
Abstract
Psychedelic therapies are an emerging class of treatments in psychiatry with great potential, however relatively little is known about their interactions with other commonly used psychiatric medications. As psychedelic therapies become more widespread and move closer to the clinic, they likely will need to be integrated into existing treatment models which may include one or more traditional pharmacological therapies, meaning an awareness of potential drug-drug interactions will become vital. This commentary outlines some of the issues surrounding the study of drug-drug interactions of this type, provides a summary of some of the relevant key results to date, and charts a way forward which relies crucially on multimodal neuroimaging investigations. Studies in humans which combine Positron Emission Tomography (PET) and functional Magnetic Resonance Imaging (fMRI), plus ancillary measures, are likely to provide the most comprehensive assessment of drug-drug interactions involving psychedelics and the relevant effects at multiple levels of the drug response (molecular, functional, and clinical).
Psychedelic Therapy (PT) is a modern re-emergence of a therapeutic paradigm that originated in the mid-20th Century, but with antecedents in traditions which stretch back into pre-history. 1 The modern incarnation typically involves administration of a psychedelic substance in a clinically-controlled manner, often within a psychotherapeutic or psychological support framework. 2 After a long period of stagnation following legal restrictions on psychedelic drugs which came into force in the late 1960s, PT is re-emerging as a viable therapeutic paradigm for a range of disorders, bolstered by encouraging early-phase clinical trial results.3 -6 With the first phase III trials currently underway or recently completed, 7 and PT now a licensed treatment in Australia, 8 the wider use of PT in many jurisdictions appears to be almost an inevitability.
Wall et al 9 recently outlined the role that neuroimaging has played in the modern development of these pharmacotherapy approaches. Functional Magnetic Resonance Imaging (fMRI) studies have formed a crucial part of mechanistic-focused studies with healthy10,11 and clinical populations.12 -14 The former have provided greater understanding of the uniquely powerful effects that acute dosing with psychedelics can have on consciousness, cognition, and perception, and led to a number of theoretical advances.15,16 Contemporaneously, clinical neuroimaging studies have provided important insights into the longer-term therapeutic effects, including changes in emotional processing,17 -19 cognitive/neural flexibility, 14 and effects on more general measures of brain function.13,14 The Wall et al paper makes the point that the advance of modern neuroimaging methods means that, for the first time, there is an opportunity to develop these drugs for clinical use, while continuing basic science investigations on their mechanisms, neural, and physiological effects. Ideally, both streams of research will advance concurrently, and each will influence the other in important aspects, as well as provide translational implications for the wider field of psychiatry. The authors sketch out a set of key questions and possible study designs using multimodal neuroimaging (principally fMRI combined with Positron Emission Tomography; PET) and ancillary techniques that will advance our understanding of these drugs and provide a foundational platform for further clinical development.
One crucial question, only briefly touched on by Wall et al is that of drug-drug interactions involving psychedelics. The overall approach of psychedelic therapy (involving perhaps only 1-3 doses administered under controlled conditions in most clinical trials conducted so far) is quite advantageous in terms of minimizing risks of unwanted interactions (as well as tolerance and ongoing side effects). However, caution is still warranted, particularly regarding interactions between psychedelics and anti-depressants. Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin and Noradrenaline Reuptake Inhibitors (SNRIs) are widely prescribed as a first-line pharmacological treatment for depression and anxiety, 20 as well as “off-label” use in a range of other psychiatric indications, such as eating disorders. 21 Since “classic” psychedelics (eg, psilocybin, LSD, DMT) are serotonergic drugs with a primary site of action for the subjective effects of psychedelics being the 5-HT2A receptor, 22 drug-drug interactions between psychedelics and SSRIs/SNRIs are highly plausible. Broadening the focus somewhat further, all classes of anti-depressants are monoamine modulators, and many psychedelics have wider actions on monoamine systems (eg, LSD is an agonist at 12 different 5-HT receptors, and all five classes of dopamine receptors 23 ). Expanding the perspective once again and considering non-classic psychedelics with diverse pharmacological actions such as MDMA (broad effect on monoamine release), ketamine (NMDA receptor antagonist), and ibogaine (effects on NMDA, nicotinic, and opioid receptors, among others), the range of potential interactions with several commonly used drug classes becomes notably more complex. Polypharmacy (prescription of two or more medications concurrently) is a common treatment model in psychiatry 24 in order to address different symptom clusters, treat co-morbid disorders, and fine-tune treatment to particular patient’s needs. Combination therapy for the specific purpose of augmenting clinical effects is also relatively standard practice in some indications (eg, treatment-resistant depression), with NMDA-targeting drugs (ketamine), mood stabilizers (lithium) and anti-psychotics most commonly used. 25 As psychedelic therapy becomes more widespread, a clearer understanding of the likely interactions with other medications will become vital for it to be accommodated within existing polypharmacy/combination treatment models.
The 2 major classes of drug-drug interaction effects for psychoactive drugs are pharmacokinetic and pharmacodynamic interactions. 26 Pharmacokinetic interactions are peripheral actions where one drug can affect the metabolism, absorption, excretion, or distribution of another drug. The overall effect is either to raise or lower the concentration of drug in the blood (for a given dose) and/or modify the time course of the drug’s overall metabolism. Pharmacokinetic interactions are commonly caused by medications (eg, rifampicin, carbamazepine, phenytoin), foodstuffs (eg, grapefruit juice) and herbal remedies (eg, St John’s Wort), and can have unintended effects on a range of commonly prescribed medications, including anti-hypertensives, anti-coagulants, mood stabilizers, and statins. 27 There are also synergistic interactions which have positive and desirable effects. An example is L-dopa, a precursor to dopamine, used in Parkinson’s disease. Carbidopa, when combined with L-dopa, prevents its conversion into dopamine outside the brain, and improves effectiveness by achieving a more continuous and less fluctuating supply of dopamine to the brain. 28 Intriguingly, the preparation of ayahuasca, the Amazonian psychedelic brew that has been used for thousands of years, exploits this synergistic interaction effect in a remarkable example of “folk” pharmacology. 29 The primary psychoactive ingredient in ayahuasca is N,N-dimethyltryptamine (DMT), which is rapidly metabolized by monoamine oxidase in the gut and rendered inactive; oral dosing of pure DMT produces no psychoactive effects. However, ayahuasca also uses other plant matter which contains harmalines; natural monoamine oxidase inhibitors (MAOIs). These prevent the deamination of DMT by the gut enzymes and markedly change the pharmacokinetics of DMT from effects that last a few minutes (if vaporized or smoked) to several hours (if consumed as ayahuasca). 29
In contrast, pharmacodynamic interactions are interactions between drugs that have either similar or opposing pharmacological effects, often interacting with the same receptor sites or body systems. These interactions can be either additive, synergistic, or antagonistic effects of two drugs at a particular receptor target, or on downstream systems (eg, second messenger effects, hormonal effects). 30 One clear example used routinely in research on psychedelic drugs is the attenuation of psychedelic-like effects following co-administration of 5-HT2A antagonists such as ketanserin or risperidone. These can produce an almost complete block of the subjective effects of LSD 31 and psilocybin 32 in human subjects. Other commonly prescribed medications, including mirtazapine, olanzapine, quetiapine and trazadone all exhibit strong affinity to 5-HT2 receptor sites, and may have similar effects. A less clear-cut example is the interaction between LSD and mood stabilizers such as lithium or lamotrigine. Some reports have indicated that chronic use of lithium may enhance the subjective effects of LSD, 33 while more recent surveys have indicated that use of lithium with classic psychedelics induced seizures in 47% of users, with no reports of adverse consequences of lamotrigine plus classic psychedelics. 34 Lithium has complex effects on the serotonin system, with overall effects likely differing depending on acute (increased synthesis and release of serotonin by inhibition of presynaptic 5-HT1A) or chronic (downregulation of 5-HT2 receptors) administration. 35
Psychedelic therapies are now legal medicines in Australia 8 and are moving toward legalized status in a number of other jurisdictions. As larger clinical trials are conducted, with more diverse samples, and these treatments ultimately become available to the broader population, developing an understanding of drug interactions and their clinical significance will become a more pressing concern. Our aim here is not to provide an exhaustive catalog of the possible interactions between psychedelics and other drugs (many of which remain uninvestigated in any meaningful manner) but to sketch out possible experimental approaches to tackling the issue in human subjects. Pharmacokinetic (peripheral) interactions can be investigated with relatively simple and established in vitro and in vivo methodologies,36,37 so our main focus here is investigation of pharmacodynamic (central) interactions. Pre-clinical work clearly has a vital role to play in such investigations, however species differences in the structure of the 5-HT2A receptor, 23 potential brain penetrance differences, 38 and the limitations of animal models for assessing subjective effects and treatment efficacy mean that human studies are also essential.
Perhaps the most serious concern with psychedelic drug interactions is the possible risk of serotonin toxicity or serotonin syndrome; a rare, but potentially life-threatening, toxidrome that can occur with (combinations of) drugs capable of increasing serotonin neurotransmission. 39 For example, combining MAOIs, which inhibit monoamine breakdown, with SSRIs, which block the reuptake of serotonin, can result in serotonin syndrome due to the combined effect on serotonin activity. 40 A more prosaic, but still important, issue is that it is currently unclear whether or how use of other psychiatric medications may affect the process or outcomes of psychedelic therapy. Most clinical trials involving psychedelics have required subjects to taper off their existing medications and have excluded patients with any co-morbidities. Tapering off patients from existing medications is not without risk, with patients reporting withdrawal symptoms from SSRIs, including somatic effects, electric shock sensations, and mood disturbances which some patients report as feeling like they have relapsed into their prior episode of mental illness. 41 One recent study has also suggested that patients who discontinue SSRI/SNRI medication before psychedelic therapy showed reduced benefits, compared to unmedicated patients. 42 Medication titration requires increased monitoring from the patient’s primary care provider to ensure that they are adequately safeguarded and supported during the tapering process.
The current state of knowledge related to interactions between MDMA/psilocybin and a range of other drugs has been outlined in a recent systematic review, 43 and readers are encouraged to consult this source (and the many primary studies cited therein) for particular details. However, since this review’s publication four additional studies have been published: two observational and two from controlled settings. The first observational study 44 used a retrospective design and found that concurrent or prior SSRI/SNRI use may be associated with weaker acute psilocybin effects up to approximately 3 to 6 months after discontinuation, although this occurred only in about half of participants. The other observational study 45 used a prospective design and similarly found that concurrent SSRI/SNRI use might reduce the intensity of the acute psychedelic experience (in terms of mystical experiences, emotional breakthroughs and challenging experiences) compared to participants who were not treated with these medications. This may be important as these experience have been linked to positive treatment outcomes in previous studies, 46 however, the changes in depressive symptoms appeared comparable in the two groups in this study. 45 The first controlled crossover study 36 focused on healthy subjects that were pre-treated for 14 days with escitalopram (or placebo) before psilocybin dosing sessions. Pre-treatment with escitalopram had no effect on the pharmacokinetics of psilocybin, and no effect on a range of other measures, including gene expression, increase in circulating Brain Derived Neurotrophic Factor (BDNF) levels and cardiac effects. The general mind-altering effects of psilocybin were also maintained as well as positive emotional effects, however there were significant decreases in several measures related to adverse/negative effects, notably anxiety-related outcomes. However, the relatively short duration of SSRI treatment makes it difficult to generalize from this work to typical clinical populations. The final recent study 47 investigated the effects of psilocybin assisted therapy in patients receiving a concomitant SSRI medication. SSRI treatment did not appear to diminish either the subjective or antidepressant effects of psilocybin, with effects on both being comparable to previous studies in patients who were withdrawn from SSRIs. 48 This suggests that co-administration is safe and may be a useful option in patients where withdrawing current medication may be a concern. Conversely, other recent work on MDMA-assisted therapy for PTSD has suggested that patients who tapered off their SSRI/SNRI usage prior to treatment showed reduced efficacy, relative to subjects who had never taken reuptake inhibitors. 49 This highlights the necessity of future studies that specifically consider the potential for interactions and management strategies for commonly prescribed pharmacotherapies and psychedelics.
Chronic use of SSRIs/SNRIs has been shown to cause down-regulation and desensitization of 5-HT2A receptors, 50 and given that the intensity of psychedelic effects correlates directly with 5-HT2A receptor occupancy in the human brain, 22 it seems plausible that chronic antidepressant use may attenuate the effects of psychedelics. However, these recent studies may indicate a more complex relationship. Evidence for attenuation of acute psychedelic effects is somewhat mixed, and similarly effects of modulation of clinical outcomes are somewhat variable. While recent studies (particularly 36 ) contain many useful measures, including pharmacokinetics, subjective measures, and assessment of downstream pharmacodynamic effects (peripheral BDNF, gene expression, autonomic functions), a key omission is any brain measure of pharmacodynamic effects. The variability in results underscores the necessity of incorporating diverse methodological approaches, including direct brain measures, in future research. This will be crucial in revealing the underlying mechanisms, optimizing therapeutic strategies, and may help to resolve the variable results seen in previous trials. Another potential avenue to explore is co-administration of different psychedelics, a relatively common practice in recreational use where combining, for example, MDMA and LSD is known as “candyflipping.” 51 This combination may be of clinical interest as co-administration of MDMA may help to reduce some of the negative effects (notably, anxiety), however one recent controlled study 52 on this topic found no significant effects of MDMA co-treatment with LSD on subjective effects or adverse events.
Given the key locus of action of (classic) psychedelics at the 5-HT2A receptor, a central method in future clinical investigations of psychedelic interactions is likely to be PET receptor occupancy studies with the relatively novel radiotracer [11C]CIMBI-36.53 -55 PET is an established method for examining drug interaction effects in vivo56 -58 and [11C]CIMBI-36 is relatively selective for 5-HT2A receptors, has high sensitivity to serotonin receptor agonists, and can be effectively used as an index of serotonin release, 59 as well as the effects of psychedelics. 22 One possible study design (similar to Becker et al 36 ) might involve treatment with a SSRI anti-depressant (either acute dosing, or to more accurately model real-world usage, chronic dosing over a period of weeks) followed by an [11C]CIMBI-36 PET receptor occupancy study with a classic psychedelic. Subjects in a second study arm could complete the same protocol except with a placebo treatment, or (for a within-subjects design) baseline (pre-treatment) PET scans could be compared to post-treatment scans collected some weeks later. Such data would provide hard evidence of the modulatory effects of SSRI anti-depressants on the binding behavior (affinity, time-course) of psychedelics at the 5-HT2A receptor. Many of the other useful measures employed in Becker et al 36 (BDNF, gene expression, subjective measures) could also be incorporated, and direct relationships drawn between effects at molecular targets and downstream pharmacodynamic effects.
Exploration of interactions at other receptor sites is feasible by accessing other existing PET radioligands. The monoaminergic neurotransmitter systems are particularly well served by the availability of useful PET ligands for a variety of receptors and transporters (including 5-HT1A, 5-HT1B, 5-HT4, 5-HT6, D1, D2, D3, 5-HTT, DAT, NAT, VMAT2, AADC). Dopaminergic radiotracers such as [11C]-(+)-PHNO60,61 (selective for D3 receptors), [11C]raclopride 62 (D2 receptors), and/or [18F]FDOPA could be useful in characterizing interactions between, for example, MDMA and dopaminergic drugs such as methylphenidate (commonly prescribed for Attention Deficit Hyperactivity Disorder; ADHD 63 ). Furthermore, given that psychedelics putatively mediate therapeutic efficacy through rapidly increasing neuroplasticity, PET studies evaluating markers of synaptic density, such as SV2A,64,65 could help reveal the effect of antidepressant pre-treatment on synaptogenesis and its role in clinical outcomes.
There is currently strong interest in using classic psychedelics to treat addiction of various types, 66 including opiate addiction 67 and alcohol use disorder. 5 Radiotracers such as [11C]-Carfentanil (selective for the mOR) are useful in exploring addiction pathology 68 and could be used to establish the interaction between classic psychedelics and pharmacotherapies commonly used in opiate use disorder including methadone, naltrexone, and buprenorphine. The atypical psychedelic ibogaine is also a potential treatment for addiction 69 (though cardiotoxicity is a serious concern 70 ). Ibogaine has a complex pharmacology including interactions at κ-opioid, μ-opioid, NMDA, and σ-2 receptors. 70 PET investigations using opioid or σ-2 71 ligands could also therefore provide valuable insights into ibogaine’s mechanism of action and its potential interaction with other drugs.
In all these cases, additional techniques would be valuable adjuncts to PET data, and multimodal imaging studies are likely to provide the most comprehensive view of drug actions and interactions. Techniques such as Dynamic-Contrast Enhanced (DCE) MRI may be useful for indexing pharmacokinetic effects (eg, looking at changes in permeability of the blood-brain barrier 72 ), however it is more likely that additional techniques will be focused on pharmacodynamic interactions. Most obviously, PET scans could be supplemented with resting-state fMRI to index putative biomarkers of psychedelic effects such as brain network segregation/modularity13,73 or entropy 74 and their modulation by SSRI co-treatment. A number of other MRI techniques may also be useful including Magnetic Resonance Spectroscopy (MRS), 75 and Diffusion Tensor Imaging (DTI) for examining effects on brain tissue microstructure. 76 Other neuroimaging techniques such as Magnetoencephalography (MEG) and Electroencephalography (EEG) have proved valuable in psychedelic research,10,77 and would likely also be useful in studying psychedelic drug interactions. Additionally, behavioral testing, and relevant clinical assessments will remain important outcome measures in such studies. Such a multimodal study could provide vital information related to drug interactions both at the receptor, and on downstream neurophysiological/systems-level effects. This multimodal/multi-technique approach to investigation of drug-drug interactions at various levels of interaction is summarized in Figure 1.
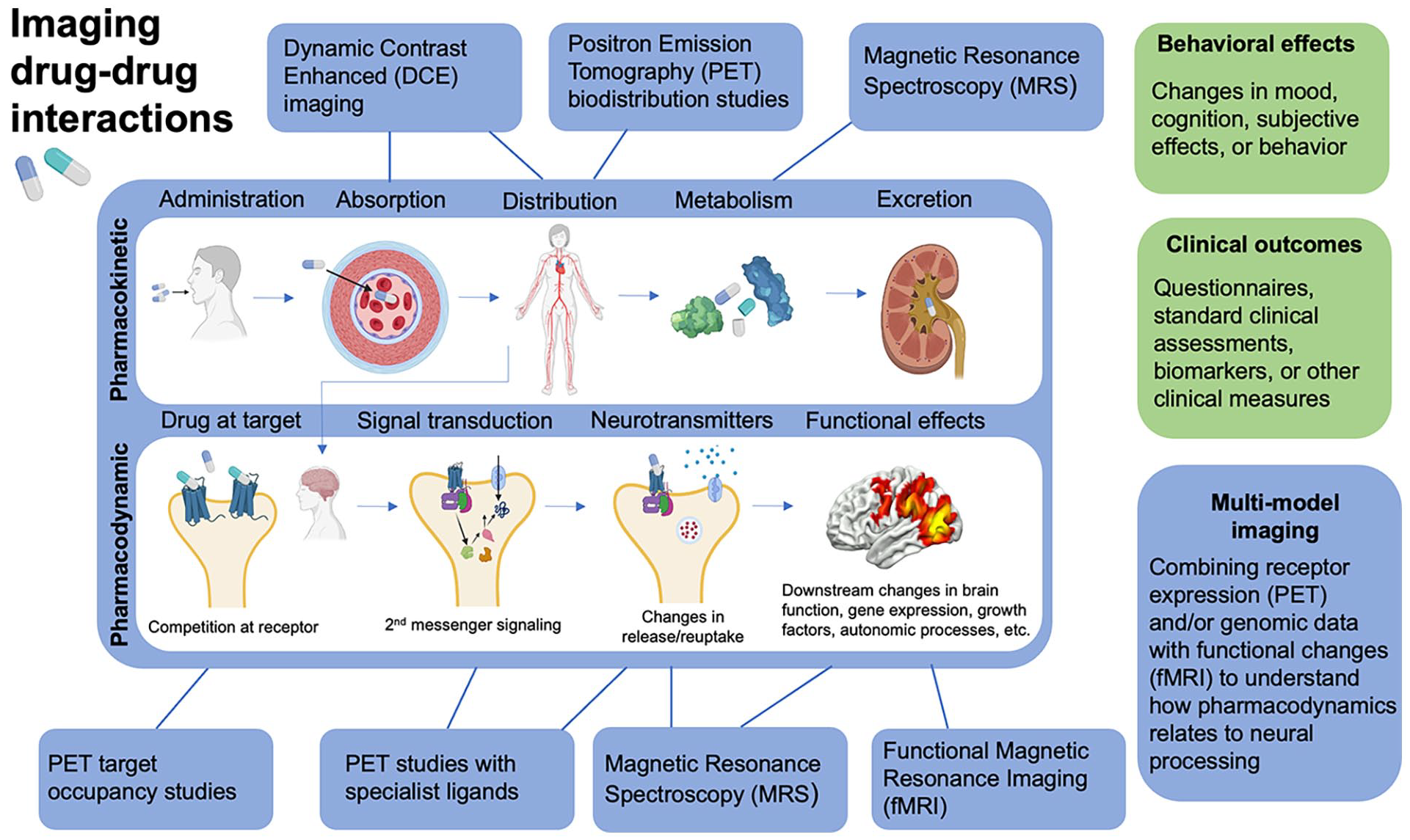
Summary of drug-drug interactions and their locations at different levels of the drug-pathway; pharmacokinetic interactions (center; top row) and pharmacodynamic interactions (center; bottom row). Blue boxes around the edge indicate potential imaging technologies which may be useful measures of the interactions at each level, perhaps in combination with behavioral/clinical measures (green boxes).
Such studies would broadly fall under the rubric of translational research. Much of this work could be performed in groups of healthy subjects, but with a clear focus on applications in the clinic. This would be a clear example of the bi-directional influence of basic science and clinical research 9 where clinical practice (ie, combination therapy) motivates the basic science work (studies of drug interactions), which then iteratively feeds back into clinical research and practice. For example, the PET study design briefly outlined above involving SSRI pre-treatment and a suitable psychedelic would provide hard evidence about receptor-level effects, and additional measures (eg, fMRI/EEG) could provide functional-level information. The results would provide a solid foundation for decision-making on whether to taper off patients from current medication in future clinical trial protocols and, eventually, in clinical practice.
The multimodal neuroimaging studies outlined here have some obvious challenges and limitations. Though perfectly possible, they are certainly technically ambitious and rely on large teams with diverse expertise plus currently cutting-edge technologies (ideally, combined PET/MR scanners) which are not currently widely available. The specific 5-HT2A ligand [11C]CIMBI-36 is also an issue as it has so far only been implemented at two locations (Copenhagen 22 and London 59 ). [11C]CIMBI-36 belongs to the NBOMe (N-methoxy-benzyl) drug class; highly potent and potentially toxic synthetic psychedelic compounds which sometimes appear in the illegal recreational market. 78 As such, NBOMes are legally classified as Schedule 1 in many jurisdictions, which places additional restrictions on the use of [11C]CIMBI-36. Cost is another major barrier, with total cost of many multimodal neuroimaging studies currently running into the (low) millions of dollars; a significant investment for a smaller commercial entity or an academic funding body. PET is also an invasive modality, often involving the placement of an arterial catheter, plus the use of radiation means studies have to be carefully designed and higher numbers of repeated scans may not be possible due to radiation exposure considerations. There are also general pragmatic issues of integrating neuroimaging investigations, perhaps involving several scans/visits on different days, into clinical trial protocols. While many drug-drug interaction studies could potentially be completed using healthy volunteers, there is a clear translational benefit to using patient cohorts in some cases. Most psychedelic clinical trials that have used neuroimaging measures have preferred to follow a pre- versus post-treatment design where scans are conducted at baseline, and then at some point after the therapy sessions.12,79 However, studying drug interactions with psychedelics will likely optimally require scans conducted in the acute dosing phase of the trial, that is, during or alongside the psychedelic therapy session. This is a potential issue with patients who may be unfamiliar with both psychedelics and neuroimaging procedures and may find either or both potentially challenging. Care must be taken in such studies to balance the scientific aims with safeguarding patients when they may be in a vulnerable state, managing anxiety, not overburdening patients with invasive procedures, and minimizing disruption to the psychotherapeutic component of the therapy. 80
The psychotherapeutic component of psychedelic therapy (sometimes explicitly referred to as “psychedelic-assisted psychotherapy”) is deserving of some further discussion in this context. In an important sense, psychedelic therapy has been conceptualized as a combination treatment from its early beginnings in the 1950s, 81 where the drug and psychotherapy components are thought to work in synergy to achieve the therapeutic aims. Studies of drug-drug interactions in the context of psychedelic therapy are therefore adding a third component to an existing dual-treatment model. Broadly, therapy involving classic psychedelics usually favors a non-directive psychotherapy component, often termed “psychological support.” 3 MDMA-assisted therapy makes the inclusion of more explicit psychotherapeutic features possible, as MDMA produces a less profoundly altered state of consciousness. 82 There is currently much debate around the causal role of the psychotherapy component in driving therapeutic change, with some commentators suggesting recently that the drug effects are the primary mechanism, and psychotherapy may only have a minimal role, 83 though this is disputed by others. 84 These are complex issues and outside the scope of this article, beyond noting that there is extensive evidence that psychotherapy itself can bring about measurable changes to brain function. 85 It therefore seems unwise to disregard the psychotherapeutic component of psychedelic therapy in clinical neuroimaging studies though, as noted above, usefully integrating neuroimaging measures into psychedelic clinical trials is an ongoing challenge.
While pre-clinical in vivo and in vitro experiments can provide useful insights, drug-drug interactions investigated in real time in human subjects may be the only way to fully understand the significance of the interactions, particularly on clinical outcomes where pre-clinical models have clear limitations. 23 Other authors have recently advocated for a “precision psychiatry” approach to psychedelic treatment development, 86 possibly by also integrating genomic data with neuroimaging studies. Application of artificial intelligence and machine learning technology is currently at a nascent stage in neuroimaging, but may also have strong potential for developing such an approach. 87 Given that, as noted above, multi-drug combination treatments are a key method for tailoring treatments to individual patients in psychiatry, robust data on drug-drug interactions involving psychedelics in both healthy and clinical populations is a high priority, and a necessary step in providing such a precision approach. Such results will be a vital step in enabling clinicians to safely integrate novel psychedelic-based therapies into existing treatment regimes, and the successful deployment of psychedelic therapies at scale will likely depend on a holistic assessment and the judicious application of results from both basic science and clinically-related research. Multimodal imaging studies can provide highly relevant information at several key levels of drug (inter)action, and thereby build the conceptual molecular-functional-clinical translational bridge necessary to achieve these goals.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MBW wrote the first draft and coordinated the project. All other authors provided edits, additional material, revisions, and other intellectual content.