
Abstract
Hypertrophic olivary degeneration is a rare condition caused by a lesion in the Guillain-Mollaret triangle which leads to trans-synaptic degeneration resulting in the degenerative hypertrophy of the inferior olivary nucleus. This condition presents clinically with palatal tremor but can also produce ocular myoclonus or cerebellar signs. While any lesion that occurs within the Guillian-Mollaret triangle and results in the deafferentation of the inferior olive can lead to hypertrophic olivary degeneration, the most common etiologies include ischemic and hemorrhagic stroke, vascular malformation, neoplasm, and iatrogenic injury related to surgery. We report a series of 7 patients who presented with this condition bilaterally on MRI imaging, including 1 case which represents the first report of toxoplasmosis leading to the development of bilateral hypertrophic olivary degeneration and only the third reported case, unilateral or bilateral, related to an infectious etiology.
Keywords
Key Points
Hypertrophic olivary degeneration is a rare condition caused by a lesion in the Guillain-Mollaret triangle
The majority of reported HOD cases are Bilateral as opposed to unilateral
The most common etiologies include ischemic and hemorrhagic stroke, vascular malformation, and neoplasm.
Background Information
Hypertrophic olivary degeneration (HOD) is a rare disorder in which damage to the brainstem or cerebellum leads to degenerative hypertrophy of the inferior olivary nucleus (ION). The condition was first described at autopsy by Oppenheim. 1 Oppenheim’s initial report was confirmed by additional authors in the early 1900s and the pathophysiology underlying the condition described by Foix et al in 1926.2,3 According to Foix et al’s 3 description of “trans-synaptic degeneration,” neuronal alterations and eventually cell death may be caused by the loss of synaptic input which occurs after an insult to the afferent fibers. In 1931, Guillain and Mollaret further expanded upon the work of Oppenheim and Foix by providing a detailed description of the anatomic network implicated in HOD—the dentato-rubro-olivary pathway, which was later named the Guillain-Mollaret triangle. 4 This triangle is made up of afferent fibers from the dentate nucleus which ascend through the dentatorubral tract before synapsing on the contralateral red nucleus. Following this, the afferent fibers of the red nucleus descend through the central tegmental tract to the ipsilateral ION. Any lesions along the previously described portions of the triangle from the dentate nucleus to the ION can cause HOD. The final leg of the triangle involves the olivodentate fibers which originate from the ION and ascend to the contralateral dentate nucleus. These olivodentate fibers are not involved in HOD, because they arise from the ION and provide synaptic output from the ION, so their interruption will not lead to trans-synaptic degeneration of the ION. Clinically, the most commonly described feature of HOD is palatal tremor. Clinical presentations have also been reported to include Holmes (dentatorubral) tremor as well as ocular myoclonus. These clinical manifestations are thought to be secondary to the loss of inhibitory input to the ION and the resultant hyperactivity of the olivary neurons. 5
Previous studies have described both unilateral and bilateral HOD from multiple causes including stroke, cavernous hemangioma rupture, surgical injury, neoplasm, and multiple sclerosis.6-10 In this review, we intend to elucidate the complex gross anatomy of the rubro-olivary dentate tract (ROD). We then review the imaging anatomy of the ROD and medullary brainstem. Finally, we address the current understanding of HOD pathogenesis and imaging findings of patients with HOD on MRI.
Methods
Following Institutional Review Board approval of this research study, all cases included in this retro-respective review were identified using mPower (Nuance, Burlington, MA, USA) natural language processing software to search for “hypertrophic olivary degeneration” within the radiology reports generated at our institution from 2014 to present. The images were then reviewed by 2 radiologists with certificate of added qualification (CAQ) in neuroradiology who confirmed the diagnosis of bilateral hypertrophic olivary degeneration.
Imaging acquisition
All images were acquired using a 1.5 T MR imaging scanner (Magnetom Avanto; Siemens, Erlangen, Germany) with a slew rate of 125 T/m/s and an 8-channel head array coil. The MR imaging protocol included the following sequences: axial FLAIR, axial T2-weighted, axial T1- weighted, and axial diffusion-weighted MR imaging in all patients. Postcontrast T1WI was performed in all 7 patients. Susceptibility-weighted imaging was performed with the following parameters: FOV 230 mm × 190 mm × 130 mm (anterior-posterior × right-left × height-feet), voxel size 0.6 mm × 0.6 mm × 1 mm, reconstruction matrix 960, TE/TR 7.12/31 ms, flip angle 20° with no water or fat suppression used (1.5 T MR imaging unit, Avanto).
Results
Case 1
A 57-year-old male with a past medical history of hypertension presented to our institution with slurred speech and decreased mental status (Table 1). Initial workup revealed findings consistent with an acute basilar-territory ischemic stroke, involving the artery of Percheron (Figure 1). Following the initial acute hospitalization for stroke management, the patient was discharged home. On routine 1-month follow-up examination in the stroke clinic, dysconjugate gaze and hypophonic slurred speck were noted upon physical examination. Follow-up MRI at this time demonstrated encephalomalacia within the bilateral thalami, midbrain, pons, bilateral cerebellar hemispheres related to prior basilar infarct. In addition to these findings, there was increased T2 signal noted in the bilateral ION without evidence of contrast enhancement.
Etiology and findings of patients with HOD.

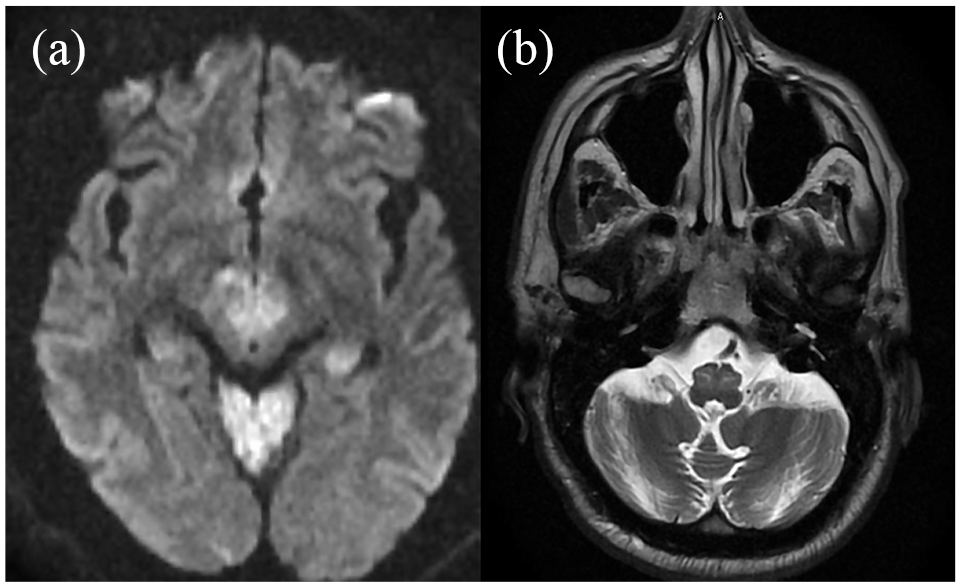
(a) A 57-year-old male who initially presented with restricted diffusion of territories consistent with a stroke involving the basilar artery and the artery of Percheron and (b) 1-month follow-up MRI demonstrated bilateral T2 hyperintensity of the ION.
Case 2
A 37-year-old female initially presented to our institution with a massive pontine hemorrhage extending into the midbrain and medulla secondary to a cavernous malformation (Figure 2). The patient was left with significant left-sided weakness and eventually required tracheostomy and percutaneous endoscopic gastrostomy (PEG) placement prior to discharge. Following the acute phase of her care, she was discharged to a skilled nursing facility (SNF). After her discharge to a SNF, she continued to follow-up with her stroke neurologist. She continued to improve clinically, eventually progressing to the removal of tracheostomy and feeding tube. An MRI obtained 6 months following her initial injury revealed increased T2 signal localized within the ventral medulla bilaterally, without associated enhancement.

(a) Initial gradient echo sequence of a patient who presented with pontine cavernoma rupture demonstrating and (b) a 6-month follow-up MRI (FLAIR sequence) demonstrating bilateral T2 hyperintensity in the inferior olives.
Case 3
A 52-year-old male with a past medical history of hypertension, crack cocaine abuse, and HIV (not on anti-retroviral therapy) with CD4 count of 315 cells/ul, who lived at a drug rehab facility, presented with left-sided weakness, numbness, and facial droop. MRI of the brain obtained during the acute inpatient hospitalization demonstrated a subacute infarct of the posterior limb of the right internal capsule in addition to multiple foci of leukomalacia involving the supratentorial white matter and brainstem (Figure 3). Follow-up MRI obtained 2 months after initial presentation demonstrated swelling of the bilateral ventral medulla with corresponding rounded T2 hyperintensities consistent with a diagnosis of bilateral HOD.

Initial (a) and 2 months follow-up MRI of a 52-year-old male with HIV and crack cocaine use who presented with sub-acute strokes and leukomalacia, demonstrating bilateral FLAIR hyperintensities and fullness of the bilateral ventral medulla (b).
Case 4
A 26-year-old male with a past medical history of motor vehicle collision 10 years prior and resultant post-traumatic epilepsy and cerebellar outflow tremor presented to our institution in Mach of 2019 with complaints of multiple breakthrough seizures. He had no acute changes noted upon physical examination at the time. After titration of his anti-epileptic medication, an MRI of the head was obtained. The MRI revealed moderate T2 lengthening in the bilateral ION, consistent with bilateral HOD (Figure 4).

(a) A 26-year-old male who presented following remote trauma was found to have multiple lesions consistent with a history of high-grade diffuse axonal injury, including lesions best visualized on susceptibility-weighted sequences located in the right dentate nucleus and (b) increased T2 signal in the bilateral inferior olives.
Case 5
A 44-year-old male presented for outpatient follow-up of a previously diagnosed central pontine hemorrhage in 2013 (Figure 5). At the time of discharge, the patient had residual right-sided weakness. A follow-up MRI brain was obtained in the stroke neurology clinic 6 weeks following the initial hemorrhage. The MRI revealed increased T2 signal bilaterally in the ventral medulla, consistent with bilateral HOD.

(a) A 44-year-old male presented with central pontine hemorrhage, extending into the bilateral middle cerebellar peduncles and (b) bilateral FLAIR hyperintensity of the ventral medulla in the same patient on 6-week follow-up MRI.
Case 6
A 54-year-old female with a past medical history of HIV presented in November of 2017 for evaluation of headache and abnormal gait with a CD4 count of 220/ul. Initial evaluation with brain MRI with/without contrast revealed one ring enhancing lesion within the right caudate head and one ring enhancing lesion within the right thalamus (Figure 6). Additionally, a few small ring enhancing lesions, 0.9 cm × 0.3 cm, in the bilateral superior cerebellar peduncles were noted. The imaging finding and laboratory testing of blood for anti-toxoplasma IgM and IgG antibodies via ELISA confirmed a diagnosis of Toxoplasmosis. Following the initial diagnosis, the patient was initiated on a course of pyrimethamine 25 mg tablet twice daily for 60 days. A follow-up MRI brain was obtained 6 weeks following her initial hospitalization to assess the progress of treatment. The MRI brain demonstrated resolution of the enhancement within the right thalamus and an improving appearance of the bilateral enhancing lesions in the superior cerebellar peduncles, suggestive of improving central nervous system (CNS) toxoplasmosis. On this follow-up MRI, new bilateral T2 hyperintensities without enhancement were noted within the bilateral ventral medulla, concordant with the diagnosis of bilateral HOD.

(a) contrast-enhanced MRI of a 54-year-old, HIV positive female who presented with headache, demonstrating a contrast-enhancing lesion that appears to involve the posterior pons and both superior cerebellar peduncles, (b) T2 FLAIR sequence demonstrating significant edema associated with multiple contrast-enhancing lesions in a patient with CNS toxoplasmosis, and (c) follow-up MRI was obtained 6 weeks later that demonstrates bilateral fullness with associated T2 hyperintensity at the level of inferior olives.
Case 7
A 28-year-old male was initially diagnosed with cerebellar medulloblastoma and underwent open surgical resection in May of 2018, which was followed by proton beam radiation therapy to the neuroaxis, with an additional boost to the tumor site. The administered radiation therapy dose was 23.4 Gy, with posterior fossa boost to a total of 30.6 Gy. He presented to the outpatient radiation oncology treatment in August 2018 for evaluation of abnormal lab values, low testosterone and low thyroid levels, with concern for adverse radiation effects. At the clinic visit, the patient reported no new symptoms and no changes in the physical exam were noted. An MRI brain, 6 months post-operation, was obtained which demonstrated rounded areas of increased T2 signal within the ventral medulla bilaterally, consistent with bilateral HOD (Figure 7).

(a) A 28-year-old male underwent resection of medulloblastoma with initial post-operative MRI revealing trace blood products on susceptibility-weighted sequences and (b) 6-month follow-up MRI showed bilaterally increased T2 signal as well as increased fullness at the level of the ventral medulla, consistent with bilateral HOD.
Discussion
We present 7 cases of patients with bilateral hypertrophic olivary degeneration. Many etiologies of HOD have been previously described.9-11 To our knowledge, ours is the first series to report the development of HOD bilaterally due to an infectious etiology such as toxoplasmosis. Only 3 other cases have been reported in the literature describing the association of an infectious etiology with the development of HOD.11-13 One such case involved the development of unilateral HOD following disseminated Listeria infection which resulted in numerous brain abscesses. 13 The remaining 2 cases described the development of unilateral HOD following acute Toxoplasmosis infection.11,12
Previous studies have sought to elucidate the pathological changes that lead to HOD as well as the correlating imaging findings on MRI. Goto et al14-16 undertook post-mortem examinations of patients who had suffered pontine hemorrhages and then subsequently died at varying lengths of time following their injury. From this study, Goto et al14-16 described distinct stages of the development of HOD characterized by no significant changes for the first 24 hours, subtle degeneration of the ION at 2 to 7 days, mild ION hypertrophy without glial reaction at 1 to 3 weeks, hypertrophy of astrocytes and neurons from 8 months to approximately 3 to 4 years, followed by olivary atrophy. Recent reports examining the MRI changes associated with HOD have described a series of imaging changes that correlate with these pathological stages of degeneration. The MRI changes characteristic of HOD occur in 3 stages: (1) increased T2 signal in the ION without hypertrophy (within 1 month of inciting event), (2) persistently increased T2 signal with associated hypertrophy (6 months-3 years from ictus), and (3) atrophy of the inferior olive with persistently increased T2 signal (greater than 3 years following the inciting event).
From the first description by Oppenheim to its characterization by Guillain and Mollaret, HOD has been characterized as a typically unilateral lesion that results from a discrete insult along the afferent input pathways to the ION (Figure 8).1-4 The majority of literature surrounding this disease has been composed of case reports and small case series, the majority of which have highlighted the apparent predilection for the development of unilateral HOD.8,11,12,17,18 Recently, authors from large tertiary referral centers have published retrospective series of all patients who were diagnosed with HOD; revealing a significant percentage of cases are actually bilateral.9,10 Contrary to what would be expected given our current understanding of the pathogenesis of HOD, these studies showed that in 2 series of 102 and 95 patients, 76% and 59% of all cases showed bilateral findings, respectively.9,10 Additionally, these studies, as well as other smaller case series have all reported significant proportions of HOD cases without an identified causal lesion. In the 2 previously described studies, the proportion of patients without an identified etiology was 52% of patients with bilateral HOD vs 13% with unilateral HOD in one study and 50% vs 25% of bilateral vs unilateral patients in the second study.9,10 In this case series, 100% of the presented patients have bilateral HOD with relatively clear associated lesions. Out of identified lesions, the bilateral central tegmental tract was perceived to be the most common lesion location accounting for 57% of the cases. Bilateral superior cerebellar peduncles and bilateral temporal lobes were also among other identified lesion locations. Clearly, if only strict anatomic lesions confined to the triangle of Guillain and Mollaret were able to cause HOD, the larger studies and case series would reflect a preponderance of unilateral or bilateral cases with clearly identified lesions. Likely, one of two explanations is possible, either: lesions reported in other clinical series are detected in later stages of HOD formation or there are lesions causing bilateral HOD that are outside the resolution of clinically available MRI, or the range of lesions that can cause HOD is not confined to the dentate-rubro-olivary triangle. Our case series favors the explanation that the majority of lesions are identifiable and possibly within the direct pathways which may produce secondary effects on the triangle of Guillain and Mollaret; leading to the same end-effect of trans-synaptic degeneration of the ION, just from an injury further upstream in the pathway.

Triangle of Guillain-Mollaret.
Hypertrophic olivary degeneration is a rare clinical entity that is defined by pseudohypertrophy of the inferior olive following an injury to the afferent fibers which comprise the Guillain-Mollaret triangle. This can occur with or without an identified causative lesion and can occur unilaterally and bilaterally. As in our series, larger series have found bilateral cases to be more common. Several etiologies have been implicated in the development of hypertrophic olivary degeneration; however, our series is the first to report the development of this finding bilaterally due to an infectious cause, Toxoplasmosis. In the follow-up of patients with previously identified cerebellar or brainstem pathology, regardless of etiology, clinicians should pay careful attention to the inferior olive for the delayed development of this rare pathology.
HOD in the pediatric population
HOD has also been reported in the pediatric population in multiple literature reviews. However, the number of reported cases in pediatrics is far less common than reported cases in adults. Among reported cases, the vast majority are bilateral HOD with identifiable lesions. 19 The majority of reported cases in this population are secondary to posterior fossa syndrome following brain tumor resection. 20 Children appear to have more clinical symptoms compared to their adult counterparts. 20 Our case series does not include any pediatric patients and there seems to be a paucity in literature considering very minimal reported cases in this population.
Conclusion
Hypertrophic olivary degeneration is a rare pathology that has been reported to be caused by multiple etiologies that cause discrete lesions within the triangle of Guillain-Mollaret. The literature highlight that the reality is often n less well-delineated, with a significant proportion of cases caused by lesions either outside the triangle of Guillian-Mollaret or below the resolution of MRI imaging. Our case series, however, favors Our case series favors the explanation that the majority of lesions are identifiable and possibly within the direct pathways which may produce secondary effects on the triangle of Guillain and Mollaret. Given the diagnostic variability, as well as the low clinical utility of symptoms or exam findings in diagnosing HOD; the neuroradiologist should maintain a high index of suspicion for the development of HOD when reviewing follow-up MRI imaging of patients, especially those with previously diagnosed pathology involving the infra-tentorial compartment.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
All authors were involved in writing and conducting this research.
Ethics Approval and Consent to Participate
Institutional Review Board approval of this research study, all cases included in this retro-respective review.
Consent for Publication
Consent for publication has been obtained from our institution and the patients involved in this study.
Availability of Data and Material
All of our used resources are available in our database.