
Abstract
Plain Language Summary
What is known: Unhealthy alcohol use is a significant public health issue, which has been exacerbated during the COVID-19 pandemic. Screening and brief intervention for unhealthy alcohol use is an evidence-based practice shown to help reduce drinking-related behaviors, yet it remains rare in practice. What this study adds: Using a qualitative approach, we identify barriers and facilitators to recruiting primary care practices into a funded trial that uses practice facilitation to address unhealthy alcohol use. We identify general insights as well as those specific to the COVID-19 pandemic. Barriers are primarily related to competing priorities, incentives, and lack of infrastructure. Facilitators are related to framing of the project and the anticipated level and type of resources needed to address unhealthy alcohol use especially as the pandemic wanes. Implications: Our findings provide information on barriers and facilitators to recruiting primary care practices for behavioral health projects and to implementing these activities. Using our findings, we provide a discussion of suggestions for conducting these types of projects in the future which may be of interest to researchers, practice managers, and providers.
Keywords
Introduction
At least 25% of adults in the United States participate in unhealthy alcohol use (UAU) each month, including binge drinking or exceeding weekly consumption limits (National Institute on Alcohol Abuse and Alcoholism (NIAAA), 2021a). In addition, the COVID-19 pandemic has led to an increase in both alcohol sales and unhealthy drinking (Barbosa et al., 2020; National Institute on Alcohol Abuse and Alcoholism, 2021b; Zipursky et al., 2021). UAU is associated with short- and long-term health impacts as well as societal costs (Centers for Disease Control and Prevention, 2021a; Esser et al., 2020; Stahre, 2014). Recent evidence suggests that excessive drinking has resulted in over 95,000 deaths and approximately $250 billion annually (Esser et al., 2020; Sacks et al., 2015). As such, practice guidelines and quality measures now encourage primary care providers to address UAU (Bazzi & Saitz, 2018; Centers for Disease Control and Prevention, 2014a; National Committee for Quality Assurance, n.d.; US Preventive Services Task Force et al., 2018; VA, 2013). Despite widespread recognition of UAU as an important public health concern, uptake of evidence-based practices (EBPs) to address UAU has remained relatively low and differs by patient demographics and geography (Centers for Disease Control and Prevention, 2014a; McKnight-Eily et al., 2017, 2020).
In response to the low utilization of such practices, AHRQ funded six grantees to study dissemination and implementation of evidence-based interventions to address UAU in primary care practices (Agency for Healthcare Research and Quality (AHRQ), n.d.; HHS Awards $16 Million to Help Primary Care Practices Address Patients’ Unhealthy Alcohol Use, 2019). The STop UNhealthy Alcohol Use Now (STUN) trial is one of these grantee projects and utilizes practice facilitation to implement Screening and Brief Intervention (SBI) for UAU in primary care practices in North Carolina (EvidenceNOW Managing Unhealthy Alcohol Use: The STUN (STop UNhealthy) Alcohol Use Now Trial, 2020; “Jonas Awarded $2.2 Million Grant to Address Unhealthy Alcohol Use,” 2019, ClinicalTrials.gov number NCT04317989). SBI generally includes a two-part screening for alcohol use behaviors and then tailored brief interventions such as educational materials, brief counseling, or referral to a specialist depending on the needs of the individual (Centers for Disease Control and Prevention, 2014b, 2021b). Practice facilitation is one mechanism demonstrated to increase uptake of EBPs and entails a trained individual working closely with practice to support care improvement, often through implementation of quality improvement efforts and project management (Practice Facilitation for Primary Care, 2019; Practice Facilitation Handbook, 2018).
STUN is an adaptive, randomized controlled trial that uses practice facilitation to increase uptake of evidence-based screening, counseling, and treatment of UAU in small- to medium-sized primary care practices across North Carolina. The trial design was based on the Chronic Care Model and the Improving Performance in Practice program (Cretin et al., 2016; Wagner et al., 2001; Improving Performance in Practice, 2015; Institute for Healthcare Improvement, n.d.; Margolis et al., 2010). Both of these focus on strategic efforts to improve care processes within primary care and ultimately patient health. The STUN trial is a collaboration between an academic research team and the North Carolina Area Health Education Centers (AHEC). One program of the NC AHEC includes providing practice support coaches who work one-on-one with practices across the state to review current practices, support new initiatives, and implement evidence-based practices. In the STUN trial, practice coaches serve as the primary points of contact for recruiting small- to medium-sized primary care practices into the study as well as delivering the practice facilitation intervention to enrolled practices throughout the trial. Practice coaches work alongside enrolled practices to identify and improve workflows specific to UAU screening, treatment, and referrals; assist with optimizing the use of electronic health records (EHRs) for billing/coding, panel management, and documentation; and provide practices with educational resources. Many of these practice coaches have been with NC AHEC for many years and have worked with potential STUN practices on other projects and efforts in the past. In addition, practice coaches may work with enrolled practices on STUN and other projects simultaneously.
Since the STUN project began in the Fall of 2019, the global COVID-19 pandemic has changed the healthcare, public health, and research landscape. Pressure on clinicians, practices, and researchers has made ongoing research challenging to maintain, including difficulty recruiting participants for research. During the pandemic, there has been significant discussion on how to continue implementation and practice-based research in other areas that are vital to public health during this unprecedented time (Clay, 2020; Fleming et al., 2020; Kroenke et al., 2021; McDermott & Newman, 2020). The process of generating evidence from laboratory and clinical trials in biomedical research and translating those findings into practice is protracted (Westfall et al., 2007; Zerhouni, 2006). Additionally, many findings from early studies in the roadmap of biomedical research do not translate into real-world practice. Practice-based research represents a key component in understanding and improving the implementation of evidence into real practice, and interrupting this process is costly both in terms of finances and time. Therefore, researchers and funding agencies alike have drawn attention to the importance of continuing clinical research focused on topics other than COVID-19 (Kroenke et al., 2021; National Institutes of Health (NIH), 2020; Patient-Centered Outcomes Research Institute (PCORI), 2020); however, research that involves practices and providers during the pandemic has encountered a set of novel barriers. In addition to existing challenges and workloads, many practices and providers are struggling with staffing, finances, and new COVID-19-related workflows, including shifting to telehealth and administering COVID-19 vaccines (American Association of Family Physicians (AAFP) News Staff, 2021; American Medical Association (AMA), 2020; Joint Letter to Health and Human Services (HHS) on Medicaid Relief During COVID-19 Pandemic, 2020; Primary Care Collaborative, 2020; Rubin, 2020; Song et al., 2020; Ungar, 2020).
The STUN trial is intended to advance practical dissemination and implementation of knowledge of practice facilitation as a strategy to address UAU in primary care. Low recruitment in implementation science research may bias findings and may therefore hinder the ability to translate findings from evidence-based practices into clinical practice. The purpose of the current study is to characterize the recruitment experiences of a trial focused on efforts to implement an EBP into primary care, both within and beyond the context of the pandemic. Findings from this study will advance the field of implementation science through the identification of barriers not only to recruitment of practices into a trial but also to recruitment of practices to implement an EBP related to UAU.
Methods
Sample and Data Collection
A purposive sample was used to identify practice coaches, including those experienced in working with a variety of practice types, in all nine AHEC regions across North Carolina. A member of the STUN research team facilitated introductions and invitations to coaches via email to participate in video calls about their experiences with the STUN project.
In addition to initial participant invitations, we followed a snowball sampling approach where interviewees were asked at the end of the interview if they could suggest other practice coaches who might be willing to speak with us. Interviews were conducted via institutional Zoom accounts in January and February 2021. With the consent of the participants, interviews were recorded; the built-in Zoom transcription function was used. Although applying codes to interviews, transcripts were cleaned as needed.
Interviews were conducted according to a semistructured interview guide, beginning with the background of interviewees’ general experiences as practice coaches followed by sections about their experiences with the STUN project pre-COVID and during COVID (Appendix A). The interview guide was informed by the trial design, the Chronic Care Model and Improving Performance in Practice model on which the trial was built, and recruiting experiences so far. Questions were related to the general experience of practice coaches included their time as a practice coach, whether they were involved in a previous study on which the STUN trial was based, and if they had training or experience as a healthcare provider. These questions were included to better understand the context for each coach in their experience of recruiting for STUN. Each interview concluded with a discussion about suggestions for improving recruitment for this project. We continued conducting interviews until thematic saturation was reached. Two members of the research team (CB, SR) were present for all interviews. Both researchers have qualitative research training and experience. Neither of the researchers have regular, direct contact with the practice coaches as part of the larger STUN trial. One member of the research team led each interview while the other took notes and filled in with additional questions and probes as needed.
Analysis
We used a thematic analysis to inductively identify themes and subthemes from the interviews. An inductive coding approach allows themes to emerge from the data rather than to begin with a preexisting coding scheme or proposed themes (Thomas, 2016). The two members of the research team who were present for all interviews (herein referred to as “coders”) met after each interview to document key insights and to build a list of emerging themes. After every 3–5 interviews, the coders reviewed and revised this list until a preliminary coding guide identifying themes and subthemes within the larger categories of “barriers” and “facilitators/successes” was developed. Next, both coders independently reviewed the same three interview transcripts and applied codes reflecting this coding guide. Coders met to discuss these transcripts, resolve conflicts, and refine the codebook. All conflicts were resolved through this process resulting in agreement on codes and the codebook from these three interview transcripts. This was considered a consensus among the coders. Next, the remaining interviews were divided among the two coders. Next, each coder reviewed the interviews coded by the other to ensure consistency in coding approaches. Lastly, the two coders reviewed code use and frequencies across all interviews and together decided which codes to combine and remove as needed. Only subthemes that were coded in at least three of the interviews are presented in the results. Analyses were conducted in ATLAS.ti version 9 (Berlin, Germany). This study was approved by the institutional review board at University of North Carolina at Chapel Hill.
Results
Invitations were sent to 16 practice coaches in January 2021. Fifteen practice coaches agreed to participate, and one did not respond after a second invitation was sent, making the final response rate 94%. Interviews were scheduled for one hour but ranged from 17.5 to 42.5 min with a mean time of approximately 31 min. Across the interviews, perspectives from all nine AHEC regions were represented. Participating practice coaches described experiences working with small practices, independent practices, rural and urban areas, large health systems, federally qualified health centers (FQHCs), and other practice types. Participants had a range of experience working as AHEC practice coaches, ranging from a few years to more than a decade. A total of three barrier themes with 12 subthemes and six facilitator themes were identified.
Barriers
Pandemic-Related (COVID-19) Barriers
Shifting Focus to COVID-19 Efforts
Participants highlighted four barriers to recruitment for the STUN project related to the ongoing COVID-19 pandemic (Table 1). A foremost concern was shifting focus away from typical primary care efforts to COVID-19, including introducing new pandemic-related safety measures, testing, and vaccinating into workflows as well as navigating new administrative tasks, such as billing and coding for COVID-19-related care. Coaches described this shift as requiring everyone's full attention because it was uncharted territory. One coach emphasized the difficulty in learning how to manage a new disease: “When was the last time in modern history we had a new disease that they had to learn as fast as they could, when science couldn't even provide a lot of research for them, you know?” (Interview 9). A few coaches also noted examples of practices that had agreed to participate in STUN before COVID-19 but then decided to withdraw or pause their participation because of the new demands related to the pandemic.
Barriers.

Note. EHR = electronic health record; AUDIT-C = Alcohol Use Disorders Identification Test-Concise (a validated, brief tool for alcohol screening); UAU = unhealth alcohol use.
Staffing Issues
Staffing challenges related to the pandemic were another prominent issue, affecting willingness to participate in a new project, as illness, quarantines, and inability to find childcare made it difficult to keep practices fully staffed. One coach summarized these challenges as: “So whether it's people leave or it's short term or someone is sick, it's all of the above, leading to staffing issues still. Now I hear it every day” (Interview 15). Several coaches mentioned practice and provider experiences with severe COVID-19 including hospitalizations and deaths of providers and practice staff.
Financial Concerns
Several coaches highlighted how pandemic-related financial concerns drained practices’ ability to concentrate on tasks and even forced some practices to consider closing. One coach said: “I have three independent practices currently that have closed their doors for two weeks because of being short staffed plus having to quarantine.” (Interview 14) Although most described the financial constraints brought on by the pandemic, one coach also noted the opposite. When I say financial burdens, I’m not talking about only losing money. They have also been inundated with financial opportunities and so to navigate those financial opportunities and to keep track of those and to apply for those financial opportunities and then figure out what to do with that new all that new money. That has been overwhelming. (Interview 6)
Coaches Distanced from Practices
Coaches expressed that not being able to interact with practices in-person hampered their ability to establish workflows, provide support, and maintain relationships with practices, which has affected recruitment. In addition, the pandemic and the associated challenges have made it difficult for coaches to find time to communicate with and support practices and providers in general (even through virtual connections), making them feel increasingly distanced and pressed for time to bring up new initiatives like STUN. Compared to when coaches could provide support directly alongside providers, one coach described the challenge in providing support during the pandemic. So it's also really hard for us to support the practice. To say, let me show you how we can do this easier because I need them to like, show it on their screen and me sit and try to figure it out. (Interview 1).
Practice-Specific Barriers
Practices have Competing Demands
Nearly all coaches affirmed that a primary reason that practices were unlikely to enroll in research studies at this time was a proliferation of competing demands, even outside of the pandemic. For example, North Carolina completed Medicaid transformation from fee-for-service to managed care in July 2021, requiring attention from practices as they prepared for the transition. Practices also want to continue participating in various quality and reimbursement initiatives, most notably Meaningful Use, Merit-based Incentive Payment System (MIPS), and patient-centered medical home certification. One coach pointed out that “very few practices are looking forward, they’re just trying to put all the pieces together most days” (Interview 1).
Practice Infrastructure
Participants described practice infrastructure as a barrier to entry, as practices often lack adequate resources including staffing, time, and technology. Even before the pandemic, small primary care practices often struggled to recruit and retain staff, with a resulting lack of adequate training for the staff they do have. According to one coach, time presented a “double-edged sword…they need the resource [practice coaching] and they want them in there and they always want [support], but it can be very hard for them to find the time to give to coaching” (Interview 10). Some practices lack EHRs capable of implementing a project focused on UAU while others lack an EHR altogether. For example, some EHRs have built-in screening tools for UAU that allow for streamlined development of workflows, while others lack appropriate screening tools; the latter practices must build the infrastructure to screen for UAU either within the EHR or by bypassing it.
Working with Practices and Health Systems
Organizational structures and workflows also presented unique barriers. Coaches described practices that are integrated with health systems as more challenging for recruitment and implementation because of the oversight and structures in place. One respondent illustrated the situation as such: “Which comes first, the chicken or the egg? Do you get support and then take it to the upper management and leadership or do you go to local leadership and let it be their idea and then take it to the practices?” (Interview 2). Coaches described internal practice structures as a barrier in both independent practices and those that are a part of a health system. In many situations, practice managers acted as gatekeepers, resulting in differences in how coaches recruited or described the STUN project to practice managers compared to providers. Coaches described focusing the recruitment message on workflows and reimbursement when talking with practice managers. In contrast, coaches took a different approach with providers, focusing on patient health and well-being. Finally, coaches have made repeated efforts to recruit practices. Several participants stated that they did not want to continue to approach practices that they know are not interested or capable of taking on projects like this.
Insufficient Incentives
Several participants also stated that the study's incentives, financial or otherwise, were insufficient to motivate participation given their current financial situation or staff bandwidth. This was described by one coach as follows: There's usually not a whole lot of money that can be offered to them and [money] usually works. I mean sometimes it works, but sometimes there's just not money available. (Interview 12)
Project-Specific Barriers
Project rollout
Participants mentioned four barriers specific to the project. First, coaches described being adversely affected by the iterative rollout of the project. In order to successfully recruit practices, some coaches wanted additional materials including more workflow diagrams and information related to data extraction. One coach described their perspective: I think the hesitation once we started learning more began with how we’re going to collect this data. Are we going to be able to pull [it]? (Interview 13)
Sensitive Topic
According to several participants, some physicians are hesitant to broach the topic of alcohol use with patients. One practice coach described a specific regional concern: It's a heavily religious area, but people drink, they just don't want to publicize that they drink, you know what I mean? So good old boy Doc that's known him for 10 years, he may have a really hard time saying, “tell me exactly how much you drink.” (Interview 10)
Not all participants agreed, with several noting that the subject's sensitivity would not inhibit a physician from inquiring.
Follow-up on Positive Screens
Participants noted that practices have expressed concerns about how to follow-up on positive screens, and that this in turn bred resistance to participating in the project. Many practices are based in rural settings, where specialized services for UAU are harder to access. One coach described this challenge in the following way: “I’m not going to ask the question if I’m not sure I have a place to send my patients for counseling.” (Interview 9)
Alcohol not a Top Priority
Coaches suggested that alcohol use was viewed as a lower priority than other health and wellbeing concerns by some practices, either due to perceptions that unhealthy use is rare or that other health conditions are more important. One coach described “the whole idea of screening for alcohol use, it wasn't on the top of their [practices] list like a normal clinical process like cardiovascular disease…something that they worked on every day already.” (Interview 5)
Facilitators and Successes
Facilitators and examples of successes were also described by participants (Table 2).
Facilitators and successes.
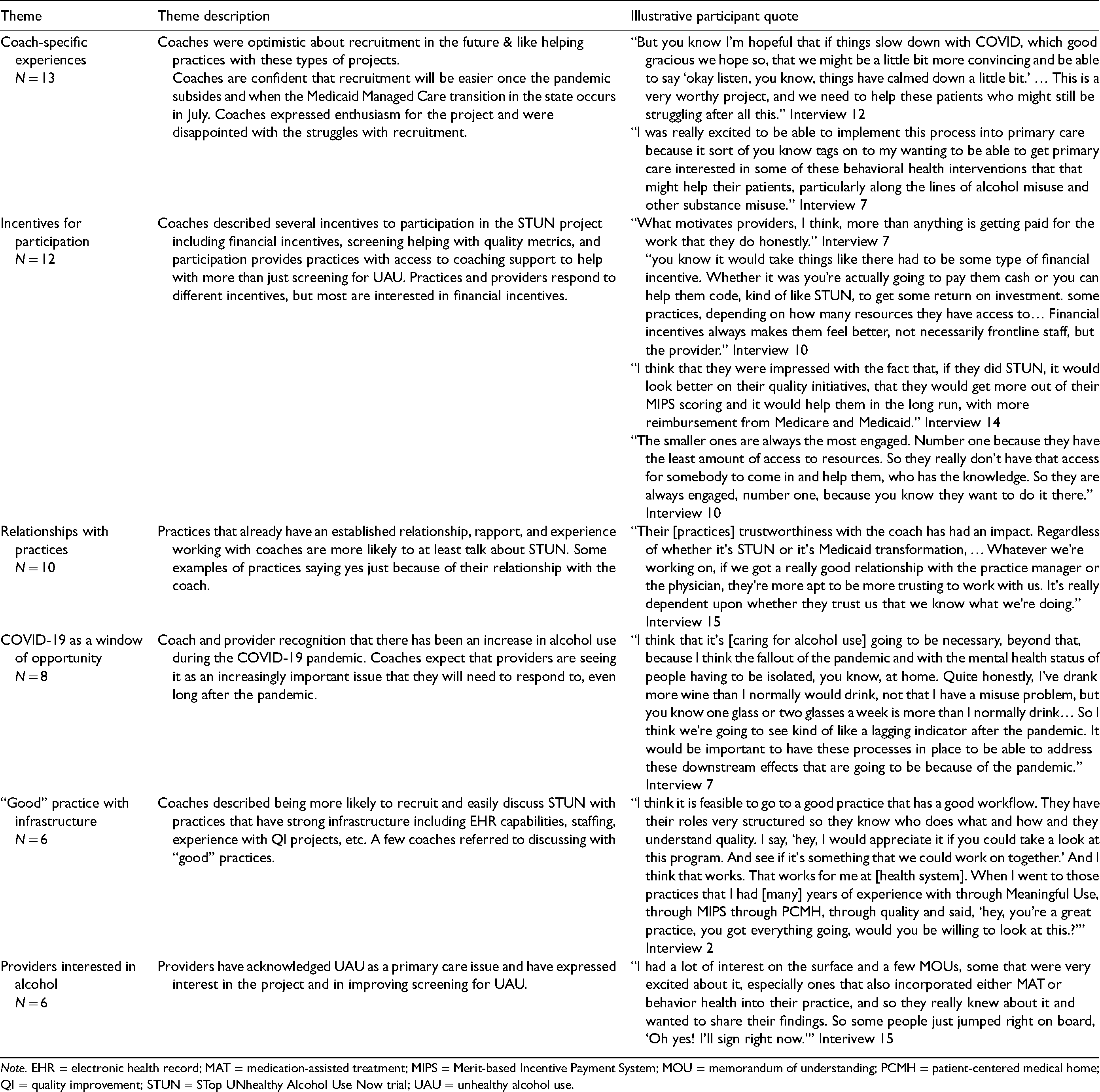
Note. EHR = electronic health record; MAT = medication-assisted treatment; MIPS = Merit-based Incentive Payment System; MOU = memorandum of understanding; PCMH = patient-centered medical home; QI = quality improvement; STUN = STop UNhealthy Alcohol Use Now trial; UAU = unhealthy alcohol use.
Coach-Specific Experiences
Participants emphasized their own enthusiasm and optimism about the project. One coach stated “I was really excited to be able to implement this process into primary care because it tags on to my wanting to be able to get primary care interested in some of these behavioral health interventions that might help their patients” (Interview 7). Another coach noted their optimism about the project's future: I’m hopeful that if things slow down with COVID… that we might be a little bit more convincing…this is a very worthy project, and we need to help these patients who might still be struggling after all this. (Interview 12)
Incentives for Participation
Several participants noted that a project focused on increasing alcohol screening fit well within practices’ various quality and reimbursement initiatives. Participants emphasized how important incentives are to motivate practices to participate. One coach described the importance of financial incentives, “What motivates providers, I think, more than anything is getting paid for the work that they do, honestly,” (Interview 7) while another coach highlighted non-monetary incentives as well: They [practices] are just thrilled to get the hours of a coach to come in and help them, kind of, either understand where they’re at or where they need to start. And that's with the research study, but these practices also usually have problems in other areas, so they’re just happy to get the free hours of a coach to come in, and you know kind of look at their stuff. (Interview 10)
Of note, STUN provides financial incentives for practice staff and providers who complete surveys and STUN provides training for practices related to billing for screening and counseling services related to UAU, so that practices can learn to receive appropriate compensation for their work.
Relationships with Practices
Many participants identified existing relationships with providers and practice managers as key to their success in persuading practices to enroll in STUN. One coach highlighted their approach: “Regardless of whether it's STUN or it's Medicaid transformation… if we got a really good relationship with the practice manager or the physician, they’re more apt to be more trusting to work with us.” (Interview 15)
COVID-19 as a Window of Opportunity
Although the pandemic presented numerous obstacles, coaches highlighted that COVID-19 also presented a window of opportunity to address many systemic issues affecting population health, including UAU. One coach suggested that recognition has increased in response to the uptick in alcohol consumption during the pandemic. We’re going to see kind of like a lagging indicator after the pandemic. It would be important to have these processes in place to be able to address these downstream effects that are going to be because of the pandemic. (Interview 7)
“Good” Practices with Infrastructure
Several coaches described having more success recruiting “good” practices and further describing them as those with strong infrastructure. One coach discussed their experiences recruiting practices with established workflows as follows: I think it is feasible to go to a good practice that has a good workflow. They have their roles very structured so they know who does what and how and they understand quality. I say, “hey, I would appreciate it if you could take a look at this program. And see if it's something that we could work on together.” And I think that works. (Interview 2)
Providers Interested in Addressing Alcohol Use
Participants also discussed how some providers are interested in UAU specifically. Likewise, several have structures in place that allows easy integration of a project like STUN. One coach described that practices: Had a lot of interest on the surface and a few [signed agreements], some that were very excited about it, especially ones that also incorporated either [medication-assisted treatment] or behavior health into their practice, and so they really knew about it and wanted to share their findings. So some people just jumped right on board. (Interview 15)
Discussion
The current study describes the experiences of practice coaches in recruiting primary care practices to implement an UAU screening intervention during the COVID-19 pandemic. Barriers to recruiting practices for the STUN project may be relevant to others planning similar projects in the future and are germane to interpreting the findings of the larger AHRQ evaluation of interventions to implement EBPs related to UAU. Barriers generally fit into two categories: competing priorities for practices (including those related to the COVID-19 pandemic) and variation in practice infrastructure.
Many of the barriers identified were related to the priorities of and constraints on practices. With respect to the pandemic, coaches echoed many of the barriers described elsewhere (AAFP News Staff, 2020; AMA, 2020; Joint Letter to HHS on Medicaid Relief During COVID-19 Pandemic, 2020; Primary Care Collaborative, 2020; Rubin, 2020; Song et al., 2020; Ungar, 2020) including the major shift to addressing COVID-19, establishing new procedures and workflows, understanding a new disease, and managing staffing shortages during this time. Importantly, coaches perceived similar COVID-related barriers among all types of practices, including those of varying sizes, demographics, and geographies. Although the barriers related to COVID-19 are similar, the variation in resources may result in differences in the ability to overcome those barriers.
Outside of the pandemic-related barriers, many other challenges exist to both recruitment practices for research or buy-in to implementation of EBPs, and therefore have hindered recruitment. Many of these barriers also echo those identified in other practice-based research and evidence-based medicine such as lack of adequate incentives, practice managers or administrators as gatekeepers, challenges within health systems, infrastructure challenges, and such activities being low priorities (Loskutova et al., 2018; Sadeghi-Bazargani et al., 2014). Small, independent, and rural practices are always resource-constrained and face competing demands unique to their circumstances. First, practices are often spread thin trying to meet requirements of the numerous quality and reimbursement reform efforts being promoted by national or state policy and various payers such as Meaningful Use, MIPS/Medicare Quality Payment Program, FQHC requirements, and many more (AAFP, 2020; CMS: Quality Payment Program, n.d.). Program requirements also change over time, forcing practices to shift focus and relearn reporting requirements year after year. Second, many practices are facing increasing consolidation as health systems acquire smaller practices in the area and the pandemic is expected to continue this trend (Furukawa et al., 2020; Gustafsson & Blumenthal, 2021; Schwartz et al., 2020). This creates changes in market dynamics both within practices that are acquired and those that remain independent. Finally, practices are motivated by financial incentives, which often focus on screening and management for chronic illnesses. Incentives that practices see as insufficient for the effort and anticipated outcomes may impede enrollment.
Infrastructure of practices is also a critical component for participation in the STUN trial and findings from this study echo previous work on the adoption of EBPs more generally (McNeely et al., 2018; Pagoto et al., 2007; Sadeghi-Bazargani et al., 2014; Tacia et al., 2015). For example, a qualitative study of barriers and facilitators to screening for substance use in primary care also identified lack of time and provider training as barriers (Loskutova et al., 2018) while a systematic review of barriers to evidence-based medicine practices found that a general lack of resources and time, as well as logistical barriers, were commonly identified across included studies (Sadeghi-Bazargani et al., 2014). Practice resources, staffing, and experience with behavioral health, EHRs and quality measures may all affect willingness to participate, as they affect practices’ ability to implement such projects and services. Additionally, coaches recognized that the practices that most needed the support and are most likely to benefit from the STUN project are those with the least infrastructure, who face the greatest obstacles to participation and implementation. Overcoming these more general infrastructure obstacles will require targeted funding and system-level reforms.
Limitations
Although this project provides valuable insight into the experience of recruiting practices for a behavioral health intervention during unprecedented conditions, it is not without limitations. First, there are aspects of this project that may limit the generalizability of the findings. For example, the STUN project may have a structure that is unusual in that practice coaches are heavily involved in recruitment, and it is focused on an alcohol-specific intervention. In the current study, many of the practice coaches already had established relationships with the potential practices which may aid in recruitment. Additionally, both the pandemic and the project have progressed through many different phases. Interviews for this study took place in January and February 2021 when the pandemic was near its peak nationally and locally (CDC, 2021c; NCDHHS, 2021-a) and before vaccinations were widely available to the general public (U.S. Food & Drug Administration, 2020). During this time, a modified stay-at-home order was in place, many people were working from home and schools were encouraged to be virtual, leading to many logistical burdens (NCDHHS, 2021b; Wagner, 2021). Recruitment for the STUN project was largely on hold during this time because of the pandemic. Results of this study should be interpreted with respect to this timing and not all may be generalizable to other contexts. Second, practice coaches gave assessments of what the practices were experiencing, which is an indirect assessment of practice perspectives. Third, while we do provide counts of the number of coaches that described a given theme, the interviews followed a semistructured format and followed the natural flow of the conversation. Not mentioning a specific theme does not mean that a coach did not perceive it. Therefore, these counts are likely underestimates.
Clinical and Research Implications
The COVID-19 pandemic has shed light on many of the challenges that primary care practices face as well as the vital role they play in supporting the health of our population. This study not only contributes to evidence on recruiting practices for practice-based research but also provides insights on hesitation regarding the implementation of EBPs related to UAU. The findings and recommendations described here may be valuable for researchers, health systems, practice managers, or others planning for various primary care-based interventions or promoting the adoption of EBPs in the future. For an audience of either individuals recruiting for research or approaching practices to implement EBPs, building on existing relationships and tailoring outreach may help improve recruitment or uptake. For example, we found different messaging was used by coaches when targeting practice managers compared to providers. Coaches perceived that practice managers seemed more motivated by workflows and reimbursement, and that clinicians seemed more receptive to messages about patient health and well-being. Our study also suggests that specific materials may be needed for coaches to feel more confident in their ability to recruit, including data collection tools and EHR process support. Finally, barriers to participation often reflect the competing priorities and infrastructure obstacles that many primary care practices face. Whatever researchers, practice coaches, or others can do to reduce barriers to implementing EBPs may increase the chances of successful implementation. Financial incentives and providing practical support may be especially useful.
System-level interventions may also be effective in promoting EBPs. Different payment models that support infrastructure such as Centers for Medicare & Medicaid's Comprehensive Primary Care Plus (CPC + ) model (Centers for Medicare & Medicaid Services, n.d.; Comprehensive Primary Care Plus, n.d.; Deborah Peikes et al., 2019; Primary Care First CMS, n.d.) are examples of the type of efforts that could help practices overcome these barriers. CPC + in particular provides financial support up front for investment in needed infrastructure to improve care quality. Challenges with EHRs may be addressed by EHR vendors through making validated screening tools more easily accessible (e.g., AUDIT-C, AUDIT). Collectively, these types of models or changes could allow practices to overcome these obstacles to being able to implement EBPs with fidelity. More research in this area is needed to further explore best practices for recruitment in practice-based research.
In response to the barriers and facilitators identified in the current study, we provide several recommendations that may be useful for researchers or practitioners designing and implementing similar projects in the future. First, it is important to consider how to tailor interventions, workflows, and supports to best support practices of different types and with differing infrastructure. Different strategies may be useful as well when trying to recruit different types of practices (e.g., part of a health system, in an ACO, FQHC, rural, etc.) or engaging with different stakeholders such as providers or practice managers. In our study, coaches with already established relationships with practices felt well-suited to adapt their strategies based on their knowledge of the practice and staff. Second, interventions for different conditions have their own unique requirements. Considering the anticipated challenges specific to the intervention and/or condition may help to better prepare for those differences. Finally, those who are doing the recruiting are instrumental to the success of the project. In the STUN study, recruitment was done by practice coaches who were employed by an organization separate from that of the research team. Often, coaches already had established relationships with these practices. Learning from them and soliciting their feedback may ease the recruitment process.
From the practice perspective, our study suggests that there may be several strategies to facilitate practice uptake of EBPs. First, develop training support for providers that covers topics related to documentation and billing, how to address positive screens, and what treatment resources are available in the community. Having the necessary training and knowledge of resources may increase provider confidence in addressing sensitive topics such as UAU. Second, both leadership and provider support are important but may present different challenges. Providing clear messaging and value added to the organization, providers, and patient outcomes may help garner interest and buy-in from all practice staff and leadership. The potential for increased reimbursement, meeting quality metrics, and improved patient outcomes are all examples of potential benefits practices may experience from implementing this particular EBP.
Supplemental Material
sj-docx-1-irp-10.1177_26334895221094297 - Supplemental material for Barriers to recruiting primary care practices for implementation research during COVID-19: A qualitative study of practice coaches from the Stop Unhealthy (STUN) Alcohol Use Now trial
Supplemental material, sj-docx-1-irp-10.1177_26334895221094297 for Barriers to recruiting primary care practices for implementation research during COVID-19: A qualitative study of practice coaches from the Stop Unhealthy (STUN) Alcohol Use Now trial by Casey P. Balio, Sean R. Riley, Debbie Grammer, Chris Weathington, Colleen Barclay and Daniel E. Jonas in Implementation Research and Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality (grant number 1R18HS027078-01).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.