivering service to people with opioid use disorder during the pandemic required significant adaptation due to revised regulations and limited service access. This report evaluated changes to addiction medication services caused by the pandemic, challenges encountered in rapidly adapting service delivery, and initial impressions of which changes might be sustainable over time.
Methods:
Qualitatively-evaluated structured interviews (N = 20) were conducted in late 2020 with key informants in Pinellas County (FL) to assess the pandemic’s impact. Interviewees represented a cross-section of the professional groups including direct SUD/HIV service providers, and sheriff’s office, Department of Health, and regional clinical program administrative staff. The interview questions examined significant changes necessitated by the pandemic, challenges encountered in adapting to this evolving context, and considerations for sustained change.
Results:
The most significant changes to service delivery identified were rapid adaptation to a telehealth format, and modifying service consistent with SAMHSA guidance, to allow for ‘take-home’ doses of methadone. Limitations imposed by access to technology, and the retraining of staff and patients to give and receive service differently were the most common themes identified as challenging adaptation efforts. Respondents saw shifts towards telehealth as most likely to being sustained.
Conclusions:
COVID-19 provided an unprecedented opportunity to examine adaptation in a fast-paced, dynamic, and evolving context. Adaptations identified will only be sustained through multisystem collaboration and validation. Results suggest that additional components could be added to implementation frameworks to assess rapid adaptation during unplanned events, such as access to additional resources or local decision-making that impacts service delivery. Findings will also be integrated with quantitative data to help inform local policy decisions.
Plain Language Summary:
Adaptation is an accepted part of implementing evidencebased practices. COVID-19 presented a unique opportunity to examine rapid adaptation necessitated within evolving contexts. Delivering services to people with opioid use disorder required significant adaptation due to changing regulations and limited access to lifesaving services. This study examined changes in service delivery due to the pandemic, challenges encountered in rapid adaptation, and initial impressions of which changes might be sustainable over time. Qualitatively-evaluated structured interviews were conducted with a cross-section of professional groups (direct substance use disorder (SUD) and human immunodeficiency virus (HIV) service providers, and sheriff's office, Department of Health, and clinical program administrative staff) in Pinellas County (FL). The most significant changes to service delivery were rapid adaptation to a telehealth format and increased allowance for 'takehome' doses of methadone medication. Limitations imposed by access to technology, as well as the education of and staff and patients were the most common themes identified as challenges. Respondents saw shifts towards telehealth as most likely to be sustained. COVID-19 provided an unprecedented opportunity to examine adaptation in a fast-paced, dynamic, and evolving context. Adaptations will only be sustained through multisystem collaboration and validation. Findings suggest that additional components could be added to implementation frameworks to assess rapid adaptation during unplanned events, such as access to additional resources or local decision-making that impacts service delivery.
Introduction
Adaptation is an inevitable part of implementing evidence-based treatment and may refer to changes to the treatment or the way it is delivered, organizational changes, and changes made to the strategies that support the implementation process (Aarons et al., 2019; Escoffery et al., 2018; Lengnick-Hall et al., 2020; Miller et al., 2021). In implementation science, adaptation is typically treated as a process that should be systematic, planned, and rigorous (Kirk et al., 2020; von Thiele Schwarz et al., 2019; Wiltsey Stirman et al., 2019; Miller et al. 2021). COVID-19 presented a unique opportunity to examine what adaptation looks like when decisions have to be made quickly, with less guidance, and with incomplete and evolving information. The research question guiding this brief report is: how did one community (Pinellas County, FL) rapidly adapt to maintain access to and delivery of evidence-based treatment to individuals with opioid use disorders (OUDs) during the COVID-19 pandemic?
Adaptation was different during the pandemic for several reasons. First, the pandemic removed structural barriers that previously constrained decisions, for example, new reimbursement options for virtual care (Beidas & Wiltsey Stirman, 2021; Chambers, 2020). Second, the evidence-base around COVID-19 interventions often came out faster than researchers could assess it and may not apply locally, e.g. differences in infection rates and limited availability of medical resources across sites (Wensing et al., 2020). Third, leaders were willing to try new things and make “radical decisions” in a way that they might not normally do during non-pandemic times (Wensing et al., 2020). Fourth, patient populations who were already marginalized were also hit harder by the pandemic. Relevant to our study, individuals experienced an increase in new symptoms, relapse to patterns of addictive behaviors, increased difficulty accessing services, increased withdrawal emergencies, worse COVID-related outcomes due to compromised lung functioning, and death (Liese & Monley, 2021; Volkow, 2020). Furthermore, adaptation decisions had to be made in light of the fact that any change in service delivery could pose a significant risk for persons with a pattern of illicit opioid use, who often move in and out of care, and are especially at risk for overdose, exacerbated by, in the current moment, by changing mixtures of drugs which are of increased lethality (Volkow & Blanco, 2021).
This investigation is one component of a multi-part project developing agent-based models to support decision making (Vermeer et al., 2020) to reduce opioid-related deaths. Qualitative interviews with community professionals were conducted to assess the impact of COVID-19 on access to care for persons with opioid use histories. This report focuses on the qualitative evaluation of these structured interviews related to 1) the most significant changes to service delivery for persons with opioid use disorders as a result of the pandemic, 2) challenges encountered in rapidly adapting service delivery in this unprecedented context which severely limited access to in-person care, and 3) initial impressions as to what changes in service delivery may be sustainable over time.
Methods
Participants
Between November 16, 2020 and January 11, 2021, structured interviews were conducted with community stakeholders who represented agencies and programs involved in the Pinellas County (FL) Opioid Task Force. The Task Force was formed in 2017 to address the ‘skyrocketing trend’ of opioid overdoses in the County and is co-led by leaders in the Florida Department of Health in Pinellas County and Operation PAR, a comprehensive behavioral health service provider (https://www.tampabay.com/news/health /2019/09/28). Participants were identified through their direct association with the Task Force, or were nominated by members in participating agencies (including the Department of Health-PC, the Pinellas County Sheriff’s office, substance use and HIV service providers and administrators, representatives of homeless services, and regional MH/SA program administrators). A goal was set to complete 20 interviews which is greater than the number typically required (12–15) to achieve saturation in responses (Guest, Bunce, & Johnson, 2006). Saturation, across a diversity of professional perspectives, was assessed as having been achieved from this 20 person sample.
Procedures
Interviews were initially scheduled through email with those nominated by community / Task Force members. Of 24 individuals invited to participate, 20 (83%) scheduled telephone interviews. Structured interviews were conducted by a PhD level clinical researcher (1st author) with experience in qualitative methods, criminal justice and health policy, and community-based substance use treatment. Questions evaluated as a part of this analysis (a subset of a longer interview) included 1) From your perspective, what has been the most significant change to service delivery for persons with opioid use disorders, during the pandemic? 2) What (additional) clinical practices, relative to medication-assisted treatment (MAT), have significantly changed due to the pandemic? 3) What challenges have occurred in attempting to implement any forms of practice change? 4) Of any of the service changes that have been implemented or modified, which do you believe will be sustained? Participants often offered multiple responses to a single inquiry; all were scored. Response rates (listed below), therefore, sum to greater than 100%.
Each interview lasted 35–55 min (19 questions) and were audio recorded and transcribed. Subjects gave their consent to participate following their consideration of a verbally-presented informed consent, approved by the 1st author’s Institutional Review Board; they received no compensation for their participation.
Analyses
Responses to the four interview questions were independently reviewed and evaluated by the 1st and 2nd authors and dominant response themes were identified. Following theme generation, all 20 interviews were reviewed and the themes associated with each subject’s responses were identified and rated by the two researchers. Across themes and responses, coding demonstrated 88–92% interrater agreement among the questions explored.
Results
Participants represented diverse professional perspectives involved in addressing opioid use and overdose deaths, including direct addiction treatment service providers, clinical administrators, criminal justice and county staff members; the sample included 65% female and 35% male respondents. Demographically, the sample respondents were 60% Caucasian, 20% Hispanic, 10% Black, 5% Asian, and 5% Other. A majority (85%) were between 36 and 70 years of age.
Q1: most significant change to service delivery
Dominant theme 1: transfer to telemedicine
A majority of respondents (60%) viewed the transition to telemedicine as the most significant change to service delivery resulting from the pandemic. Most described the scope of the change as being daunting. While some programs had experience with the use of telehealth, others were un- or under-prepared. Sample responses can be found in Table 1.
Most significant change to service delivery: dominant themes.

Dominant theme 2: eligibility for ‘take-homes’
Under emergency guidance offered by SAMHSA, who oversees opioid treatment programs (OTPs), persons in care could be offered ‘take-home’ medication to take unobserved, offsite without having to meet the length in treatment / other criteria usually imposed. This option was viewed as ‘most significant’ by 45% of interviewees, and was considered very positive by most; however, some clinicians voiced concerns over relaxing this rule. Sample responses can be found in Table 1.
Additional themes: loss of contact with clinicians, service disruptions
Respondents also voiced an array of COVID related changes that were significant and impactful. These included moving away from face-to-face service delivery, changing methods of service delivery so quickly with large patient populations, as well as the rapid implementation of infection control procedures. Sample response can be found in Table 1.
Q2: challenges in rapidly adapting service delivery
Dominant theme 1: retraining staff and patients
The most frequent response, offered by 40% of interviewees, related to training staff and patients in how to execute services in a new way and how challenging it proved to be. Others discussed encountering resistance, with clinicians having to overcome the impulse to revert to ‘old habits’ (no social distancing, not masking correctly). Sample responses are found in Table 2.
Challenges of rapid adaptation: dominant themes.
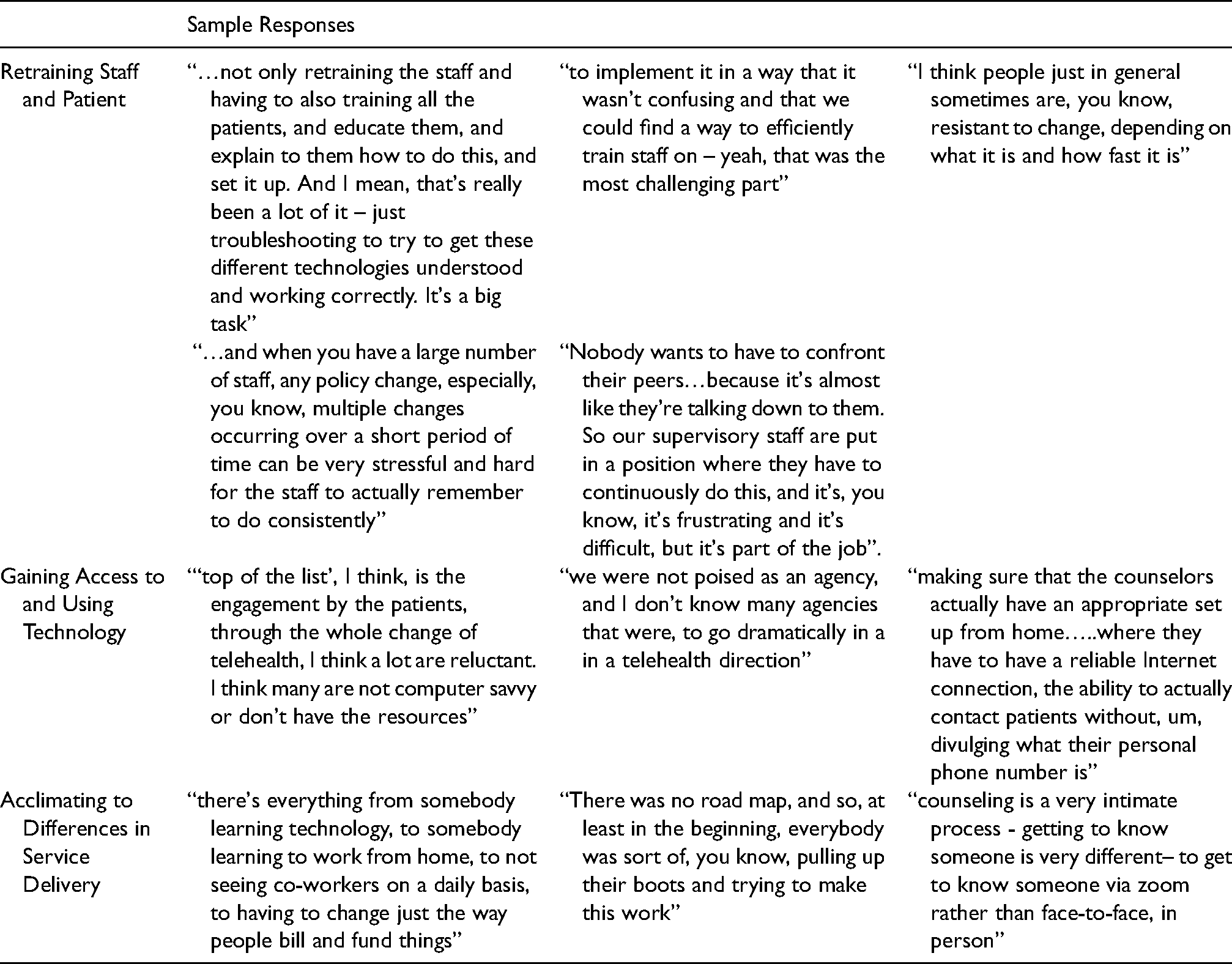
Dominant theme 2: gaining access to technology, negotiating remote Set-up, finding private spaces
Challenges in access to appropriate technology for both staff and patients was often reported. Shifting to remote work was also challenging; examples of this included having the right setting to ensure confidentiality and adequate and reliable internet access. Sample responses are found in Table 2.
Dominant theme 3: acclimating to differences in service delivery
Challenges existed in all forms of work life experience being disrupted, with only limited opportunities for instruction in the rapid adaptation to other service formats. Sample responses are in Table 2. Another theme involved having adequate and available channels of communication. Respondents reflected on how frequently they had to meet to revise methods when an initial strategy did not achieve desired results. The challenge of maintaining quality of care was also emphasized, with new methods of supervision having to be developed rapidly to fit into the telehealth format.
Q3: prospective views on sustained changes
Dominant theme 1: continuing / expanding telehealth
Most respondents (60%) expected shifts in the use of telehealth to be sustained, likely in video format. The extent of the continued adoption remained unclear, with respondents acknowledging that expanded access to technology and related funding would drive any sustained change. Sample responses are in Table 3.
Prospective views on sustained changes: dominant themes.

Dominant theme 2: expanded Use of take-homes, if allowed through regulatory changes
The second most common theme, expressed by 30% of respondents, was their hope that greater flexibility in methadone dosing could be maintained, so as to reduce an array of barriers to care, including transportation and child care challenges. Some expressed concern that reversals in policy, if they occur, would not be well received, especially if the individual had experienced no adverse effects.
Dominant theme 3: Use of infection control processes
Some respondents (30%) commented on sustaining infection control procedures. They acknowledged that the closeness of contact and volume of patients served in OTP programs make these changes a now-obvious choice. Sample responses are in Table 3. Additionally, interviewees were asked about how they had heard about systemic or programmatic changes necessitated by the pandemic, and who they would identify as making decisions related to change actions. Several reported the use of ‘Zoom’ meetings to bring together senior managers, who would then email instructions to supervisors at remote sites. End-users of this information would then ‘meet’ or exchange emails to discuss, ultimately, implementation options. Organizations with a national footprint created staff workgroups that would review relevant information and then disseminate it through the organization, facilitated by regional and local managers. Local organizations with multiple areas of oversight mobilized existing topically-specific workgroups to address challenges; in a spoke-and-wheel fashion, necessary information was then pushed out to relevant parties, largely through email communications.
Discussion
In this report, we examined the profound impact of the pandemic’s first half-year on service delivery to persons with OUDs and the rapid adaptation of policy and structural changes necessitated to maintain treatment access. The most significant change was the requirement that, due to the virulence of the disease, all in-person services were severely limited and largely converted to a telehealth format. For persons with OUDs, who, in Pinellas County, who were largely treated with daily outpatient methadone dosing, dramatic shifts in service delivery were necessary. A majority of community stakeholders described the need to implement telehealth services as the most significant change during this period. Additionally, changes in methadone dosing guidance issued by SAMHSA, allowed for patients who had been stable in care, to receive multiple weeks of methadone to be taken under their own supervision. Respondents recognized this as a huge shift from the typical practice of daily-dosing and expressed praise, and some concern, over the implications of this change. Lessons learned, through some challenging moments brought on by the pandemic, included consideration of alternative methods of intervention (telehealth, alternative dosing schedules) that may be a way to expand treatment access and reduce barriers to engagement in care. Quantitative examination of possible positive and negative effects is underway. If validated, offering a ‘menu’ of services to meet the needs of treatment populations, may actualize the long-held belief that it is necessary to meet patients where they are at – both figuratively and literally. COVID-19 provided an unprecedented opportunity to examine adaptation as a process that is fast-paced, dynamic, and underscored by an incomplete and changing evidence-base. Our study has important implications for implementation practice and research. First, adaptations driven by the pandemic will only be sustained if policy makers, funders, and service providers collaborate in the near term to provide the resources and regulatory changes necessary to institutionalize the changes that are beneficial. Providers hold relevant data that can be examined to determine if the methods ‘tested’ during the pandemic should be continued. Most interviewed offered the opinion that a movement toward greater telehealth offerings and earlier access to ‘take-homes’ as being changes worth sustaining – their impact on engagement, retention and health disparities on a large scale, however, is still to be evaluated.
Additionally, existing frameworks can be enhanced to better account for the type of rapid adaptation that we observed. For example, the FRAME (for interventions) (Wiltsey Stirman et al., 2019) could be revised to include items that are tailored to a specific unplanned, triggering event (e.g. “reasons” during COVID-19 could include CARES Act funding or local decision-making that affects service access, e.g. site closures, “contextual” modifications that are specifically related to virtual care) as well as a section to document how creative, in-the-moment decisions came about. The FRAME-IS (for strategies) includes an optional section for unplanned/reactive modifications (Miller et al., 2021). Existing FRAME-IS components (such as when a strategy modification was initiated and who participated in decision-making) could readily apply to our findings (Miller et al., 2021). Additional components that could be added to FRAME-IS specifically for rapid adaptation include an assessment of resources (existing or needed) for sustaining unplanned strategy changes and the degree of alignment of unplanned strategy changes with current and expected policy regulations and funding availability.
Studying rapid adaptation during unprecedented crisis conditions offered a unique ‘in vivo’ opportunity, and limitations. Professionals were asked to reflect on conditions that were constantly evolving, but at the same time engagement in this research allowed for the evaluation of experiences never before seen. Challenges described identified the need for preparedness in access to technological resources and reconsideration of standard clinical practices. Sustaining any change determined valuable would be complicated by the fact that multiple systems would have to be coordinated to institutionalize these changes into standard practice. Research is needed to validate any proposed changes to determine if burden is reduced, increased retention and equity are achieved, subject to acceptable costs. Findings are limited by scope of the questions and sample size. The findings generated by this work will also be used to inform agent-based models aimed at exploring the potential impact of community strategies for reducing opioid overdose deaths. Overall, the pandemic has revealed the tremendous flexibility of organizations to rapidly adapt under previously inconceivable conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This paper was supported by NIDA Award: 5P30DA027828-10S1, Supplement to CENTER FOR PREVENTION IMPLEMENTATION METHODOLOGY FOR DRUG ABUSE AND HIV (CE-PIM) Project Period: 07/01/2020-06/30/2021 (12 Months).