
Abstract
Introduction
The ongoing opioid epidemic and rising number of patients with chronic pain highlight the need for alternative and integrative pain management approaches as a strategy to reduce opioid use and misuse. Evidence-based nonpharmacologic pain management strategies are available; however, they remain underutilized due to barriers including time limitations, cost, and lack of training. To address these barriers, we implemented a pain coach educator pilot program and nonpharmacologic patient toolkit in the emergency department of a large safety-net hospital. This paper describes the implementation process and preliminary evaluation of the first year of the program.
Method
We implemented a multimodal pain coach educator program that included education on pain neuroscience and over-the-counter analgesic options, demonstration of integrative techniques, and dissemination of nonpharmacologic toolkits for home use in January 2021. Implementation strategies included changing the electronic health record infrastructure, developing stakeholder interrelationships, and ongoing education and training. We used the RE-AIM framework to guide evaluation of the first year of program implementation using data from the electronic health record, program records, and patient-reported outcomes.
Results
In the first year of program implementation, 550 pain coach educator sessions were conducted. Upon session completion, 61% of patients felt the program was helpful, 39% were unsure at the time, and none reported session was not helpful. Clinician feedback was overwhelmingly positive. Program cost per patient was $344.35. Adaptations to intervention and implementation strategies included modifications of session delivery timing to accommodate clinical workflows, additions to program content to align with patient characteristics, and changes to patient identification strategies in response to the COVID-19 pandemic.
Conclusions
Our pain coach educator program provides a model for implementing nonpharmacologic pain management opioid alternatives which can be scaled and adapted for other settings. This work demonstrates the importance of intervention and implementation strategy adaptations to enhance program reach and effectiveness.
Plain Language Summary
Keywords
Introduction
Currently, one in seven Americans report experiencing a substance use disorder (Substance Abuse and Mental Health Services Administration, 2022). Since 1999, over 932,000 people in the United States have died from a drug overdose and the age-adjusted rate of overdose deaths increased by over 14% from 2020 to 2021 (Spencer et al., 2022). Over 75% of drug-involved overdose deaths in 2021 involved opioids. Opioid addiction in the United States has resulted in over 500,000 deaths and cost the economy an estimated $1 trillion in 2017 alone (Centers for Disease Control and Prevention, 2021; Florence et al., 2021). This ongoing epidemic has expanded to all socioeconomic classes and age groups (Altekruse et al., 2020; Kocherlakota, 2014).
Misuse of prescription and illegal nonprescription opioids has overwhelmed U.S. emergency departments (EDs) (Soares et al., 2022). The reasons for these increases in overdoses are multifactorial. Efforts to address the burden of pain in the United States, combined with the introduction of new opioid formulations misrepresented as having low potential for misuse, led to widespread misuse of both prescription and nonprescription opioids by the early 2000s (Jones et al., 2018). Updated prescribing guidelines along with legislative and regulatory measures have corresponded with reductions in opioid prescribing (Dowell et al., 2022; Soelberg et al., 2017; Strickler et al., 2020); however, patients are increasingly turning to illicit drugs, and opioid-related overdose deaths continue to increase (Hedegaard et al., 2021; Mattson et al., 2021). The coronavirus disease 19 (COVID-19) pandemic has contributed to the rise in opioid-related overdoses and deaths in recent years (El-Tallawy et al., 2020; Gomes et al., 2023). Increased inactivity, worsening mental health and stress, and limited access to nonprescription pain management therapies can exacerbate pain conditions and lead to a return to opioids and other high-risk medications (El-Tallawy et al., 2020).
Healthcare systems and providers face the dilemma of balancing safe prescribing and high-risk patient recognition with appropriate pain management strategies. Chronic pain affects more Americans than diabetes, cancer, and heart disease combined (Institute of Medicine, Board on Health Sciences Policy & Committee on Advancing Pain Research, Care and Education, 2011). There is a growing focus on delivering multimodal pain management interventions to reduce opioid use and misuse. A number of evidence-based approaches to pain management are available, including non-opioid medications, restorative therapies (e.g., physical or occupational therapy), behavioral approaches, and complementary and integrative health (e.g., massage, aromatherapy) (U.S. Department of Health and Human Services, 2019). Unfortunately, these approaches are often underutilized in clinical practice or not covered by insurance, and many patients lack knowledge of or access to these options (Becker et al., 2017; Groenewald et al., 2022; Hughes et al., 2002; Skelly et al., 2020; U.S. Department of Health and Human Services, 2019).
Integrating safe and effective pain management into comprehensive patient-centered care is particularly challenging in EDs. Pain is the most common reason for ED visits (Cordell et al., 2002; Todd et al., 2007). Opioid prescribing rates in the ED have declined since the early 2010s (Dowell et al., 2016; Rui et al., 2020; Suffoletto et al., 2018), which has been attributed to legislation to change prescribing practices and prescription drug monitoring systems (Cantrill et al., 2012); however, about 15% of ED patients still receive opioid prescriptions (Stephenson, 2020; Todd et al., 2007). Previous implementation projects predominately focused on improved adherence to guidelines for opioid prescribing (Trafton et al., 2010; Zgierska et al., 2018) and increased access to opioid use disorder medications (Cheng et al., 2022); however, research on implementing alternative approaches to pain management is limited. Barriers to multimodal and integrative pain management in ED settings include lack of healthcare professional pain education, lack of access to pain specialists and consistent primary care, time and workflow limitations, insufficient insurance coverage of opioid alternatives, inadequate patient knowledge about medication safety and pain, and frustration and anger over “shuffling” of care with no improvement in pain (Becker et al., 2017; Giannitrapani et al., 2017; Hooten et al., 2019; Liu et al., 2019; Mezei et al., 2011; Plaisance & Logan, 2006; Pretorius et al., 2015; Wilsey et al., 2008).
The limited integration of evidence-based nonpharmacologic approaches to pain management in routine ED care highlights the need for strategies to support the adoption of these practices. Implementation science focuses on bridging the gap between research and practice to improve healthcare quality and effectiveness using strategies to promote the adoption of evidence-based practices (Bauer et al., 2015). In this paper, we describe the process of implementing the first known ED pain coach educator program to reduce opioid use and report adaptations and preliminary evaluation outcomes using the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) framework.
Method
The Pain Assessment and Management Initiative (PAMI) was established in 2014. The initiative is multidisciplinary and focuses on multimodal and integrative pain management in healthcare systems to improve outcomes and reduce opioid risk. PAMI consists of multiple programs, including a pain coach educator program, established in 2021, which provides patient education on nonpharmacologic, integrative, and over-the-counter (OTC) analgesic options for pain management, along with a patient nonpharmacologic pain toolkit for use after discharge. Since its initial launch in the ED in 2021, the pain coach educator program has expanded to inpatient and other settings within the health system. We conducted a non-experimental program evaluation of the pre-implementation period (September–December 2020) and first year of implementation (January–December 2021) of the pain coach educator program in the ED setting to report initial strategies, adaptations, and outcomes. The project is registered with the affiliated university's Quality Improvement Project Registry.
Setting
This new pain coach educator program was implemented in the ED of a large (700-bed), urban, safety-net, not-for-profit hospital in the U.S. Southeast with approximately 62,000 inpatient admissions annually. The ED serves over 70,000 patients annually and is the region's only Level I Adult and Pediatric Trauma Center. Electronic health record (EHR) data show that most ED patients identify as Black (62%), are insured by Medicare or Medicaid (54%), or are self-pay or charity city-funded pay (24%).
Program Description
The pain coach educator program is intended for patients aged 14 years and older with acute or chronic pain. Patients were eligible regardless of if they were admitted or discharged from the ED. Patients with psychosis, suicidal or violent behavior, incarceration, severe uncontrolled pain prior to medication, restrained, immobilized, or critically ill were excluded from the program. Patients were referred to the program by physicians or advanced practice providers through an EHR paging system, phone call, or verbal request from other healthcare professionals (e.g., nurse, physical therapist). Program staff also monitored the EHR tracking board to identify eligible ED patients. The pain coach educator then reviewed the EHR to assess the patient's relevant medical history to determine their appropriateness for the program. When possible, the pain coach educator conferred with a member of the patient's healthcare team before and after the pain coaching session. Patients with frequent ED visits or admissions for pain, risk for opioid/substance use disorder, or those being started on opioids were prioritized.
The pain coach educator program components are described in detail in a publicly available toolkit on the PAMI website (PAMI, 2022b). Briefly, sessions consisted of (1) patient education on basic pain neuroscience and prevention of acute to chronic pain transitions, (2) demonstration of integrative pain management techniques, (3) a review of options to improve pain and quality of life, (4) provision of nonpharmacologic toolkit items and educational brochures, and (5) a review of appropriate OTC and topical analgesic options. The program was intended to be delivered in a single session; however, patients could participate in the program during a later admission, ED visit, or via telephone upon patient request. Brochures covered 17 topics including OTC oral and topical medications, breathing exercises, sleep, diet, pregnancy topics, and back pain. Toolkit items included aromatherapy inhalers, stress balls symbolizing a pain management analogy (American Chronic Pain Association, 2018), hot/cold gel packs, virtual reality (VR) cardboard viewers with suggested free VR apps, wearable acupressure devices, a pain journal, and a QR code to pain management videos on the program website (PAMI, 2022a). The pain coach educator customized toolkits and sessions for each patient based on their pain assessment, contraindications, patient interest, and patient characteristics (e.g., smartphone access, comorbidities). If the pain coach educator was unavailable, clinical team members could provide patients with toolkit items by accessing a stocked cart located within the different ED clinical areas.
Pain Coach Educator Qualifications and Training
The position description for the pain coach educator specified minimum qualifications of a bachelor's degree in an appropriate discipline and 4 years of relevant experience or equivalent. Preferred qualifications included a master's degree, clinical experience, and professional experience in patient education, pain management, neurobiology, or integrative medicine. In the first year, the program was primarily delivered by a master's-level pain coach educator with formal training in integrative medicine and experience as an emergency medical responder. A small proportion of sessions (approximately 5%) were delivered by other team members with varied backgrounds (e.g., public health, health education) when the primary pain coach educator was unavailable. Orientation and training of the pain coach educators included (1) training in pain neuroscience education and pain management treatment options; (2) shadowing various pain-related healthcare professionals and services in the hospital system to understand the organizational structure, work environment, and pain management clinical roles; (3) EHR training; and (4) review of current literature, textbooks, and online learning modules related to integrative and nonpharmacologic pain management.
Implementation Strategies
The primary implementation strategies used to promote the uptake of the program in the ED during the first year fell under three categories: (1) changes to infrastructure (i.e., EHR modifications), (2) ongoing stakeholder education and training, and (3) development of stakeholder interrelationships (Powell et al., 2015; Waltz et al., 2015).
Changes to Infrastructure
Our infrastructure strategies consisted of changes to record systems in the form of two EHR modifications created during the pre-implementation period. Both strategies were designed to address barriers related to time and workflow limitations (Pretorius et al., 2015; Wilsey et al., 2008). First, our team worked with the health system EHR team to develop an “auto-page” function that offered providers a simple and efficient method for referral. The auto-page strategy also enabled more efficient pain coaching sessions by communicating more patient-specific information than a regular page (e.g., provider name, patient location, details on patient condition). An EHR note template and flowsheet for each pain coaching encounter were also developed. The flowsheet populated data from nursing pain assessments and the note template included the number of past-year ED visits for the patient, history of opioid use or new opioid prescription, toolkit items given, pain management topics discussed, brochures provided, and any additional session details documented narratively by the pain coach educator. These tools supported workflow integration by decreasing the time needed for the pain coach to review patient history and conduct sessions. The note template was also designed to enhance fidelity by providing structured documentation of each intervention component.
Train and Educate Stakeholders
To address the barriers of limited healthcare professional knowledge of nonpharmacologic pain management and lack of access to appropriate resources (Becker et al., 2017; Giannitrapani et al., 2017; Plaisance & Logan, 2006), the pain coach educator regularly provided training, distributed educational materials, and conducted outreach sessions with assistance from program support staff. These activities were overseen by two program leads (PLH, SS), both ED physicians with extensive expertise in nonpharmacologic pain management. During the first year of implementation, 22 clinician training sessions were delivered to 397 clinicians and staff. Training sessions included presentations and simulation exercises for emergency medicine residents, physician assistants, faculty, ED nurses, and ancillary staff (e.g., physical therapy, pharmacy, palliative care, case managers). The single-session training was typically 30 min in length and focused on improving provider knowledge of pain and pain management and educating providers about the program and referral methods.
Regular “rounding” with healthcare teams served as a booster to these training sessions to promote referrals and provide refreshers on the program. During the rounding sessions, program staff walked through the different clinical areas of the ED to speak with healthcare teams about program resources, discuss patients currently in the ED who could benefit from the program, train teams on nonpharmacologic pain management, and demonstrate the program toolkit items. Program staff also promoted the program through a continuous on-site presence, email announcements, and visual cues (e.g., bulletin board, flyers). The intent of these strategies was to obtain buy-in and increase adoption by building provider knowledge of evidence-based nonpharmacologic pain management approaches and increase awareness of the program.
Develop Stakeholder Interrelationships
Our stakeholder engagement strategies included leveraging advisory boards and workgroups, informing local opinion leaders, and identifying and preparing clinical champions. These strategies were designed to address barriers related to clinic culture, provider awareness and perceptions of nonpharmacologic pain management, and workflow limitations. During the development of the program and throughout implementation, the team worked with the institution's Pain and Opioid Stewardship Taskforce. The task force is required by the Joint Commission and includes multidisciplinary hospital leadership. Program updates were provided at monthly task force meetings to maintain buy-in, obtain feedback on program implementation, and disseminate program materials. Clinical champions in various roles (e.g., nurses, residents, physician assistants, physical therapists, pharmacists) were identified via self- or peer-nomination to promote the program and serve as a liaison between the program and clinical staff. This served as a method to increase visibility of the program, receive feedback from front-line staff, and disseminate updates on program initiatives. Finally, to increase provider referrals the program recognized the provider issuing the most referrals as the “PAMI Star of the Month.” The provider was featured on a message board in a high-traffic area of the ED, their supervisor was notified, and a certificate was provided. This approach was chosen to align with other clinician recognition programs in our setting and capitalize on a culture of friendly competition (Majernik & Patrnchak, 2014). Further details on the program implementation, a program guide, and lessons learned are available on the program website (PAMI, 2022a).
Evaluation
The RE-AIM framework was used to guide evaluation. We chose RE-AIM because it is a well-established evaluation framework with the ability to capture patient, clinician, and setting-level outcomes (Glasgow et al., 1999). Selected outcome measures organized by RE-AIM are presented in Table 1. Data sources included the EHR, program records maintained by staff, and ED provider and patient surveys.
RE-AIM Framework Domains and Measures
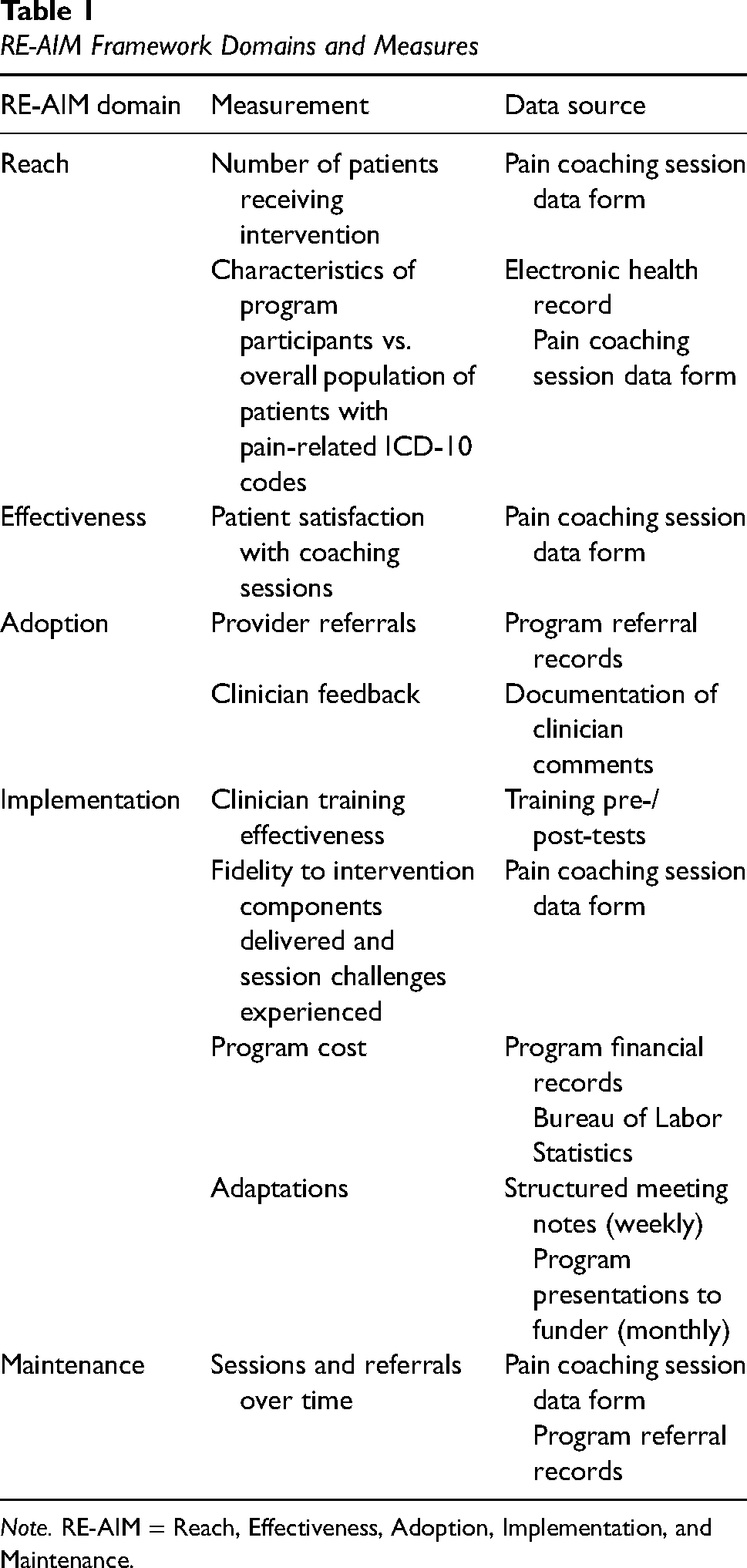
Note. RE-AIM = Reach, Effectiveness, Adoption, Implementation, and Maintenance.
Data Collection
Program staff recorded the number of referrals received and pain coach sessions conducted throughout the program. The pain coach educator documented the delivery of each session in an EHR note template created specifically for the program. In addition to the EHR note, a structured pain coaching session data form including patient demographics, pain characteristics, opioid risk assessment, pain coaching and education session components (topics coached, toolkit items/brochures provided), patient feedback, challenges experienced during the session, and patient disposition including referrals given at discharge was used (see Supplementary Appendix A). The pain coach educator also elicited and recorded patient feedback on the helpfulness of the session (yes/no/unsure) and the most helpful education topics and toolkit items on this form immediately after the session. The pain coach educator completed the form for each visit and project coordinators conducted chart reviews to obtain each patient's discharge disposition and perform data verification. All data were stored and managed in REDCap (Harris et al., 2009).
Program staff elicited provider feedback on the program during rounding and when delivering certificates to the provider issuing the most program referrals each month. Clinical champions also informed providers the program was seeking feedback, prompting some providers to email comments to the program staff; however, most clinician feedback was in the form of brief statements during informal conversations. These comments were not audio recorded but staff attempted to record comments from providers and clinical champions verbatim when possible. Clinician feedback was discussed during weekly program meetings on an ongoing basis. To evaluate clinician training sessions, a pre/post assessment measuring knowledge of nonpharmacologic toolkit items and nonpharmacologic pain management modalities was administered (see Supplementary Appendix B). We measured intervention fidelity through the documentation of session components delivered on the pain coaching session data form. We reviewed program financial records (i.e., expenditures for personnel and materials) to assess implementation and intervention costs. We used the U.S. Bureau of Labor Statistics wage tables to convert program personnel full-time equivalents (FTE) to produce more generalizable estimates (U.S. Bureau of Labor Statistics, 2021). Program staff systematically documented program challenges and adaptations discussed in weekly team meetings, which were also summarized in monthly presentations to the funding agency. The presentations and meeting notes were compiled and reviewed by the program team to produce a full list of challenges and resulting adaptations at the end of the first year of implementation. A team member with expertise in implementation science then organized these adaptations by the Framework for Reporting Adaptations and Modifications-Expanded (FRAME), which provides a structure for documenting the timing, type, goal, and rationale for intervention modifications (Wiltsey Stirman et al., 2019). The list of adaptations organized by the FRAME was reviewed by the team and refined through an iterative process. Maintenance was assessed through the number of pain coaching sessions and provider referrals over time.
Data Analysis
Descriptive statistics were generated for all quantitative measures. To measure reach and representativeness, we calculated the proportion of referred patients who received the intervention and compared the characteristics of program recipients to all patients seen in the ED with a pain-related International Classification of Diseases (ICD-10) code (e.g., headache, migraine, musculoskeletal pain, low back pain, renal colic pain) during the evaluation period. Informal feedback from clinicians was reviewed and summarized by one team member and verified by a second team member. Cost per participant was calculated by dividing the first-year total expenditures by number of participants. Costs for the pre-implementation period were calculated separately.
Results
Reach
Over the first year, 550 sessions were conducted with 549 unique patients. The characteristics of the ED program recipients and all ED patients with pain-related ICD-10 codes are presented in Table 2. Compared to all ED patients with pain-related diagnostic codes, a greater proportion of pain coach educator program recipients identified as female (65.8% vs. 54.4%) and Black (61.4% vs. 52.5%). Direct referrals accounted for 244 (44.4%) of conducted sessions. The remaining sessions (n = 306, 55.6%) were conducted with patients identified by pain coach educators and program staff through the EHR track board.
Characteristics of Program Recipients and All Emergency Department Patients With ICD-10 Codes for Pain, 2021

Note. ED = emergency department.
Patients with ICD-10 codes for headache, migraine, musculoskeletal pain, low back pain, or renal colic pain.
Effectiveness
Patient satisfaction responses (n = 550) collected immediately after the pain coach educator session are presented in Table 3. Immediately after the session, most (61.1%) recipients reported the session was helpful, 38.9% were unsure, and no patients responded that the session was not helpful. Patients most frequently identified both the coaching topics and the toolkit items as the most helpful components. Aromatherapy and the VR viewer were the most commonly reported helpful toolkit items.
Patient Satisfaction and Engagement in Coaching Topics Immediately After Pain Coach Educator Session (n = 550 Sessions)

Note. VR = virtual reality.
Could choose more than one topic or item.
Includes breathing techniques, mindful meditation, qi-gong, tai chi, and yoga.
Includes acupressure education and Aculief®.
Includes pain neuroscience education and “Car with Four Flat Tires” analogy (American Chronic Pain Association, 2018).
Adoption
In the first year of implementation, 277 referrals were received and 244 (88.1%) resulted in sessions. Referrals that did not result in sessions were due to lack of patient interest, ineligibility, or unavailable pain coach; these data were not systematically tracked. Among the 244 referrals, 134 (54.9%) were verbal and 110 (45.1%) were via the EHR or manual pages. Clinician’s comments about the program were positive. One physician described reductions in pain-related anxiety and improved mood in patients receiving coaching sessions. Another ED physician stated patients who received pain coaching seemed “happier and uplifted.” An ED pharmacist remarked that the pain coach educator helped empower patients in managing their pain and education on the pain management techniques helped reduce pain-related anxiety. The pharmacist also noted the program was successful in raising awareness of the pain coaching services and the program was well received by staff. An ED nurse also described positive reactions to the program but said it was difficult to get program information to night shift staff due to limited program availability at night.
Implementation
Fidelity
Session details are presented in Table 4. All patients were offered education on at least one pain management topic, which the patient could accept or decline. Patients were coached on most educational topics offered, with rates of educational topics offered but not coached (i.e., declined by patient, insufficient time) ranging from 0.4% (VR) to 10.8% (mind/body techniques). Most toolkits distributed included a stress ball, hot/cold pack, aromatherapy, and the program postcard. No challenges were noted for 332 (60.4%) of sessions. The most frequent challenges related to the acuity of the patient's medical condition (e.g., nausea/vomiting, lethargy) and pain level (e.g., in too much pain to participate, cognition impaired by medication).
Pain Coaching Session Details (n = 550 Sessions)

Note. VR = virtual reality.
Pain neuroscience education and “Car with Four Flat Tires” analogy (American Chronic Pain Association, 2018).
Mind/body includes breathing techniques, mindful meditation, qi-gong, tai chi, and yoga.
Acupressure includes acupressure education and Aculief®.
Program Cost
Program costs during the 3-month pre-implementation period were $24,117 ($24,011 for personnel, $106 for reference materials). Costs during the implementation period totaled $189,047 ($180,797 for personnel, $8,250 for toolkit items). Personnel included one full-time master's degree-level pain coach, one part-time (0.5 FTE) coordinator to assist with data entry, chart reviews, and toolkit item management, and one part-time (0.5 FTE) project manager responsible for day-to-day management, reporting, and administrative tasks. Personnel costs were estimated using the Bureau of Labor Statistics mean salary for health education specialists (pain coach educator), project management specialists (project manager), and administrative assistants (project coordinators) in general medical and surgical hospitals with 30% fringe benefits. The cost per patient during the first year (excluding pre-implementation costs) was $344.35.
Clinician Training Effectiveness
Pre- and post-tests were administered at two training sessions to 38 ED residents. Some residents may have attended both training sessions. Most residents had either improved or no change in scores at post-test (n = 28, 73.7%). The remaining residents showed lower scores at post-test (n = 10, 26.3%). The questions with the most incorrect answers at post-test related to deep breathing (23.7%) and hot/cold gel packs (18.4%).
Challenges and Adaptations
Table 5 presents program challenges experienced and resulting adaptations to the intervention and implementation strategies. The initial challenges experienced related to a lack of patient interest and the clinical workflow. Shortly after the program rollout, the pain coach educator recognized that approaching patients before analgesic administration was problematic in two ways. First, patients were unreceptive to the program because of their pain and frustration with the lack of immediate pain relief. Second, some patients viewed the program as interfering with or replacing analgesic pain management. To address these barriers, the pain coach waited until after the administration of analgesic medication to approach patients and introduced the program as an added service that would not impact their receipt of medications. The pain coach observed that these adaptations led to more productive sessions with patients. Another early adaptation was the introduction of a more flexible session delivery format (e.g., breaking up sessions) to avoid interfering with clinical activities. Patient feedback and pain coach observations prompted ongoing changes to the intervention content and included tailoring sessions and toolkit items to fit patient characteristics (e.g., lowering literacy level, removing items patients experiencing homelessness would be unable to use) and adding educational topics, toolkit items, and additional services (e.g., chaplain referrals) to align with patient needs, preferences, and culture.
Intervention and Implementation Adaptations Organized by the FRAME (Miller et al., 2021; Wiltsey Stirman et al., 2019)
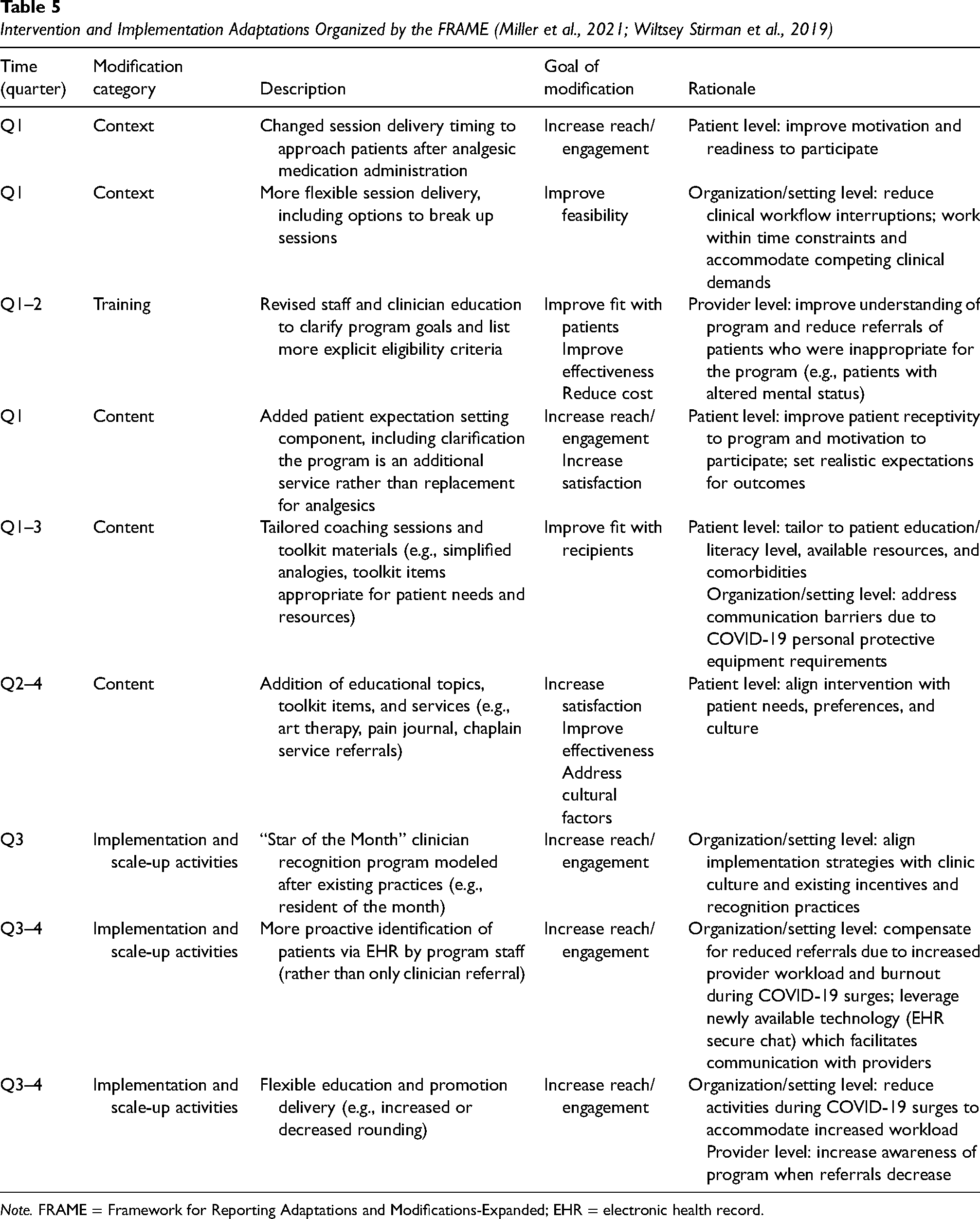
Note. FRAME = Framework for Reporting Adaptations and Modifications-Expanded; EHR = electronic health record.
Referrals for patients inappropriate for the program (e.g., excluding patients with altered mental status) prompted revised training and education to clarify eligibility. The emergence of the COVID-19 Delta wave posed a major challenge for the program, causing provider workload and burnout to increase and referrals to decline. To reduce clinician burden and maintain stakeholder relationships, program staff invested more time in identifying potential patients independently and reduced rounding and other outreach activities during COVID-19 surges.
Maintenance
The total number of sessions and sessions resulting from referrals by month are presented in Figure 1. The number of sessions steadily increased during the first 3 months of the program and then declined. A decrease in referrals was observed during the COVID-19 Delta variant wave and the related ED overcrowding and during holiday months (Centers for Disease Control and Prevention, 2022), though the total number of sessions did not fluctuate significantly.

Total Sessions and Sessions from Referral, January–December 2021
Discussion
This paper describes the implementation and evaluation of the first known ED pain coach educator program. Throughout the first year of implementation, adaptations were made to enhance the fit of the intervention and its implementation within the clinical context, external forces, and patient and clinician needs and preferences. Our findings are promising and support the need for further investigation of program effectiveness in reducing opioid use, opioid and pain-related ED visits, admissions, and increasing use of integrative alternatives in ED and other settings.
In the first year of implementation, 550 pain coach educator sessions were conducted. We found program recipients were more likely to be female and Black compared to all ED patients with pain-related ICD-10 codes seen during the implementation period; however, this is an imprecise comparison as diagnostic codes alone are not sufficient to identify patients in need of pain management support (Tian et al., 2013). Therefore, it is difficult to determine if program recipients were representative of the overall eligible population or if factors known to influence pain management, such as disparities in analgesic administration and the influence of culture and gender on pain reporting, played a role (Lee et al., 2019; Mossey, 2011). In practice, program eligibility assessment relied on clinician consultation and review of both structured and narrative EHR data. In our experience, conferring with clinicians was especially important as using features such as automated data import or copy-and-paste can result in outdated or inaccurate EHR data (Weis & Levy, 2014).
About 60% of patients reported the pain coach educator program was helpful immediately after the session. As the intent of the intervention is to provide education and tools for patients to continue to use after discharge, it is unsurprising that benefits may not be realized immediately for some patients. Furthermore, it is important to note that the remaining patients responded that they were unsure of the program's helpfulness rather than asserting the program was not helpful. Although our evaluation of effectiveness was limited to an assessment of patient satisfaction, previous research shows similar interventions are effective in improving pain intensity, pain interference, pain management self-efficacy, depression, and anxiety (Darnall et al., 2021; Rondon-Ramos et al., 2020; Siddall et al., 2022). Notably, one of these studies found a single-session program to be as effective as an eight-session cognitive behavioral therapy program (Darnall et al., 2021). Additionally, literature shows that nonpharmacologic therapies reduce opioid misuse, highlighting the importance of multimodal pain management (Gibson et al., 2020). Further research is needed to determine if our pain coach educator program produces similar results. In the second year of the program, procedures were implemented to attempt follow-up phone surveys on all patients receiving coaching sessions to better assess the program's effectiveness. Preliminary data from these assessments show high rates of continued utilization of skills 30 days after the session (Hendry et al., 2024).
The structured documentation of intervention and implementation strategy modifications is a critical first step in understanding how adaptations influence outcomes within dynamic implementation processes and contexts (Miller et al., 2021; Wiltsey Stirman et al., 2019). We were able to systematically document program adaptations by maintaining detailed logs from team meetings and frequent reports to funders. In addition, our strategy of engaging clinical champions in various roles provided us with an “on-the-ground” perspective on program challenges and adaptations. While we did not explicitly evaluate the impact of adaptations, our first-year experiences can inform the implementation of other nonpharmacologic pain management programs and other interventions delivered in ED settings. For example, approaching patients after analgesic administration can help overcome patient resistance given the high expectations for timely and effective pain management in the ED (Fosnocht et al., 2004; Motov & Khan, 2009). Our future work includes examining program adaptations during the expansion to inpatient settings to further understand strategies for adapting the program for different contexts.
Medical education programs typically devote minimal time to pain management and often focus on opioids (Shipton et al., 2018; Webster et al., 2017). This program attempted to address this gap by providing training on nonpharmacologic pain management strategies. Surprisingly, we found that about a quarter of ED residents attending training sessions scored lower on post-test compared to pre-test assessments. Most incorrect answers on post-test assessments were in relation to two topics (deep breathing, hot/cold packs), indicating the need for improved education in these specific areas. Subsequent training sessions focused on clarifying explanations of these topics and showed slight improvements in knowledge scores. We continue to conduct training sessions with incoming residents and nurses multiple times per year and now assess the impact of the training sessions on self-reported comfort in educating patients about nonpharmacologic therapies. Data from these subsequent training sessions (n = 36) show that 47% of participants felt more comfortable educating patients on nonpharmacologic modalities after the training session, 22% received the maximum score at pre-test, and 31% showed no improvement (unpublished program data; Montague et al., 2023).
We found the pain coach educator program cost $344.35 per patient during the implementation period (i.e., excluding start-up costs). Some personnel also supported program expansion to the inpatient setting during the first year of ED implementation, so this cost is likely overestimated. Nonetheless, this cost is relatively low considering the potential for the program to reduce opioid use, healthcare utilization, and associated expenditures (Watson et al., 2019). Personnel costs were higher than originally anticipated due to the need for ancillary staff for program management, toolkit inventory, and administrative tasks. Some of this need stemmed from ongoing monitoring and evaluation activities, which could be scaled as appropriate for the implementation setting and resources (e.g., capacity to obtain evaluation metrics from the EHR). These initial findings can be used to inform decisions to implement this and similar programs. Nonpharmacological and integrative pain management approaches have been shown to be cost-effective in treating various types of pain; however, more cost-effectiveness studies specific to pain management in ED settings are needed (Andronis et al., 2017; Turk & McCarberg, 2005).
The number of monthly pain coach educator referrals and sessions delivered steadily increased in the first 3 months of program implementation and subsequently declined, which may be attributable to several factors. First, patient eligibility criteria were refined in the first few months of program rollout in response to the receipt of referrals for patients who were inappropriate for the program. Second, ED volumes at our institution historically decline in summer and increase in fall and winter. Finally, in late April 2021, the pain coach educator program expanded to include inpatient settings, which reduced program staff availability in the ED. The emergence of the COVID-19 Delta variant corresponded with decreased referrals; however, due to program staff efforts to identify eligible patients, the total sessions per month remained steady during this time. Given the substantial demands on clinician time and attention, particularly in ED settings (Gualano et al., 2021; Moukarzel et al., 2019), proactive patient identification by program staff is recommended to supplement direct clinician referral methods when possible.
Strengths of this evaluation include the innovative nature of the pain coach educator program, the use of implementation science planning and evaluation frameworks, and systematic documentation of program adaptations. Despite these strengths, our approach has some limitations. First, we did not systematically document the number of patients ineligible or uninterested in the program. These procedures have subsequently been implemented in ongoing program activities. Second, clinician feedback was obtained informally rather than through rigorous qualitative methods. Qualitative data obtained through formal interviews would have provided a more robust evaluation. Finally, we reported only implementation and intervention costs rather than conducting a comprehensive economic evaluation. While the costs reported can help inform healthcare organization decisions to adopt this or similar programs, a full cost-effectiveness analysis would be more valuable.
Future Directions
This work describes a model for the design and implementation of nonpharmacologic pain education and management in the ED which can be scaled and adapted for other settings. Our findings reinforce the importance of performing ongoing evaluation and adaptation of interventions and implementation strategies. Our ongoing and future evaluation work includes the assessment of patient toolkit utilization 1 month after coaching sessions, formal evaluations of staff perceptions and experiences with the program, and the measurement of program outcomes relating to opioid use and misuse, recidivism, admissions, cost-effectiveness, and health equity. The initiative website serves as a dissemination channel and includes comprehensive toolkits, provider resources, and patient education materials to facilitate program implementation in other health systems (PAMI, 2022a). To date, the pain coaching program continues to expand to both inpatient and outpatient clinics in our healthcare system, and active dissemination efforts have resulted in the adoption of the pain coaching model in other institutions.
Supplemental Material
sj-docx-1-irp-10.1177_26334895251330511 - Supplemental material for Implementation of a novel pain coach educator program in a safety-net emergency department
Supplemental material, sj-docx-1-irp-10.1177_26334895251330511 for Implementation of a novel pain coach educator program in a safety-net emergency department by Jennifer H. LeLaurin, Magda Montague, Megan E. Curtis, Ramzi G. Salloum, Sophia Sheikh and Phyllis L. Hendry in Implementation Research and Practice
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by University of Florida College of Medicine—Jacksonville Department of Emergency Medicine; Florida Medical Malpractice Joint Underwriting Association Alvin E. Smith Safety of Health Care Services Grant; Substance Abuse and Mental Health Services Administration (SAMHSA) Emergency Department Alternatives to Opioids Demonstration Program (H79TI083101); Overdose Data to Action funded by the Centers for Disease Control and Prevention, U.S. Department of Health and Human Services; and the University of Florida Clinical and Translational Science Institute, which is supported in part by the NIH National Center for Advancing Translational Sciences (UL1TR001427). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.