
Abstract
Background:
Stroke persists as an important cause of long-term disability world-wide with the need for rehabilitation strategies to facilitate plasticity and improve motor function in stroke survivors. Rhythm-based interventions can improve motor function in clinical populations. This study tested a novel music-motor software application ‘GotRhythm’ on motor function after stroke.
Methods:
Participants were 22 stroke survivors undergoing inpatient rehabilitation in a subacute stroke ward. Participants were randomised to the GotRhythm intervention (combining individualised music and augmented auditory feedback along with wearable sensors to deliver a personalised rhythmic auditory stimulation training protocol) or usual care. Intervention group participants were offered 6-weeks of the GotRhythm intervention, consisting of a supervised 20-minute music-motor therapy session using GotRhythm conducted 3 times a week for 6 weeks. The primary feasibility outcomes were adherence to the intervention and physical function (change in the Fugl-Meyer Assessment of Motor Recovery score) measured at baseline, after 3-weeks and at end of the intervention period (6-weeks).
Results:
Three of 10 participants randomised to the intervention did not receive any of the GotRhythym music-motor therapy. Of the remaining 7 intervention group participants, only 5 completed the 3-week mid-intervention assessment and only 2 completed the 6-week post-intervention assessment. Participants who used the intervention completed 5 (IQR 4,7) sessions with total ‘dose’ of the intervention of 70 (40, 201) minutes.
Conclusion:
Overall, adherence to the intervention was poor, highlighting that application of technology assisted music-based interventions for stroke survivors in clinical environments is challenging along with usual care, recovery, and the additional clinical load.
Introduction
Stroke is the third most common cause of death in Australia and a leading cause of long-term disability. 1 More than 50% of stroke survivors report some degree of disability and require long-term assistance and support after discharge from hospital. 2 Clinical and animal studies have shown extensive cortical reorganisation and injury-induced plasticity occurs in the motor areas and corticospinal tract after stroke.2-4 Harnessing these plasticity processes may provide a means of maximising recovery of stroke survivors.5,6
Currently, rehabilitation and interventions for stroke recovery are focussed on intensive motor training, exercise and physiotherapy. Research shows rehabilitation programmes that incorporate the principles of motor learning, such as mass repetition of goal-oriented and task-specific exercises performed at high intensity can induce beneficial plasticity and produce long-term changes in motor function in stroke survivors.7,8
Although beneficial effects have been observed in stroke survivors with intensive motor training, there are several limitations of current therapies and rehabilitation approaches. Chronic stroke survivors are a heterogenous population presenting with a variety of upper and lower extremity impairments and treatment must be tailored to the needs of individual stroke patients. 2 Clinical guidelines now also recommend larger doses of motor training (>2 hours per day), which can be difficult for those with severe impairments and older stroke survivors.9-11 Finally, reduced motivation and low treatment adherence to rehabilitation programmes has been observed in stroke survivors both in hospital and in the community and this is a significant barrier to recovery.12,13 Therefore, there is a need to develop novel therapies that incorporate the effective principles of current treatments to augment training induced plasticity, while maintaining patient motivation and adherence.
Rhythm can entrain and prime neurons in the motor cortex via the rich neural connections between auditory and motor regions,14-21 and numerous studies have evaluated the therapeutic effectiveness of Rhythmic Auditory Stimulation (RAS) and music-based therapies in various clinical populations, with growing evidence that RAS can improve motor outcomes in stroke survivors.22-31 RAS, in addition to other benefits, can improve different gait parameters such as stride length and walking symmetry in stroke survivors.24,25,28,32-39 RAS has also been shown to improve neuromotor control, enhance stability and increase walking speed in people with chronic stroke.29,33,40 Meta-analyses on RAS for post-stroke recovery of upper-extremity function has demonstrated rhythmic cueing can enhance strength, elbow range of motion, synchrony, finger dexterity and co-ordination, and overall upper limb function in stroke survivors.41,42 The psychosocial benefits of listening to music during exercise and rehabilitation have been well documented, with many studies reporting the positive impact of music on motivation and endurance in exercise regimes for both healthy and stroke-affected populations.43,44 Music within rehabilitation can also improve patient mood, enhance the affective experience of therapy and increase enjoyment of exercise, which may allow patients to maintain motivation.32,45-47
Digital therapeutic technology has the potential to improve long-term motor outcomes after stroke by providing stroke survivors with independent access to individualised and targeted interventions after discharge from hospital and other rehabilitation services, or to use as an adjunct therapy in addition to physiotherapy and other rehabilitation sessions.31,48 Currently, few mobile software applications have been developed, and researchers cite multiple barriers to integration into rehabilitation protocols.49,50 We therefore developed a low-cost and accessible iPhone software application (app) that can be combined with wearable sensors to address this gap: ‘GotRhythm’. GotRhythm is a novel music-motor training app that integrates personal music, wireless wearable sensors and real-time auditory feedback via a metronome to deliver a tailored RAS protocol. GotRhythm also provides high-resolution recording of each person’s motor performance throughout training that can be used to monitor progress during rehabilitation. This randomised controlled trial was designed to test the feasibility and effectiveness of a 6-week GotRhythm intervention on motor function compared to conventional rehabilitation in sub-acute stroke survivors undergoing rehabilitation on a stroke rehabilitation ward.
Methods
Ethics
The research study was approved by the Royal Perth Hospital Human Research Ethics Committee (2017/188; RGS0000000044). All participants (and next of kin or people responsible for participants) were provided with a written information sheet, a simplified written summary of the information sheet designed for people experiencing communication impairments, and verbal information about the study. The study was prospectively registered (ACTRN12617000488303). All participants provided written informed consent.
Design
Single blind randomised controlled trial.
Setting and participants
Participants were recruited from a public sub-acute stroke rehabilitation unit at a hospital in Perth, Australia. Inclusion criteria included participants >18 years undergoing rehabilitation after stroke (subacute stage: 0-180 days following initial stroke) and whose clinical staff judged were likely to be inpatients ⩾6-weeks. Exclusion criteria included severe joint pain, impairment, other than from stroke, that prevented participant’s ability to complete the protocol, or unstable co-morbid medical or psychiatric disease. Patients had no severe cognitive impairment as assessed by clinicians on the stroke rehabilitation unit.
Randomisation
Consenting participants were randomised using a computer-generated sequence of numbers and sealed opaque envelopes (Figure 1).
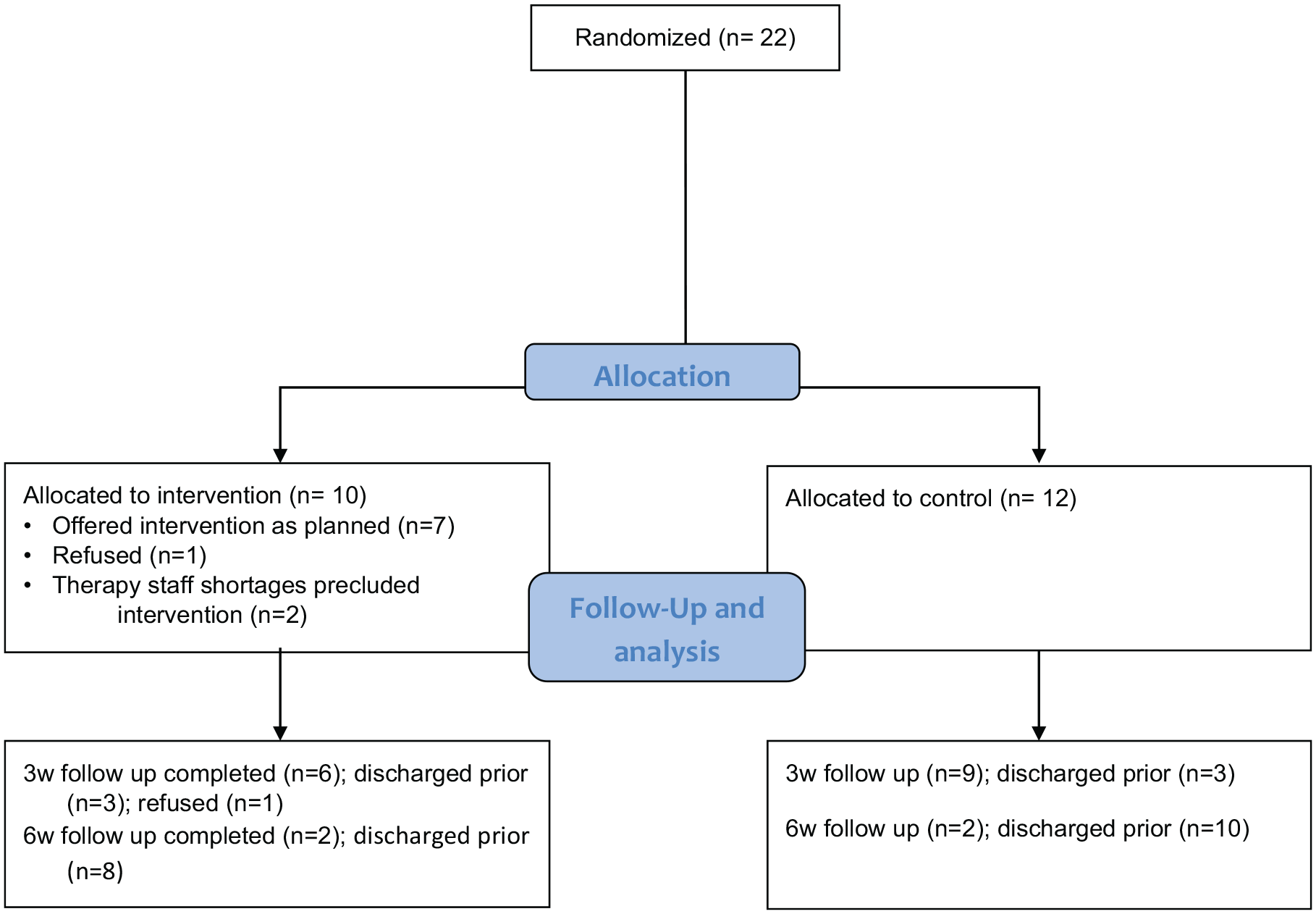
Participants were randomly allocated to an intervention (n = 10) or control (n = 10) group.
Intervention
GotRhythm is a mobile phone-based app used to deliver individualised music-motor therapy to stroke survivors and provides feedback on motor performance. GotRhythm was provided on an iOS device (iPhone 5, Apple Inc., CA). GotRhythm training was tailored to a participant’s specific injury in consultation with their hospital clinicians. The training took place under supervision at the hospital’s stroke rehabilitation clinic, and training was in addition to the usual stroke rehabilitation programme recommended by their clinician. GotRhythm supports a wide array of sensors to detect a variety of physical activities, including both upper and lower limb movements, as well as gross and fine motor skills. A series of participant-specific movement tasks focussing on different affected body parts were selected to match the rehabilitation goals of each patient.
Patients wore non-intrusive sensors (wireless inertial motion units [IMU]; Mbientlab Inc., San Francisco, CA) on the relevant body part that link wirelessly to the app. The IMUs wirelessly transmit acceleration, gyroscope and magnetometer data at a rate of 100 Hz to the GotRhythm app. GotRhythm converts the raw sensor data into attitude angles (yaw, pitch and roll) in real time. Clinical staff configured the start and end point angles in GotRhythm for the chosen attitude (eg, yaw). For example, GotRhythm is configured for periodic upper arm movement from 0° (parallel to the ground, start point) to 45° (end point). One complete cycle through this range of movement corresponds to a ‘beat’, and the aim is to match the beats to the target beats per minute (BPM). The allied health professional in charge of the patient’s rehabilitation prescribed the GotRhythm training by assigning a suitable target rhythm using BPM for each patient. The initial tempo was matched to the patient’s baseline movement frequency where patients were instructed to move at a comfortable pace. Tempo was adjusted in each session to suit each patient’s abilities, such as increasing the BPM as patients’ function improved, and progressively attuned to any changes in the patient’s rehabilitation needs over the intervention period. The tolerance band (the acceptable tempo range the participant could move within) was also adjusted to suit the patient’s abilities. For example, a target BPM of 60 with a tolerance of 3+/−, results in an acceptable tolerance range of 57 to 63. Music was selected based on participant’s personal preferences: 8 to 10 songs were selected with an approximate overall playtime of 30-minutes. GotRhythm changes the tempo of the music to the defined target BPM in real time without any change in pitch. During each intervention session, participants were instructed to move to the beat of the music. When the participant’s movements deviated from the selected tempo range, the music was silenced and replaced with a metronome playing at the pre-selected target tempo. The metronome provided real-time auditory feedback until the participant moved again within the target tempo range.
Intervention group participants were offered 6-weeks of the GotRhythm intervention, consisting of a supervised 20-minute music-motor therapy session using GotRhythm conducted 3 times a week for 6 weeks. The GotRhythm programme consisted of a warm-up, preparatory activities (BPM/movement selection), main activities and cool down led by their clinician. Participants were able to stop, and rest whenever required.
The target for total sessions was 18 sessions (ie, 360 minutes of intervention in total). These sessions were planned to be conducted on Monday, Wednesday and Friday of each week.
Control group participants’ usual care stroke rehabilitation was unchanged during the study, with no additional music-motor therapy.
Outcomes
Adherence to intervention. Clinicians recorded the length of time each patient engaged with the app in logbooks provided by the research team.
Change in Fugl-Meyer Assessment (FMA) of Motor Recovery score from baseline.
The FMA is a stroke-specific, performance-based impairment index that evaluates upper and lower limb motor function, balance, sensation and joint functioning in patients following stroke with excellent inter- and intra-rater reliability.51-54 The motor domain includes items measuring movement, co-ordination and speed and reflex action of the shoulder, elbow, forearm, wrist, hand, hip, knee and ankle. Items were scored on an ordinal scale of 0 (cannot perform, absent), 1 (partial impairment), and 2 (no impairment). Overall motor scores range from 0 (hemiplegia) to maximum of 100 (normal motor performance), with 66 points assigned for the upper extremity and 34 points for lower extremity. Participants were assessed with the FMA at baseline, after 3-weeks and at end of the intervention period (6-weeks). Assessments were conducted by a trained member of research team. Assessors were masked to participant group allocations.
Sample size and data analyses
For this feasibility pilot study a sample size of 20 participants (n = 10 intervention group) was sought, informed by previous stroke intervention studies,55-58 as this would be likely to be adequate to assess the primary outcome of adherence to the intervention.
Results
Adherence to the intervention
Overall, adherence to the GotRhythm intervention was limited. Three participants randomised to the intervention did not receive GotRhythm. Despite providing informed consent 1 participant declined to engage with the intervention and no intervention sessions were attempted. For 2 participants clinical staffing shortages precluded provision of the GotRhythm intervention as planned.
Of the 7 participants who engaged in the intervention in the first 3-week intervention block, only 5 completed the 3-week mid-intervention assessment (1 participant was discharged before undergoing their 3-week assessment and 1 refused). Only 2 of the 10 intervention participants were still inpatients, completed some intervention for the second 3-week intervention block, and completed the 6-week post-intervention assessment.
Recording of data in the app, which requires recordings to be manually started and stopped, also appeared to be inconsistent. For 5 of the 7 participants who received the GotRhythm intervention, use of the app according to the study logs exceeded actual recordings in the app, suggesting that the manual step required to initiate recording in the app had not been completed.
The intervention was intended to deliver three 20 minute sessions in each of two 3-week blocks, that is a total of 180 minutes across 9 sessions for block 1, and a further 180 minutes across 9 sessions in block 2. Overall, the 7 participants were logged to use the GotRhythm app for 70 (IQR 40, 201) minutes in 5 (4, 7) sessions however app recordings only validated use for 19 (0, 34) minutes in 3 (0, 4) sessions.
The actual number of sessions attempted varied widely – from minimum 3 to maximum 8 (of 9 intended) sessions in the first 3-week block and from minimum 1 to maximum 6 (of 9 intended) for the 2 participants continuing in the second 3-week block. The 2 participants who remained inpatients and engaged in both blocks of the intervention completed 14 sessions (201 minutes) and 7 sessions (142 minutes) of the intended ‘dose’ of 18 sessions and 360 minutes. The duration of sessions was also very variable ranging from 4 minutes (of the intended 20 minutes) up to 30 minutes.
Change in FMA scores
Fugl-Meyer assessment results are presented in Table 1. Upper limb scores improved at 3-week follow-up in both intervention and control groups.
Participant characteristics and Fugl-Meyer Assessment scores at baseline, 3 and 6 weeks.

Clinician feedback
Feedback provided by 2 clinicians (ward therapists) suggested it may be easier to have a shorter intervention session every day (rather than a 20 minutes session on 3 days of the week). Time required for study assessments was perceived to be at the expense of ‘usual’ therapy time. Therapists cited difficulty ensuring availability of clinical staff to implement the intervention and assist research staff and participants. It was also perceived that the research intervention tended to be added onto usual therapy and thus performed later in the day when participants may have been more fatigued. Participants were perceived to enjoy the music but, despite that, to become bored by repetitive movements.
Discussion
Main findings
Overall, adherence to the intervention in practice was poor. Although the concept of rehabilitation using RAS for stroke survivors remains attractive, in practice, designing an effective and engaging intervention has many challenges, even when supported by clinical staff.
Results in context
Studies of music-motor therapy have occurred in a range of settings and with heterogenous goals. The dosage we chose (3 sessions per week for 6 weeks) in the current study is lower than some previous studies, although interventions delivered 3 days a week for 3 to 6 weeks have led to small but significant improvements in movement.59,60 The clinicians’ suggestion for daily therapy is consistent with previous research that has primarily used higher dosage with daily application, 5 days per week for 3 to 6 weeks, and led to statistically significant changes in motor function.22,24,26,33,39,61-64
Strengths/limitations
Interpretation of our data is limited by the small number of participants, frequent losses to follow up and incomplete recording of data in the app itself, limiting the conclusions that can be drawn. Future revisions of the app should avoid the requirement for manual initiation of recording of data in the app to ensure the total time spent training during each session and participants’ performance across the training period can be assessed. Participants were heterogeneous (with varied levels of impairment) and future studies may more clearly define a target population.
Conclusions
This pilot suggests that future studies of RAS in inpatient stroke survivors will require resourcing for delivery of the intervention, and recording of data, by research, rather than clinical, staff and be carefully designed to maximise adherence to the intervention.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Neurological Research Program (NRP) and Royal Perth Hospital Medical Research Foundation.
Declaration of Conflicting Interests:
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to study conception and design and provided critical revisions. CEB analysed the data. KH was involved in data acquisition, data intepretation and drafted the manuscript.