
Abstract
Transcatheter aortic valve replacement has been established as an advanced therapeutic modality for severe aortic stenosis. Despite procedural advancements, anatomical variations may hinder successful prosthetic valve delivery in certain cases. Delivering a relatively bulky prosthesis through a constricted and extensively stenosed surgical bioprosthetic valve remains challenging. Such cases require alternative procedural strategies to enable smooth device navigation. In this case, the presence of a surgical tissue prosthesis with a Dacron conduit resulted in stacking of the delivery system within the aortic arch. An anchor balloon (20/45 mm) over a buddy wire was used to assist in guidewire compression and effective valve advancement.
Keywords
Introduction
The first clinical implementation of transcatheter aortic valve replacement (TAVR) was carried out in a middle-aged patient. In 2002, a prototype balloon-expandable valve was successfully deployed by Professor Alain Cribier in a 57-year-old male with severe aortic stenosis (AS), who was deemed unsuitable for surgery due to hemodynamic instability and multiple coexisting comorbidities. 1 Initially, coronary interventions were conducted on a small group of extremely low-risk patients, but they began to include more high-risk and complex cases. 2 In contrast, TAVR was initially utilized in elderly high-risk patients and later extended to younger populations.
Today, we are facing a lifetime management strategy for severe AS. The primary goals are to minimize open heart surgery procedures and to avoid anticoagulation. 3 This strategy includes transcatheter aortic valve implantation in degenerated, dysfunctional surgical bio-valves. 4 Many factors influence the strategy of TAVR in surgical aortic valve replacement (SAVR): (a) valve selection, (b) procedural techniques, (c) coronary protection, and (d) late accessibility. 5 In some clinical cases, crossing the degenerated surgical bio-valves with a TAVR device may be compromised, even more so in the case of previous ascending aorta surgery, despite improved versions of new valve prostheses and new flexible delivery systems.
We described a situation in which the presence of a surgical bioprosthetic valve and Dacron conduit complicated transcatheter valve implantation. We obtained the strategy of stent delivery from percutaneous coronary intervention with the distal anchor balloon technique. 6 Unlike prior cases, this case employed a distinct approach of anchoring the transcatheter valve system on an artificial surgical aortic bioprosthesis using a distal 20/45 mm balloon.
Case Presentation
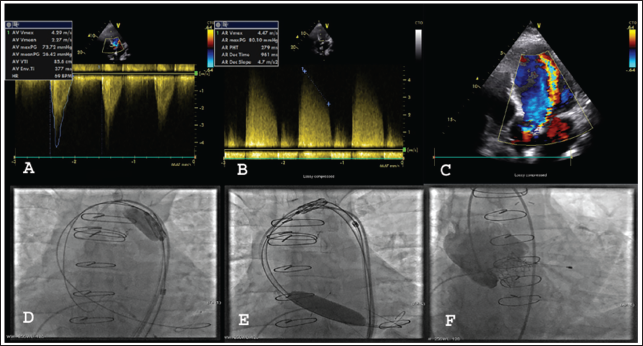
A 39-year-old man suffering from severe artificial surgical valve AS and New York Heart Association (NYHA) class III heart failure symptoms was prescribed to go for a TAVR. His medical background was notable for acute aortic dissection, leading to SAVR with a 23 mm Braile tissue valve and bioprosthetic conduit in the ascending aorta 9 years ago. Although his vital parameters were within acceptable limits, a physical examination revealed bilateral pretibial leg edema with a high-grade (5/6) systolic ejection murmur best heard at the apical section. Transthoracic echocardiography highlighted a structurally deteriorated artificial tissue aortic valve, with an area of 0.82 cm 2 and peak and mean pressure gradients of 73 and 36 mmHg (Figure 1A), with concomitant severe aortic regurgitation (AR) (Figure 1B) and moderate to severe lateral paravalvular leak (PVL) (Figure 1C). Evaluation by the heart team concluded that the patient was inoperable, and TAVR was advised.
(A) Severe Artificial Valve Stenosis. (B) Severe Artificial Valve Regurgitation. (C) Severe Artificial Valve Paravalvular Leak. (D) Inchworming Balloon in the Aortic Valve. (E) Anchor Balloon on Buddy Wire Compressing Transcatheter Aortic Valve Replacement (TAVR) Wire to Surgical Bioprosthesis Assisted to Cross Aortic Arch. (F) Valve in a Good Position and Function.
Approach
Informed consent was taken from the patient. The procedure was performed under general anesthesia. Right groin access was used for valve deployment. Right groin access was used to place a temporary transvenous pacemaker. A Python sheath (Meril Life Sciences, Vapi, India) was placed easily. An Amplatz Super Stiff™ guidewire (Boston Scientific, Marlborough, MA, USA) was placed in the left ventricle (LV). A five-French pigtail catheter was used for the first aortogram that was introduced through the left femoral artery. The 24.5-mm Myval bioprosthesis (Meril Life Sciences, Vapi, India) was advanced. However, the aortic arch could not be surpassed. Several attempts aimed to alter the catheter’s flexion proved ineffective.
A diagnostic 6F AL1 catheter (Medtronic, Minnesota, USA) was administered via the left groin to position an additional Amplatz Super Stiff™ guidewire (Boston Scientific, Marlborough, MA, USA) in the LV as a buddy wire. However, this maneuver also proved to be unsuccessful. The prosthetic aortic valve was placed on top of the TAVR wire, and balloon inflation at reduced pressure with the aortic valve balloon 20/45 mm (Valver, Balton, Poland) on the buddy wire from the left groin, upgraded to 9F in the aortic arch, failed to advance the valve (Figure 1D). Then, the same aortic balloon was positioned in the bioprosthetic valve, compressing the TAVR wire on the surgical bioprosthesis, thus anchoring the TAVR wire and increasing its pushability. This technique pushed the TAVR prosthesis into the ascending aorta and across the aortic valve while the balloon in the surgical bioprosthesis was simultaneously inflated (Figure 1E). This anchoring approach was effective. The anchor balloon and buddy wire were retrieved from the left groin. After confirmation of positioning, the valve was positioned under rapid pacing at 180 beats/min. The balloon catheter was subsequently withdrawn into the descending thoracic aorta, followed by the performance of an aortogram. The valve was optimally positioned, with no evidence of AR (Figure 1F). Transthoracic echocardiography further confirmed appropriate valve positioning, resolution of the transvalvular gradient, and the absence of paravalvular AR (Table 1). On the following day, repeat echocardiography demonstrated complete resolution of AS, AR, and PVL.
Pre- and Post-procedural Hemodynamics.

At the 6-month follow-up, the patient’s condition had improved, with no shortness of breath and a status of NYHA I, indicating no signs of congestive heart failure. The transthoracic echocardiography reveals a maximal gradient across the TAVR prosthesis of 18 mmHg and a mean gradient of 10 mmHg, demonstrating the effectiveness of the treatment.
Discussion
Very often, advanced interventions are necessary to prevent TAVR insufficiency. As far as our case is concerned, the prosthesis was stacked on a tube placed in the ascending aorta in the previous surgery. Crossing the native aortic arch may be technically challenging because of several anatomical and procedural factors, leading to disastrous outcomes, 7 such as angulation, calcification, or, in our case, the presence of a Dacron conduit. The anchor balloon approach was used to enhance pushability and the delivery of the prosthesis to make it easier to pass.
The Buddy balloon technique, which uses the transfemoral contralateral approach with a peripheral balloon, was described in the literature as facilitating valve delivery in TAVR. 8 Yao et al. described snaring the delivery wire to navigate devices in patients with complex aortic anatomies. 9 The anchor balloon technique was successfully used to deliver stents in complex coronary anatomy. Fujita et al. originally described this technique as the inflation of a balloon in a side branch of the target coronary vessel to enhance backup support and further stabilize the “Anchor wire.” 10 A Dacron conduit and a surgical bioprosthetic valve presented challenges in our case. We used balloon support for the TAVR device progression in the descending aorta (body balloon) and crossing the aortic arch (anchoring).
Unlike other reported cases, our study used a larger balloon anchored in the LV to deliver the valve in the proper place.
Conclusion
In conclusion, the anchor balloon technique and device proper placement were difficult in our case, but the prosthesis could cross the aortic arch with a Dacron conduit. This technique could also reduce exposure to radiation, thereby ensuring success and decreasing the probability of more catastrophic adversities.
Footnotes
Authors Contribution
SL: Conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing—original draft, writing—review and editing.
VV: Data curation, investigation, visualization, writing—original draft, writing—review and editing.
NM: Data curation, investigation, visualization, writing—original draft, writing—review and editing.
MB: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.