
Abstract
Neuropsychological symptoms associated with post-COVID-19 conditions may prevent patients from resuming normal activities at home or work. We report a retrospective, cross-sectional evaluation of neuropsychological and cardiopulmonary outcomes in 2 groups of patients: outpatients with mild enough infection to be spared from hospitalization and those who required inpatient admission. We hypothesized a dose-response model of post-COVID symptom severity in which persistent consequences would be more severe in those who experienced worse acute infections. In a dedicated COVID clinic, 321 patients were seen (33% outpatient, 67% inpatient). Outpatients skewed female, White, non-Hispanic, and younger. Outpatients had worse insomnia (measured with insomnia severity index) and were less able to resume their usual activities (EQ-5D-5L usual activities scale), despite inpatients experiencing worse cognition (Montreal Cognitive Assessment), having greater obesity (body mass index), decreased exercise tolerance (6-minute-walk distance), and more exertional oxygen desaturation. In both groups, insomnia worsened while cognition improved significantly with time from infection to testing while controlling for patient age; other variables did not. In logistic regression, female sex, higher MoCA score, EQ-5D-5L “usual activities” subscore, less oxygen desaturation with exertion, and longer time from infection remained as significant associations with outpatient status. Our study demonstrated that the functional sequelae of post-COVID-19 conditions in patients with mild acute disease have the potential to be as severe as that in patients who have recovered from severe illness.
Keywords
Introduction
COVID-19, the infectious disease caused by SARS-CoV-2, has affected more than 100 million Americans as of February, 2023. 1 Post-COVID-19 conditions (PCC), also known as post-acute sequelae of COVID-19 (PASC) or colloquially as “long COVID” comprise a multi-system syndrome of persistent symptoms after resolution of acute infection and include psychiatric, neurological, pulmonary, cardiac, and musculoskeletal complaints. Researchers started to identify lingering neuropsychiatric symptoms after acute infection as early as March of 2020 in a study of patients isolated for mild COVID in Wuhan, China. 2 As defined by the WHO, PCC appears within 3 months from the onset of COVID-19, persists for at least two months, cannot be explained by alternative diagnoses, and impacts everyday function. 3 While estimates of PCC incidence vary widely, recent large population surveys point to PCC in up to 30% of post-COVID patients in the United States.4-6 Neuropsychological complaints are among the more commonly reported in patients with PCC with manifestations including, in estimated order of frequency, fatigue, “brain fog,” insomnia, memory/attention impairment, anxiety, depression, and anosmia.7-9 More concerning for public health, however, is memory and cognitive impairment; significant “brain fog” or memory complaints may affect 20% to 50% of patients with PCC.8,9 Studies utilizing neuropsychological testing have found deficits in memory, attention, executive function, and language in patients with PCC compared to healthy controls.10,11
Several facets of cognitive impairment require further evaluation. First, cognitive impairment may be difficult for patients to report; for example, PCC patients with fatigue and no self-reported cognitive complaints still may demonstrate impaired cognition when assessed with formal testing.9,10 Second, cognitive impairment (and many other symptoms of PCC), are non-specific enough to calculate their incidence difficult. For example, a study using a health care database in the Netherlands matched those with and without a history of COVID infection; of the 25% of patients who complained of some facet of PCC, only 12.7% of patients in the PCC group had symptomatology rise above the incidence of similar symptoms in the control cohort. 12 Third, impaired cognition, like other PCC symptoms, is more severe in those with more severe initial illness; in other words, PCC symptoms should follow a “dose-response” relationship.13,14 In this study, we report the retrospective, cross-sectional experiences of patients seen in a tertiary referral center pulmonary clinic dedicated to post-COVID-19 symptoms. Patients represent the full spectrum of COVID-19 ranging from mild outpatient disease to acute respiratory distress syndrome (ARDS) with prolonged intensive care unit (ICU) hospitalization. Rather than focus on symptoms, we obtained quantitative outcomes in the realms of cognition, function, mood, and pulmonary status. We hypothesize that the severity of post-COVID symptoms will follow a dose-response model with more severe persistent neurocognitive symptoms and functional consequences in those who experienced worse acute infection.
Materials and Methods
Patients
The University of Virginia Institutional Review Board (HSR #22463) determined the study to be exempt from full review. This retrospective, cross-sectional, observational study reports on a cohort of patients seen at the University of Virginia pulmonary-based, post-COVID Clinic between 6/2/2020 and 11/7/2022. Patients were included if they had a confirmed COVID-19 infection and persistent pulmonary complaints, specifically, persistent cough, shortness of breath or dyspnea on exertion. Patients discharged from the University of Virginia Medical ICU were actively recruited for follow-up in the clinic, all other patients were either self- or physician-referred for ongoing symptoms.
Variables
The
The time between COVID-19 confirmation and the initial clinic visit (time from infection) was calculated to control for the effects of interval change in symptoms.
Statistical analysis
Univariate comparisons between outpatients and inpatients were performed with Fisher’s exact tests (categorical data) and Student’s t-tests (continuous data) to provide initial screening. Those variables with alpha P < .05 were evaluated with 2 different statistical models. Those variables with a potential relationship to time from infection were evaluated with linear regression using time from infection as the main independent variable and age as a common covariate. All variables with an alpha P < .05 were used to construct a logistic regression model with the dependent variable outpatient versus inpatient group. Imputation was not performed; only those patients with complete data were included in the regression model.
Results
Univariate comparisons
A total of 321 patients (outpatient: 107, 33%; inpatient: 214, 67%) met the criteria for inclusion. Inpatients were comprised of those admitted to ICUs (152 of 214, 71%) and those who were in the acute care wards (62, 29%).
Demographics differed significantly between outpatients and inpatients (Table 1). Outpatients skewed female, White, and non-Hispanic compared to inpatients. Outpatients were on average 6.3 years younger (P < .001). The 2 groups did not differ by median income by home ZIP code.
Univariate comparisons between outpatients and inpatients.

Statistically significant.
The pooled incidence of cognitive impairment, as determined by MoCA thresholds, was MCI in 33% and severe cognitive impairment in 14%. At least MCI was present in 31% of outpatients and 55% of inpatients (P < .001). The relative proportion of those falling in the dementia range was lower in outpatients (4%) than inpatients (19%) (Figure 1(a)). Mean MoCA scores were higher in outpatients with the mean above the cut-off between normal cognition and MCI, whereas the mean MoCA score of inpatients fell within the MCI range (Table 1).

Distribution of patients by group (inpatient or outpatient) by the presence of (a) cognitive impairment as determined by the Montreal Cognitive Assessment and (b) insomnia as determined by the Insomnia Severity Index ⩾10. MCI = mild cognitive impairment.
Outpatients reported significantly worse insomnia, both by ISI mean scores and by cut-off criteria; 60% of outpatients reported insomnia compared to 45% of inpatients (Figure 1(b)).
Functional status assessed with components of the EQ-5D-5L differed significantly in the “usual activities” component; outpatients reported a significantly higher severity of symptoms that impacted the conduction of usual activities (2.56 ± 1.16 vs 2.21 ± 1.14, P = .026). The other components of the EQ-5D-5L did not significantly differ between the 2 groups. Quality of life scores from the EQ-5D-5L VAS did not differ significantly between groups. Depression and anxiety measured through PROMIS surveys did not differ significantly between the groups. PTSD scores were similar between groups and below the diagnostic threshold for PTSD.
Physical and pulmonary function was significantly better in outpatients compared to inpatients. Mean BMI was lower, the 6 MW distance was farther, and oxygen saturation with exertion was higher in outpatients.
Finally, the latency between infection and assessment was significantly longer in outpatients, about 10 months for outpatients versus 6 months for inpatients.
Regression: Time from infection
The effect of the duration between COVID infection and clinic visits was evaluated (Table 2). Insomnia (ISI) was more severe with greater time from infection, but MoCA scores were higher with greater time from infection while controlling for patient age. The time from infection was not a significant factor with other variables.
Linear regressions of the effect of time between infection and clinic visit with age as a covariate.
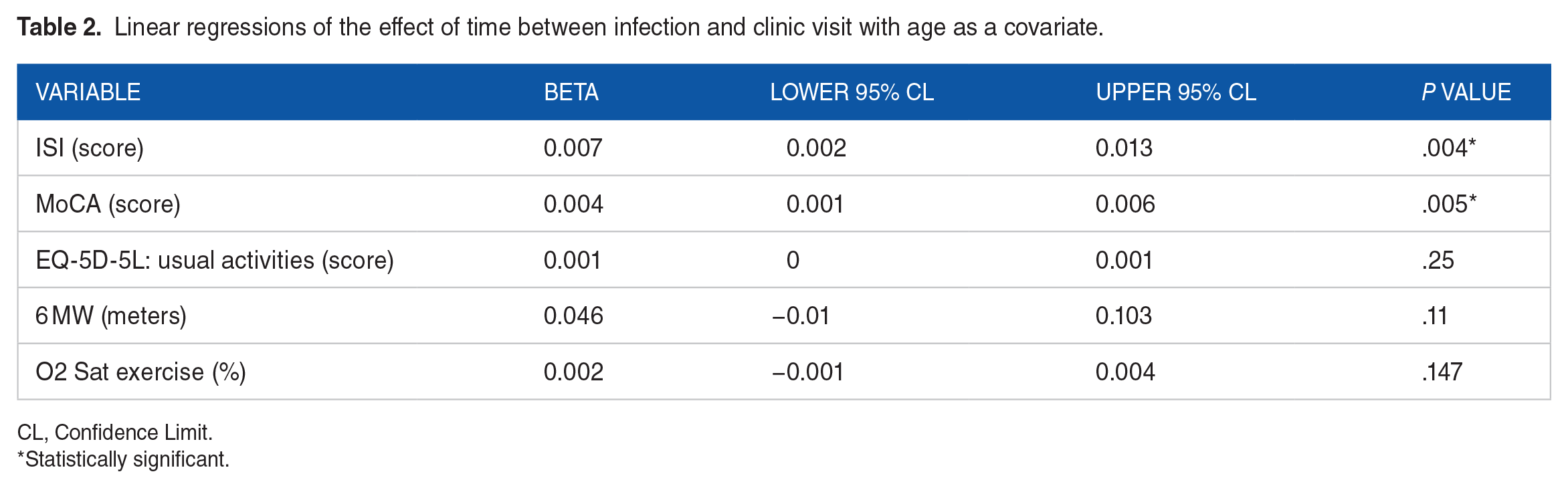
CL, Confidence Limit.
Statistically significant.
Regression: Patient group
From the above variables, a logistic regression model with the patient group as a dependent variable was constructed with sex, race, ethnicity, age, ISI, MoCA, EQ-5D-5L “usual activities” score, BMI, 6 MW distance, and oxygen saturation with exertion (Table 3). Eighty-five outpatients and 98 inpatients (57% of the sample) had valid data for regression analysis.
Logistic binomial regression model of outpatient:inpatient groups as outcomes associated with independent variables with P < .05 brought into the model.

CL, Confidence Limit.
Statistically significant.
Of the above variables, female sex (OR 3.043 [95% CI 1.379-6.713]), EQ-5D-5L “usual activities” score (OR 2.279 [95% CI 1.497-3.791]), higher oxygen saturation with exertion (OR 1.327 [95% CI 1.155-1.525]), higher MoCA score (OR 1.16 [95% CI 1.012-1.329]), and longer time from infection (OR 1.003 [95% CI 1.001 to 1.006]) remained as significant associations with outpatient status while controlling for other variables.
Discussion
The main finding of this retrospective evaluation of patients seen in a tertiary COVID-19 clinic is that outpatients reported equal or worse subjective function after COVID infection despite having markers of better physical, cognitive, and pulmonary health. In multivariate analysis, outpatients had worse insomnia and were less able to complete their usual activities despite worsened cognition, increased obesity, decreased exercise tolerance, and lower exertional oxygen saturation in inpatients. Our findings suggest that patients with milder acute disease nevertheless can present with significant neuropsychological sequelae long after the resolution of acute COVID-19 infection and that these symptoms do not follow a dose-response relationship to initial disease severity. This runs counter to our initial hypothesis that inpatients in our sample would have more severe functional limitations.
The female sex was more prominent in the outpatient group, agreeing with previous studies that demonstrated an increased incidence of PCC in women.5,9,23 PCC shares features with chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) that has been speculated to be a post-viral phenomenon and has a female to male preponderance of roughly 3:1. 24 A German study of 42 patients with post-COVID fatigue found that 45% of their sample met diagnostic criteria for CFS/ME. 25 A Mayo Clinic series demonstrated persistent interleukin-6 elevation—a possible biomarker of CFS/ME—that was more common in women than men in their PCC cohort. 26 Other studies have shown an association between inflammation in the acute phase of COVID and post-COVID depressive symptoms. 23 The similar features of PCC and CFS/ME raises the possibility of shared mechanisms and also may suggest common management strategies for patients with refractory PCC.
Our findings confirm that the common subjective complaints of “brain fog,” memory issues, and impaired attention are supported by quantitative measurements of cognition.7,8 Although inpatients had more severe cognitive impairment as measured by MoCA, about a third of outpatients scored equal to or worse than the MCI threshold. Our findings agree with studies that used the MoCA or larger batteries of neuropsychological measures.10,27-29 In comparison between our findings and meta-analyses centering on the use of the MoCA, our overall incidence of cognitive impairment (MCI or worse) of 47% is lower than the 80% documented in those measured in the subacute period of post-COVID recovery. 30 On one hand, the potential effect of such an incidence (40–80%) of cognitive impairment is large. Our population is, on average, in their fifth to sixth decade of life, and the impressive incidence of cognitive impairment is likely to have significant personal and economic effects. On the other hand, however, cognitive impairment following COVID-19 may be time-limited. While longer time from infection was associated with less severe cognitive impairment, the cross-sectional design of this study and the significantly later time of initial visit for outpatients do not allow for conclusions about trends in cognition over time. Notably, the improvement of cognition with time has been demonstrated in studies using serial testing within the first year after infection. 31
Outpatients reported a greater incidence of insomnia than inpatients in the univariate model, and the severity of insomnia regardless of group significantly worsened with time from infection. Data on the severity of insomnia in the post-COVID setting is sparse, but previous studies estimated rates of moderate-to-severe insomnia in about 30% of patients, which is similar to our population.32,33 Our findings run counter to those in a study that showed that insomnia improved over time. 33 We propose that our patients with continuing symptoms converted from acute to chronic insomnia in accordance with the hyperarousal model of insomnia. 34
Outpatients rated their ability to perform normal functions (as measured by the EQ-5D-5L) worse than inpatients. We were surprised by both the severity of post-COVID dysfunction in our outpatient group as well as the discordance between greater functional disability with lesser severity of physical disability (as represented by longer 6 MW distance and higher oxygen saturation with exertion). Regarding physical disability, our study agrees with previous studies that showed worsened post-acute pulmonary limitations with a more severe initial disease.35,36 Decreased functional ability in those with less severe physical evidence of post-COVID disease is a novel finding. In a study from the UK, the severity of function (based on the COVID-19 Yorkshire Rehabilitation Scale) correlated with a subjective survey measure of overall health. 37 In a Swedish study of healthcare workers who were surveyed after the resolution of their acute COVID symptoms, 11% of seropositive patients reported moderate-to-marked disruption in any Sheehan Disability Scale category (a measure of functional home and work status) as well as having at least 1 moderate to severe PCC symptom lasting for at least 8 months. 38 The main difference between the present study and the 2 cited was that we compared functional status to objective physiological measurements, whereas other studies used either a subjective measure of health or an antibody marker. Our study suggests that functional impairment does not follow the severity of cardiopulmonary sequelae of severe, inpatient COVID infection in lockstep. We propose that the discordance between function and physiological severity may be one reason, as documented in the lay press, why patients with PCC experience difficulties in obtaining disability benefits. 39 Our work emphasizes that the hunt for objective biomarkers of “long COVID” continues. 40
Limitations of our study include that patients with incomplete data decreased the number of patients available for the regression model. Our patients were, on average, younger than the validated age range for the MoCA; our use of the MoCA, however, is consistent with its use in other post-COVID studies.10,29 Referral patterns differed between groups; all outpatients and non-ICU inpatients were self- or physician-referred because of persistent symptoms post-infection, while post-ICU patients were scheduled in the clinic as part of our post-ICU protocol. Our study lacked baseline measurements; however, no patients presented for neurocognitive testing prior to illness, suggesting that patients were not impaired enough to bring them to medical attention.
Conclusion
Neurocognitive complaints were common in a cohort of outpatients and inpatients seen in a post-COVID clinic for persistent pulmonary symptoms. Despite more severe initial infection and objective pulmonary and cognitive impairment in inpatients, outpatients reported worse functional limitations. Our study demonstrated that the severity and functional impact of PCC in patients with mild disease has the potential to be as severe as that in patients who have recovered from severe illness.
Footnotes
Author Contributions
SFO, SAF, JP, AK collected data. MQ, KBE, EMD, and AK performed statistical analysis and interpretation of data. SFO, SAL and JP prepared the manuscript. AK conceptualized the work, and approved final manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.