
Abstract
The COVID-19 pandemic transformed the delivery of healthcare across the world. Telehealth has emerged as the primary method for providing healthcare early in the pandemic. Patient and healthcare provider views of the effectiveness of telehealth services are encouraging and support the long-term use of telehealth services in clinical practice. Telehealth may provide a strategy that has far-reaching benefits for diverse patient populations, such as patients with Batten disease and other rare diseases, who face additional barriers to accessing subspecialty healthcare services. The aims of this paper, through the experience of a single Batten Disease Center of Excellence, are to (1) review the benefits and barriers involved in the delivery of telehealth services to patients with rare diseases; (2) discuss components of a model for clinical care that utilizes telehealth services for patients with Batten disease; (3) discuss limitations and future directions of using telehealth in patients with rare diseases. Healthcare systems should consider building clinical models that utilize telehealth services to provide multidisciplinary services to patients with rare diseases. There are numerous benefits in using telehealth that can enhance and expand service delivery between the patient and clinician. Telehealth services can also improve provider-to-provider communication and collaboration when providing clinical care to individuals with rare diseases. Although there are many benefits to utilizing telehealth services in provision of care to patients with rare diseases, it is important to consider factors that may limit or add additional barriers prior to implementing telehealth services. There is a need for future collaborative research to examine and compare the effectiveness and outcomes of telehealth services with standard of care services that are provided in-person. Future research should also examine how to reduce the challenges and barriers associated with the implementation of telehealth services.
Plain language summary
Telehealth is defined by the US Department of Health Resources and Services Administrations1 as the “use of electronic information and telecommunication technologies to support long-distance clinical healthcare, patient and professional health-related education, public health, and health administration. Technologies include video conference, the internet, store-and-forward imaging, streaming media, and terrestrial and wireless communication.”
This review was conducted to guide a clinical model using telehealth services for patients with Batten disease and other rare diseases based on the experiences of a single Batten Disease Center of Excellence.
Individuals with rare diseases may face multiple barriers to accessing clinical services. Local doctors and treatment providers, such as speech therapists, occupational therapists, physical therapists, and psychologists, may not have knowledge of rare diseases or how to manage symptoms and disease progression, or how to guide treatment services. Other barriers may also include:
• Lack of local resources;
• Increased caregiver stress;
• Difficulty obtaining a correct diagnosis.
There are numerous benefits to using telehealth services for both patients with rare diseases, such as:
• Convenience;
• Cost savings;
• Improved access to care;
• Ability to see multiple providers that can help with symptom monitoring, assessment, and treatment services.
It is important to consider limitations when creating a model for clinical care for patients with rare diseases. Some limitations to think about are:
• Clinician and organization familiarity with telehealth;
• Reimbursement and coverage from insurance companies for telehealth;
• Security and privacy of patient information;
• Training of telehealth providers;
• Logistical factors, including use of equipment, internet/connectivity, and technical troubleshooting.
Future directions should involve collaborative research that studies the effectiveness, feasibility, and perceptions of families of rare diseases and providers that use telehealth for clinical healthcare services. Research should also further study and consider ways to improve barriers and challenges associated with implementing telehealth systems into existing healthcare systems.
Introduction
The World Health Organization declared a pandemic in March 2020 due to the rising number of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or COVID-19) cases. The transmission of the COVID-19 virus occurs during person-to-person contact; therefore, a key factor in slowing the spread of the virus includes the practice of social distancing. Consequently, many health organizations had to modify their standard of care across patient and clinical care services during the pandemic to slow the spread of the virus by reducing or canceling non-essential in-person appointments and procedures. 2 The use of telehealth services has been paramount in continuing to deliver the provision of care (e.g. assessment, planning, treatment, and coordination services) across patient populations. 3 Data from Duke institutional operations report increasing their telehealth services from <1% of total visits to 70% of total visits (e.g. >1000 video visits) in a 4-week time period. 2 Patients and healthcare providers also reported a high level of satisfaction with the use of telehealth services during the COVID-19 pandemic, particularly in subspecialty fields. 4
The COVID-19 pandemic transformed the landscape of delivery of healthcare across the world. Telehealth services were delivered out of necessity to ensure seamless delivery of healthcare for each individual. Patient and provider perceptions of the utility of telehealth services are encouraging and support the long-term use of telehealth services in clinical practice after the pandemic. 5 Telehealth may provide a strategy that has far-reaching benefits for diverse patient populations, such as patients with Batten disease and other rare diseases, who face additional barriers to accessing healthcare services and specialty care. The aims of this paper, through the experience of a single Batten Disease Center of Excellence, are to (1) review the benefits and barriers involved in the delivery of telehealth services to patients with rare diseases; (2) discuss components of a model for clinical care that utilizes telehealth services for patients with Batten disease; (3) discuss limitations and future directions of using telehealth in patients with rare diseases. To accomplish these aims, the authors have reviewed current literature utilizing PubMed and Web of Science of telehealth care delivery between 2010 and 2021. The proposed clinical model is based on a single center experience of a Batten Disease Center of Excellence, in which pediatric patients with Batten disease and their caregivers come from the United States, Europe, and South America. Patients are evaluated within a multidisciplinary model that includes a team of specialists from the disciplines of pediatric neurology, physical therapy, occupational therapy, speech therapy, psychology, and social work.
Batten disease and rare diseases
Batten disease, or neuronal ceroid lipofuscinoses, includes a class of lysosomal storage inherited disorders that are neurodegenerative and fatal. The gene defects associated with Batten disease disrupt the cell’s lysosomal functioning and ability for the cell to recycle molecules. There are 13 genotypic forms of Batten disease that are characterized by mutations on different genes that can vary in disease onset and severity of symptoms. 6 Batten disease is a rare disorder with a worldwide prevalence of 1 in 100,000 live births.7,8 Most symptoms of Batten disease begin during early childhood. Symptoms include vision loss, seizures, developmental delays, cognitive regression, and motor impairments.9 –11 Individuals with Batten disease experience premature death. Although there is no cure for Batten disease, there are approved treatments with enzyme replacement therapy (ERT) and promising research currently being conducted, such as gene therapy.10,12 To date, cerliponase alfa (Brineura; BioMarin Pharmaceutical) is the only Food and Drug Administration approved treatment to slow the progression of one form of Batten disease (CLN2) through ERT. 13
Treatment for individuals with Batten disease include symptom management and palliative care. 14 Individuals with Batten disease often participate in rehabilitation treatment modalities to help maintain developmental skills, physical health, and quality of life. Clinical care for individuals with Batten disease involves ongoing assessment and treatment across multidisciplinary healthcare providers. Disruption in healthcare services can add to increased family stress, as well as potentially adverse developmental and medical outcomes, given the pervasiveness of symptom presentation and nature of disease progression. Unfortunately, the unique and ongoing needs that patients with Batten disease and their families face are not exclusive of other populations with rare diseases. In the United States, a disease is characterized as rare if it affects about 1 in 2000 people. 15 Although, the authors of this manuscript reference patients with Batten disease in the models and considerations proposed below, the applications are likely able to be broadly applied to other populations with rare diseases.
Barriers to accessing clinical services for individuals with rare diseases
It can be challenging to access evidence-based clinical services across patient populations; however, unique and additional barriers exist in the field of rare diseases. 16 Individuals with rare diseases have heterogeneous etiologies that are often chronic and fatal. In comparison with common diseases, there is a paucity of research and guidance for clinical practice in rare diseases. Bell and Smith 17 analyzed characteristics of interventional trials and found that of the 24,000 trials categorized as part of their study only 11.5% were rare diseases trials. Research guides clinical practice; therefore, it is alarming and unfortunate that individuals with rare diseases are underrepresented in clinical research trials. Listed below are additional barriers and challenges to accessing clinical services that individuals and families of patients with rare diseases may experience:
Lack of local resources. Patients with rare diseases are geographically dispersed and may not have local access to large healthcare organizations or specialty clinics. They also travel longer distances for specialty care providers to receive targeted or comprehensive treatment and/or diagnostic services. Many patients with rare diseases have complex medical needs and require ongoing follow-up with multiple providers for the management of clinical symptoms. Increased transportation demands and travel also increase financial burden on families. Additionally, there may be longer waitlists to access services depending on local resources and capacity for service delivery to patients with rare diseases.
Difficulties achieving accurate diagnosis. Delays in accurate diagnosis are related to a lack of understanding of prodromal and clinical symptoms by referring or clinical providers. Many rare diseases have limited information about the natural history of the disease, resulting in a lack of knowledge about disease progression and presentation. 16 Diagnosis of rare diseases often requires confirmation through next generation sequencing or genetic testing via a chromosomal microarray, 18 which can require additional clinical resources or result in external referrals to access services (e.g. genetic counselor) and can significantly delay diagnosis depending on the family’s access to those resources. 19
Provider lack of knowledge of rare diseases etiology and treatment. Even providers that are familiar with rare diseases may lack knowledge about disease progression and treatment. Evidence based treatments that are used as standard of care to alleviate symptoms (e.g. medication management) or work on skill acquisition (e.g. speech therapy) of patients with common disease may not be as effective. This may be because treatment is not targeting the same mechanistic factors given potential etiologic differences between patients with rare and common disease. Local healthcare providers in remote areas likely have not had exposure to, let alone training on, diagnosis or treatment of rare diseases. Also, potential for collaboration and consultation with other providers with expertise in rare diseases may be scarce or difficult to arrange and a limiting factor in service delivery and a provider-to-provider training opportunity.
Caregiver stress and isolation. Parents of children with rare diseases often become overwhelmed due to the complex medical needs of their child. This responsibility sometimes results in change or loss of employment due to the increased time and demands that may be required to provide care. Parents of children with rare diseases are at a higher risk for experiencing more stress, anxiety, and depression 20 and also may experience feelings of isolation and lack of emotional support. 21 The availability of the internet has improved access to families and organizations but they may still need to advocate and coordinate their own family’s clinical care due to limited knowledge from service providers, which places a burden on families to assume the “expert” rather than the “parent” role. 21
Telehealth services
Telemedicine services can be an effective way to deliver care outside of emergency situations. The US Department of Health Resources and Services Administrations 1 defines telehealth as the “use of electronic information and telecommunication technologies to support long-distance clinical healthcare, patient and professional health-related education, public health, and health administration. Technologies include video conference, the internet, store-and-forward imaging, streaming media, and terrestrial and wireless communication.” Telehealth services can be classified into both provider-to-patient and provider-to-provider communications, through the use of e-consults, remote patient monitoring, patient-initiated messaging, telephone visits, and video visits. 2 There are numerous benefits22 –24 of utilizing telehealth services in clinical medicine, including:
Convenience. Patients have flexibility to see their healthcare providers from home or a location that is convenient for them. This reduces the need for transportation or barriers related to child-care to attend appointments. Providers also have flexibility to see their patients at times that are convenient to them without logistics of navigating use and availability of clinical space.
Cost savings. It improves access to healthcare professionals (e.g. primary care providers, specialty doctors) and may decrease the cost of urgent care and emergency visits.
Improved access to care. Patients may have increased access to care due to less barriers related to geographic location of the patient or provider. Patients with physical limitations or other health considerations may be able to access telehealth services more easily.25,26 Providers may be able to see more patients without the barrier of the confinement of a physical clinical space. This also creates space for patients that need to be seen for “in-person” visits. In a study that analyzed the benefits of telehealth during COVID-19 that were selected by neuro-ophthalmologists, 61.3% selected access to care as a benefit. 23
Multidisciplinary visits. It can be easier for multidisciplinary specialists to coordinate and provide care. Multidisciplinary providers can be from different geographic locations to see patients. It increases collaboration and consultation from providers with varying professional backgrounds and areas of clinical expertise.
Provider-to-provider consultation. Providers can seek medical consultation and advice in “real-time” to best fit the needs of their patients. Moss and colleagues 23 report that 87% of survey responders indicated “continuity of care” as a benefit of telehealth video visits. Additionally, video teleconferencing can help disseminate medical knowledge and expertise among providers in rare disease through case-based learning. 27
Infection control. The spread of disease and infection is reduced with fewer patients and staff present in clinical spaces.
Diagnosing, treating, and triaging patients. Improved access may lead to quicker services of diagnostic, treatment, and triage services.
Considerations in delivering telehealth services in rare diseases
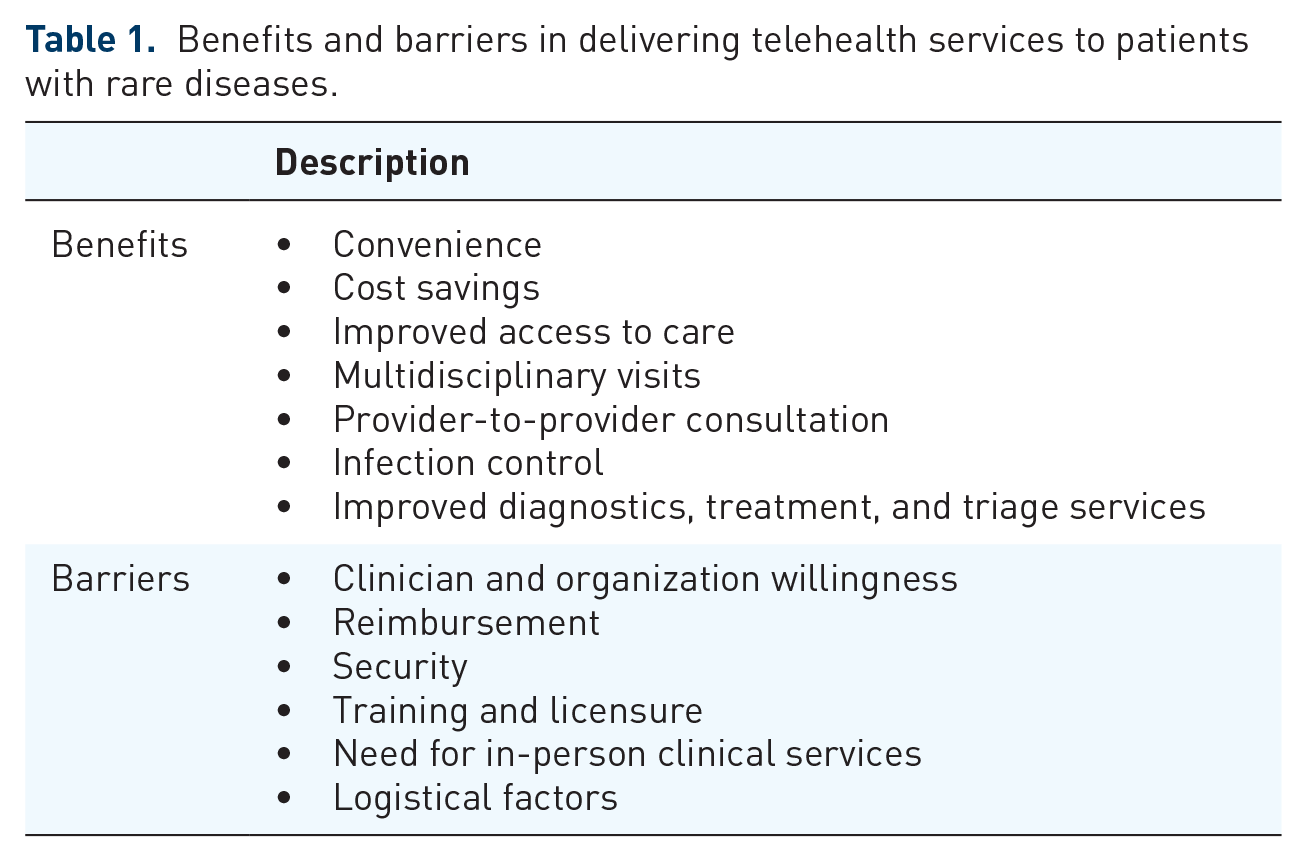
Although there are many benefits in delivering telehealth services to patients with rare diseases that are highlighted above, there are a few limitations that warrant consideration before employing telehealth services. Barriers to delivering telehealth services are highlighted below, as well as listed in Table 1:
Benefits and barriers in delivering telehealth services to patients with rare diseases.
Clinician and organization willingness. There may be clinician and organizational resistance to implementing telehealth into standard of care, particularly when there is less familiarity with telehealth.3,28 It can be difficult for organizations to restructure appointments and services offered as standard of care into a telehealth format. The integration of telehealth services into a healthcare system may require additional workflows and responsibilities. There may be a need for additional staff with training of specific skillsets in telehealth. 24 Staff training and education in delivering telehealth services can help improve clinician acceptance of telehealth. 29
Reimbursement. Current reimbursement models for healthcare services may not include telehealth services as an option for coverage.3,22,24 Insurance providers also require specific credential or licensure to practice via telehealth in specific states to ensure coverage. The reimbursement of clinical services delivered via telehealth may be different from clinical services provided in-person.
Security. It is crucial for telehealth platforms to be secure and protect patient information. 22 Breach of confidentiality of patient information is a risk when using digital modalities. Patients and providers should consider risks and take measures to secure private medical information.
Training and licensure. There are reduced geographic boundaries in delivering telehealth services that impact clinical practice. In order to protect patients and providers, there needs to be consideration of guidelines of medical licensure when providing telehealth services. 22 State laws may vary state-to-state that may influence clinical practice. Careful consideration should be given by healthcare organizations and private providers to legal aspects of telehealth service delivery. Clinicians should receive specialized training to know clinical and professional boundaries when delivering telehealth services remotely across geographic regions.
Need for in-person clinical services. Although many clinical services can be provided remotely through telehealth, there are some services that require in-person appointments or clinical visits, such as physical exams, imaging services (X-rays, etc.), and laboratory services. This is an important consideration because patients with rare diseases often have unique physical and medical needs that require routine physical exams and laboratory work to monitor outcomes and to prevent degradation. Collaboration and consultation with local providers that can conduct in-person clinical services might be an option to supplement telehealth services or specialty care.
Logistical factors. There are logistical factors to consider when delivering telehealth services, including equipment, internet/connectivity, and technical troubleshooting. The logistics of employing telehealth services may prove challenging for individuals who are less “tech savy.” 22 Also, the use of technology to telehealth may further exacerbate disparities in healthcare to patient populations that do not have access to internet or devices that are required to support telehealth. 30 The digital platform of telehealth also introduces technical difficulties that hinder or disrupt the delivery of clinical services that are not present during in-person clinical visits.
Rationale for providing telehealth services
When developing clinical service delivery systems for telehealth it is important to consider foundational questions of healthcare delivery through the lens of telehealth. The first question that needs to be considered is how patients with rare diseases may benefit from telehealth services. Telehealth services can be utilized for many clinical purposes, including parent education, symptom management, developmental assessment and monitoring services, and direct intervention. Considerations likely will need to be individualized for each healthcare organization and patient needs; however, the following clinical model may provide guidance when developing a framework to deliver telehealth services.
In Batten disease, children and young adults are ideally managed through a multidisciplinary neurology clinic. Williams and colleagues 14 identified four domains of services in the management of Batten disease: medical, quality of life, family support, and end-of-life care. Once diagnosed, there are immediate needs for parent education and service coordination, as well as family centered emotional support. Long-term symptom management involves management of seizures, cognitive deterioration, management of nutrition, and pulmonary concerns. Given the neurodegenerative nature of Batten disease, repeated cognitive assessments are necessary to monitor skill regression. Developmental therapies are also conducted in an attempt to maintain skills and facilitate development as possible. Allied health services including physical, occupational, and speech therapy are necessary to support recommendations for local services. Some of these services, such as developmental monitoring, developmental therapies, and some medication consultation, can be completed partially or completely through telehealth. However, other procedures, especially direct medical interventions or laboratory work (e.g. blood draws), cannot be completed through telehealth. The decision of which elements of a clinical process can be implemented over a telehealth system is a first step toward creating a model of care.
It is also important to consider the requirements that must be satisfied to implement telehealth services. Procedures and protocols may vary across institutions, but it is important to keep patient safety and confidentiality in mind when establishing telehealth services. Chowdhury and colleagues 31 provide guidance for performing telehealth services and suggest obtaining written or verbal consent from the patient or parent prior to arranging the telehealth encounter. It is also important to have compliance with HIPAA and utilize a modality that is secure and offers a platform that allows direct communication to the patient. Organizations should consider integration of telehealth services into the patient’s electronic medical record that allow multiple providers to be present at the appointment and to have access to patient information, scheduling, billing, and insurance information. 31 It is also important to consider technology infrastructure (e.g. access to broadband, computers/tablets, software, cameras, and microphones) and familiarity in using technology platforms for both providers and patients. 32
Building a multidisciplinary team
A strength of telehealth service delivery is that it reduces some barriers of multidisciplinary work, namely, conducting appointments over video conferences reduces the facility needs of large multidisciplinary teams and eases some scheduling challenges that arise from many busy practitioners having to be co-located in order to have multidisciplinary clinics. Clinic teams for rare genetic diseases are generally led by a medical provider who acts as the team lead. 12 Teams consist of medical providers, nursing staff, psychologists, physical therapists, occupational therapists, speech therapists, social workers, and other neurodevelopmental professionals. When adapting these teams to telehealth, it will be important for team members to spend some time outlining their individual practices. This allows teams to identify possible redundancies across disciplines and create a virtual clinic flow. Team appointments over telehealth allow multiple providers to observe a child’s behavior at the same time, which can reduce the tasks demands placed on a child during an appointment. In order to take advantage of this opportunity, the team should think actively and flexibly about how best to order activities throughout the clinic.
Developing a clinic team for a given rare genetic disease will always require individual consideration. In our institution, a multidisciplinary approach to Batten disease as a center of excellence has the following components:
Neurology. Our clinic team is led by neurology. However, this is variable in other rare disease settings which may be led by a metabolic physician, geneticist, or palliative care physician. The clinic physician considers medication management and the integration of other services to provide a complete conceptualization of the child’s needs.
Psychology. Another necessary discipline within the assessment team is psychology. Given the neurodegenerative nature of Batten disease, cognitive assessments are a necessary component to assess and implement services for children with Batten disease. Telehealth services can be provided by a psychologist to provide assessment of general cognitive and adaptive functioning with comparable results to face-to face services. 33 The psychologist can also provide behavioral assessment, consultation, and recommendations for treatment.
Speech and language pathology. Speech and language pathology is also an important component in the multidisciplinary team. Direct monitoring of receptive, expressive, and pragmatic language skills will be important in considering the child’s overall cognitive functioning and monitoring regression, as well as continuing to tailor language intervention to a child’s current level of functioning. Speech pathology can also assist in considering the use of augmentative and alternative communication systems. This team member also monitors swallowing or feeding difficulties.
Occupational and physical therapy. An occupational and physical therapy service also critical to the multidisciplinary assessment and treatment of Batten disease is the monitoring of the child’s fine and gross motor skills. Therapists can provide assessment and treatment services as well as any medical equipment needs that may be necessary to support a child’s mobility or fine motor dexterity.
Social work. Social workers are members of the team who focus on care coordination services for families as well as helping to support families through the complexities and emotional issues of families with complex medical needs.
Caregivers and family members. Caregivers of pediatric patients with rare diseases are critical members involved in the assessment and treatment process. It is crucially important for other members of the multidisciplinary team to consult and provide education to caregivers, as they are most likely involved in the direct care of the patient. Caregivers often provide important clinical information regarding symptom presentation and developmental skills that inform medications and therapy goals. Clinical models should consider the development of protocols and how to disseminate information and recommendations to caregivers who are involved in the direct treatment and care of the patient.
Assessment procedures
An evaluation begins with developmental, medical, and behavioral history. Given the team nature of the evaluation, this assessment can be conducted with all team members present for efficiency. The interview is led by the team physician, who focuses on elucidating the primary goals of the assessment, medical history, and current medical needs. Each subsequent team member can then add necessary questions from the perspective of their discipline. This process allows a comprehensive history to be taken for the team’s consideration, without subjecting caregivers to multiple providers’ repeated questions.
Each discipline conducts specific testing and evaluation practices based on their evidence-based practice. We recommend reviewing medical records to allow the team to prioritize the complex medical needs of each patient. This allows the team to consult with one another and communicate areas of assessment that might be needed by each team member. Comprehensive assessment generally includes testing a patient’s cognitive or developmental functioning, language skills, and motor functioning. Caregivers may also complete structured or semi-structured interviews, as well as rating scales, to provide a comprehensive view of the child in multiple settings and from multiple perspectives. These assessments also allow the team neurologist to observe the child’s development with each member of the evaluating team. After each individual testing session is completed the team can conference to decide potential diagnoses and preliminary treatment course. Finally, feedback is given to the family with any appropriate diagnoses, a plan for necessary medical testing orders, and recommendations for any necessary developmental, behavioral, or educational intervention. This evaluation process can provide a robust understanding of their child’s development and a comprehensive plan for future care.
Developmental assessment conducted through telehealth
There are careful considerations that should be made when designing a battery for remote testing. When a patient’s developmental skills are evaluated in-person during a clinical visit, the clinician has an opportunity to directly elicit developmental skills in a carefully controlled environment using standardized assessment. Developmental skills can also be assessed through telehealth by caregiver questionnaires and interviews evaluating adaptive and developmental functioning. Certain cognitive and neuropsychological assessment measures can also be reliably performed via telehealth.34,35 Consideration for specific cognitive domains, such as attention or memory, should be given when assessing via telehealth. For example, the quality of the audio, as well as distractions in the testing environment may be difficult to manage. Cognitive and developmental assessments and other methods (e.g. caregiver report, behavioral observations) conducted through telehealth can guide recommendations for treatment and intervention efforts.
When completing assessments remotely, it is especially important to consider historical sources of information that may describe a child’s developmental functioning. Previous evaluations may have been completed for local early intervention services. These previous evaluations can help build an understanding of a child’s functioning, as well as provide a baseline with which current observations of development can be compared. For clinics where assessments are going to be consistently completed in other areas, it is beneficial to develop relationships with local providers who can work in partnership with the team to facilitate direct assessment of the child’s developmental skills.
When choosing assessment measures for telehealth developmental assessment, it is important to consider how likely it will be to be able to get a direct sample of the skill being assessed over video conferencing and the standardization of the testing instrument being used. To date, no direct tests of child development have been developed to be administered in a telehealth setting. However, there is a growing evidence base of studies that some tests, including the Weschler Intelligence Scale – Fifth Edition (WISC-5) 36 and the Woodcock Johnson Cognitive Abilities-Fourth Edition, 37 have equivalency over telehealth services. Similarly, verbally based tests have been shown to yield equivalent results over telehealth platforms. 38 This would suggest that some assessment of language skills, such as the Clinical Evaluation of Language Fundamentals-Fifth Edition (CELF-5) 39 could be administered remotely. Initial findings suggest that remote assessment of cognitive abilities in patients with rare disease is promising. Ragbeer and colleagues 35 conducted a pilot study that compared remote cognitive assessment with in-person evaluations and found high agreement and feasibility in their sample of patients with Batten disease.
Options for standardized testing have limitations over telehealth but questionnaires and direct behavior assessment can be performed. In these cases, assessments will have to be conducted through a combination of parent report and informal observation of developmental milestones. There are multiple developmental measures that are normed using parent report, including developmental assessments [e.g., Developmental Profile-Fourth Edition (DP-4), language assessments (Receptive-Expressive Emergent Language Test (REEL), and adaptive behavior measures (Vineland Adaptive Behavior Scales – Third Edition (Vineland-3)].40 –42 If a clinician is relying on these parent report measures to assess a child’s skills, it will be important to also make some qualitative observational assessment of the child’s skills over video. This will allow the clinician to consider the validity of the results of indirect assessment and improve the decisions that are made based on those indirect assessments. In cases where traditional direct assessment of skills is not possible, it will be important to choose developmental tests that allow for indirect parent report of skills as well as opportunities to probe developmental skills directly, such as the Developmental Assessment of Young Children – Second Edition. 43 It will be important for each clinic to define the parameters under which tele-assessment tools should be utilized.
In the example of CLN3 Batten disease, as patients begin to experience vision impairment, a recommended neurocognitive testing battery includes verbal cognitive subtests from the WISC-5, a verbal sentence recall task (CELF-5), and verbal working memory tasks taken from the Wide Range Assessment of Memory and Learning – Second Edition.44,45 The addition of parent report of adaptive skills using a Vineland-3, and behavior rating measures, such as the Child Behavior Checklist, 46 completes a comprehensive assessment battery that could be completed exclusively over telehealth. For children who cannot answer questions verbally, utilizing the DP-4, REEL, and/or Vineland-3 will allow clinicians to obtain standardized ratings of child development. When paired with direct behavior observations, the multidisciplinary team will be able to make informed recommendations regarding the child’s treatment and educational needs.
Treatment
Although telehealth serves most naturally as an avenue for briefer forms of consultation, the COVID-19 pandemic has ushered in a significant increase in telehealth treatment services. It is possible for therapy services to be completed over telehealth models.47,48 The telehealth model allows the children access to the allied health professionals during the pandemic and tailor to their child’s specific needs. Although the literature base is still evolving, there is evidence that therapy for children with developmental disabilities via telehealth can be effective. 49
Direct therapy with the children with rare diseases over telehealth may be challenging depending on the developmental level of the child or medical complexities associated with their disease. Parent-mediated intervention can be a viable option to delivery treatment and consultation services. Parent training models of treatment have been found to be effective to increase the rate of a child’s learning across multiple domains of functioning. Parent training models of therapy have demonstrated efficacy over telehealth in children with other neurodevelopmental disabilities, such as autism spectrum disorder. 50
Provider-to-provider consultation services
Telehealth also provides an opportunity for targeted consultative service delivery that could be especially helpful in continuing care. Access to specialized care for developmental disabilities is challenging in rural communities. 51 In Batten disease, children have complex medical issues including cognitive, visual, and physical limitations. Consultative services that could be conducted over telehealth include educational services to help families understand their child’s specialized instruction through the school. Educational consultation could also be used to advocate for some proactive considerations for visual impairment, to help children learn skills such as braille or using a cane. Speech consultation services could also be used to help a family and treating speech therapy provider to consider and implement functional communication strategies or an augmentative and alternative communication system. Medical consultation services are frequently used to adjust or reconsider medical interventions. Behavioral consultation services are used to manage emergent disruptive or maladaptive behaviors, as well as working with occupational therapy consultation to increase functional independence. Telehealth consultation services can also be considered as a means to monitor or enhance services between in-person clinic visits. The use of targeted consultation services is one of the ways in which services can be delivered in novel and creative ways to increase the quality of overall care that a child receives.
Future directions
Healthcare systems should consider building standardized clinical models that utilize telehealth services to provide services to patients with rare diseases. There are numerous benefits in using telehealth that can enhance and expand service delivery between the patient and clinician. Telehealth services can also improve provider-to-provider communication and collaboration when providing clinical care to individuals with rare diseases. Although there are many benefits to utilizing telehealth services in provision of care to patients with rare diseases, it is important to consider factors that may limit or add additional barriers prior to implementing telehealth services. It is also critical to consider security and privacy when choosing telehealth platforms that protect private patient information. 2 Smith and colleagues 3 propose the following strategies when implementing telehealth services in emergency contexts that may also be applied to routine models of care: (1) ensure that all health professionals receive appropriate education and training; (2) introduce telehealth accreditation for professionals; (3) provide funding which adequately covers that cost of providing telehealth services; (4) redesign clinical models of care; (5) support all stakeholders with an effective communication and change management strategy; and (6) establish system to manage telehealth services on a routine basis.
There is a need for future research to examine and compare the effectiveness and outcomes of telehealth services with standard-of-care or specialized services that are provided in-person. Clinical outcomes that should be considered are costs, patient experiences and satisfaction, provider experiences and satisfaction, disease or health outcomes, and feasibility. Additionally, future work should focus on challenges associated with the implementation of telehealth services, including reducing barriers previously discussed, as well as the practicality of utilizing telehealth services. Telehealth continues to be a promising avenue to deliver effective and efficient clinical services to diverse patient populations, such as those with rare diseases.
Footnotes
Author contributions
Jessica Scherr: Conceptualization; Resources; Writing-original draft; Writing-review & editing
Charles Albright: Conceptualization; Resources; Writing-original draft; Writing-review & editing
Emily De Los Reyes: Corresponding Author; Conceptualization; Resources; Writing-original draft; Writing-review & editing.
Conflict of interest statement
E. de los Reyes has grant support and consultancy with BioMarin and Amicus Therapeutics.
J. Scherr has grant support with Biomarin.C. Albright has grant support with Amicus Therapeutics.
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Ethics statement
Ethical approval and informed consent were not required for this review.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.