Severe aortic stenosis (sAS) is a relentless disease, which carries significant morbidity and mortality. Definitive treatment of sAS in the form of aortic valve replacement (AVR) mostly revolves around the presence of symptoms. Last decade has witnessed a surge in observational data suggesting asymptomatic sAS associated with higher cardiovascular events than what was previously appreciated. While society guidelines endorse early AVR in a selected subgroup of asymptomatic sAS patients, the majority are still managed with traditional “watchful-waiting” approach. This article reviews the available literature on the natural history of asymptomatic sAS, associated risk modifiers, and identify patients who are at high-risk for future clinical events to offer them preemptive valve placement therapy.
Epidemiologic transition in countries like India is often reflected in its disease spectrum as well.1, 2 Chronic risk-based diseases start taking a center stage over receding trends in nutritional or infectious diseases. One such palpable change is seen in the field of valvular heart disease where a shift from rheumatic to degenerative pathology is apparent.3 Rising prevalence of severe aortic stenosis (sAS) reflects an ageing population exposed to traditional atherosclerotic risk factors. Foundational principles of the natural history of sAS come from the original work of Braunwald and Ross from 1968 and predate the use of echocardiogram.4 The dataset obtained from autopsy study of 64 patients with an average age of 48 years demonstrated sAS of having a long latent asymptomatic period with low cardiovascular (CV) event rate. The onset of symptoms heralded a dismal prognosis with 2-year mortality reaching 50% unless treated with aortic valve replacement (AVR). Hence, decision making in sAS mostly revolves around the presence of symptoms.5, 6 The long latent period seen in the original study is likely reflective of congenital or rheumatic disease in the young population and may not apply at its face value to degenerative sAS in the elderly population. Recent data suggest that asymptomatic sAS may not be as benign as is thought to be with 5-year event-free survival as low as 25%.7-10
Hemodynamic Pathophysiology
Aortic stenosis (AS) incurs a fixed afterload to the left ventricle (LV) manifesting as elevated valvulo-arterial impedance (Zva).11 LV pressure overload leading to compensatory LV hypertrophy (LVH) is often maladaptive, with associated diastolic dysfunction and elevated LV filling pressure. Myocardial wall stress and related abnormal cardiac-coronary coupling result in increased early systolic deceleration of coronary blood flow responsible for myocardial ischemia without epicardial coronary artery stenosis.12, 13 Disproportionate LVH, left ventricular mass >110% of age-gender matched population, in the absence of hypertension has been correlated with worse prognosis.14, 15 Concentric remodeling and subendocardial ischemia eventually lead to myocardial fibrosis, which can be demonstrated by speckle tracking echocardiogram16, 17 or cardiac MRI (CMR)18, 19 and are associated with poorer outcomes even in the absence of overt clinical symptoms. A staging system of sAS progression is described from stage 0 to stage 4 with each subsequent stage marked by a gradual parametric change seen on echocardiogram culminating in pulmonary hypertension and biventricular dysfunction.20
Asymptomatic Status
Up to 50% of patients with sAS may not report typical symptoms of angina, syncope, or heart failure and are often considered “asymptomatic”.7, 21 While few patients may experience atypical symptoms such as easy fatigability or nonspecific weakness, others may not have any symptom at all. It is imperative to note that sAS being a slowly progressive disease typically affecting patients in their 6th decade of life or later, many patients adjust their activity level to avoid symptoms. These limitations evolve over months rather than days or weeks and are easily attributed to ageing thus leading to underreporting and/or underestimation of the symptoms. Eventually, patients start avoiding social functions, stop going out for shopping or playing with their grandkids, avoid taking stairs, etc. Musculoskeletal symptoms, typically present in sexagenarians and older, are often remarkably absent and should alert a physician to enquire about physical activity or lack thereof. Occasionally, sAS is revealed for the first time with cardiac decompensation following an intercurrent illness like infection, thus unmasking itself.
Treadmill Test
Treadmill stress test (TMT) will unveil limiting symptoms in almost 50% of patients with “asymptomatic” sAS22 and is endorsed by society guidelines in asymptomatic sAS.5, 6 Positive TMT, particularly presence of symptoms, is associated with 6-fold increased risk of cardiac death with high predictive value and gets a class I recommendation for early AVR.5, 6, 23 For this reason, TMT as a risk stratifying tool is increasingly being advocated. A supervised, symptom-limited, low-workload TMT using modified Bruce or Naughton protocol24 is both safe and yields meaningful information.24-26 In a series of 347 patients with AS undergoing TMT, no major adverse events were reported.27 It should be noted that TMT is contraindicated in symptomatic patients. TMT essentials in sAS are summarized in Table 1.
True “Asymptomatic” Severe Aortic Stenosis
Patients with sAS who do not report any active cardiac symptoms at age-appropriate physical activity and/or have a negative TMT can be considered truly asymptomatic. While the afterload mismatch of sAS may not be leading to a manifest clinical syndrome, it continues to add hemodynamic burden to the LV as discussed previously. The annualized rate of sudden cardiac death (SCD) in asymptomatic sAS is 1% to 1.5% and in up to 75% of the patients, SCD may be the first presenting symptom.8, 28 Definitive therapy in the form of surgical AVR helps mitigate the risk but must be a balancing act against the cost of perioperative mortality. Too early AVR imposes unnecessary surgical risk, need for anticoagulation, and bioprosthetic valve degeneration. By contrast, AVR at later stages of the disease leads to higher perioperative risk and suboptimal long-term outcome.20 AVR performed at each subsequent stage is associated with a 45% increase in perioperative mortality. Even after an uneventful AVR, underlying myocardial damage fails to recover in up to 25% of the patients.29 Also, the surgical risk is age-dependent with perioperative mortality 1% to 3% in age <70 years, and 3% to 7% in older patients.30
Treadmill Exercise Testing in Patients With Asymptomatic Severe Aortic Stenosis
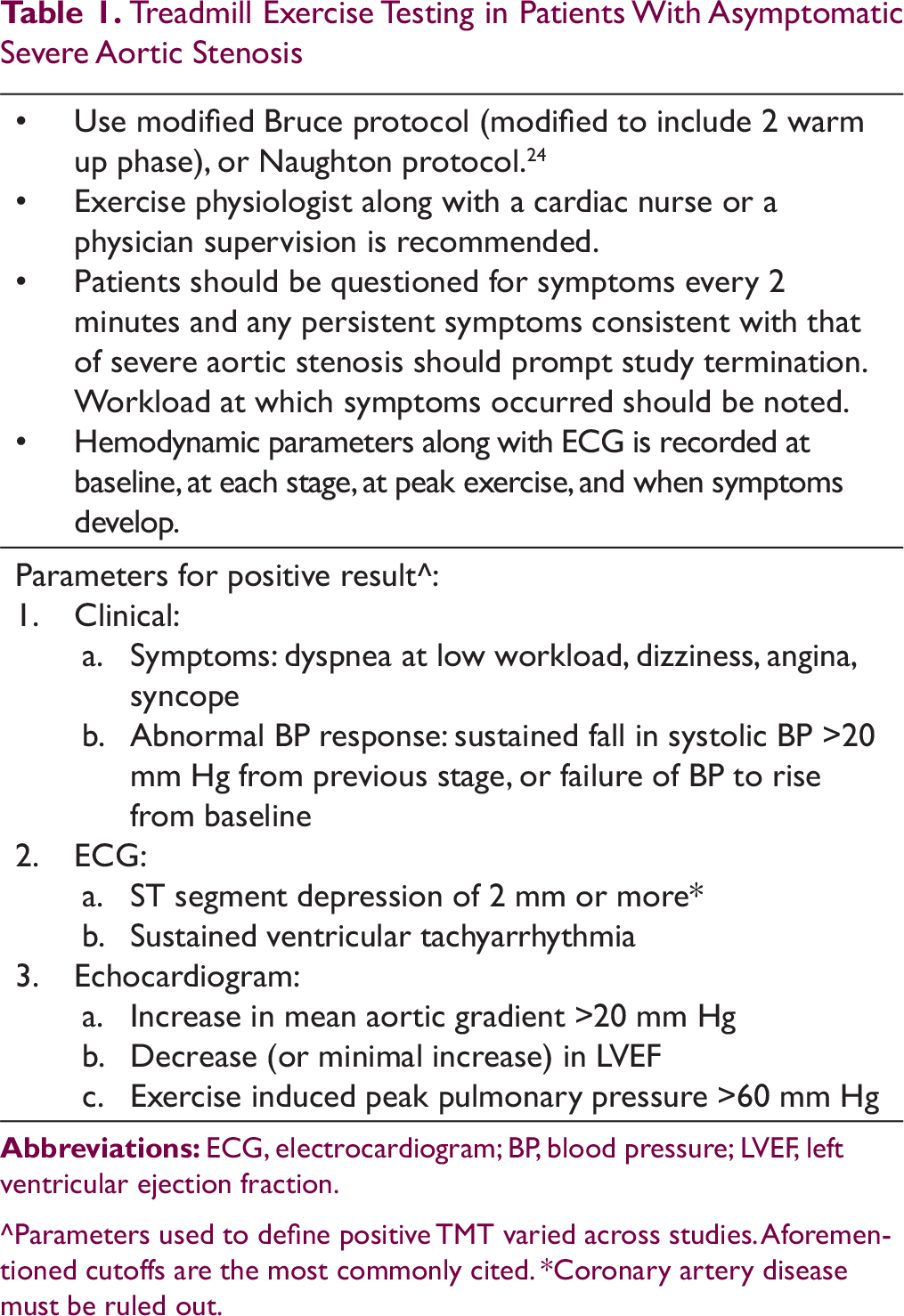
Use modified Bruce protocol (modified to include 2 warm up phase), or Naughton protocol.24
Exercise physiologist along with a cardiac nurse or a physician supervision is recommended.
Patients should be questioned for symptoms every 2 minutes and any persistent symptoms consistent with that of severe aortic stenosis should prompt study termination. Workload at which symptoms occurred should be noted.
Hemodynamic parameters along with ECG is recorded at baseline, at each stage, at peak exercise, and when symptoms develop.
Parameters for positive result^: 1. Clinical: a. Symptoms: dyspnea at low workload, dizziness, angina, syncope b. Abnormal BP response: sustained fall in systolic BP >20 mm Hg from previous stage, or failure of BP to rise from baseline 2. ECG: a. ST segment depression of 2 mm or more* b. Sustained ventricular tachyarrhythmia 3. Echocardiogram: a. Increase in mean aortic gradient >20 mm Hg b. Decrease (or minimal increase) in LVEF c. Exercise induced peak pulmonary pressure >60 mm Hg
^Parameters used to define positive TMT varied across studies. Aforementioned cutoffs are the most commonly cited. *Coronary artery disease must be ruled out.
Practical Issues Related to “Watchful-Waiting” Approach in Asymptomatic Severe Aortic Stenosis
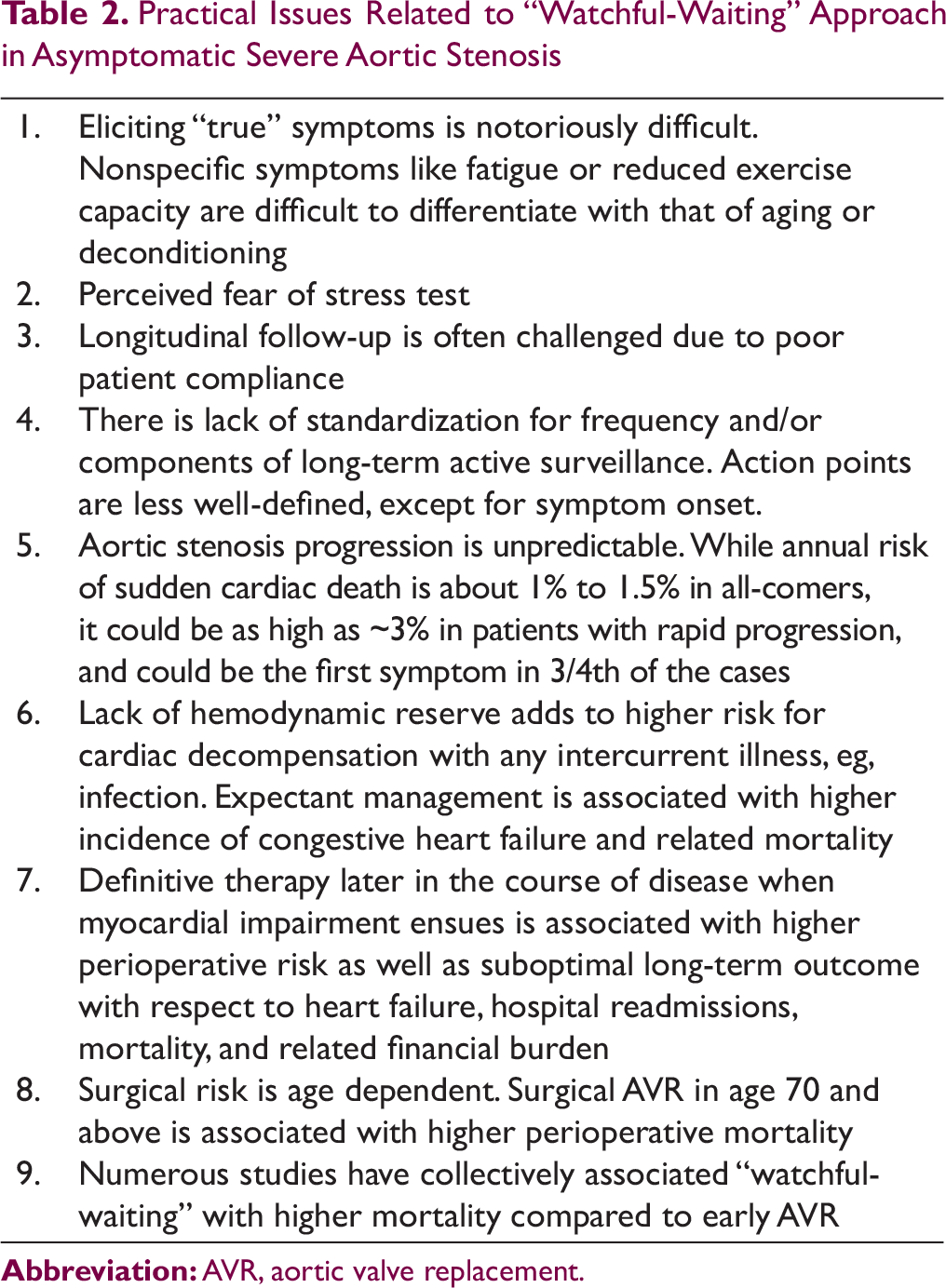
1. Eliciting “true” symptoms is notoriously difficult. Nonspecific symptoms like fatigue or reduced exercise capacity are difficult to differentiate with that of aging or deconditioning 2. Perceived fear of stress test 3. Longitudinal follow-up is often challenged due to poor patient compliance 4. There is lack of standardization for frequency and/or components of long-term active surveillance. Action points are less well-defined, except for symptom onset. 5. Aortic stenosis progression is unpredictable. While annual risk of sudden cardiac death is about 1% to 1.5% in all-comers, it could be as high as ~3% in patients with rapid progression, and could be the first symptom in 3/4th of the cases 6. Lack of hemodynamic reserve adds to higher risk for cardiac decompensation with any intercurrent illness, eg, infection. Expectant management is associated with higher incidence of congestive heart failure and related mortality 7. Definitive therapy later in the course of disease when myocardial impairment ensues is associated with higher perioperative risk as well as suboptimal long-term outcome with respect to heart failure, hospital readmissions, mortality, and related financial burden 8. Surgical risk is age dependent. Surgical AVR in age 70 and above is associated with higher perioperative mortality 9. Numerous studies have collectively associated “watchful-waiting” with higher mortality compared to early AVR
Abbreviation: AVR, aortic valve replacement.
In total, 5-year survival in asymptomatic sAS patients without AVR is reported to be anywhere between 38% to 83%.22 This heterogeneity in outcome is likely related to patient factors which if identified and treated early (with low perioperative mortality) may provide a net clinical benefit. Although preemptive AVR is increasingly being advocated in a certain subset of patients, “watchful-waiting” is often the most common short-term risk-aversion strategy chosen by treating physicians. Practical issues related to “watchful-waiting” approach is listed in Table 2. A study level pooled meta-analysis of early AVR performed within 3 months of diagnosis vs “watchful-waiting” in asymptomatic sAS found the latter strategy to be associated with ~3.5-fold higher mortality.22
Risk Parameters and Their Role in Early AVR
Risk parameters and related society guidelines to aid in decision-making for AVR in asymptomatic sAS are summarized in Table 3. It is noteworthy that most of the listed recommendations are categorized as level of evidence B or C; the conclusions are drawn mostly from small-scale studies or expert consensus given lack of robust randomized data. Binary cutoff values, in the guidelines or elsewhere, are mostly derived out of observational studies, are inconsistent across different society statements, and have less clinical relevance when used in isolation. A multiparametric approach to risk modifiers listed in Table 3 combined with clinical risk profile like diabetes and/or dyslipidemia is likely to be more relevant in predicting CV outcomes.
Aortic Stenosis Severity
Long-term clinical outcome, particularly SCD, is directly related to stenosis severity and rate of progression.21, 28 Very severe AS (VSAS), defined as peak aortic jet velocity >5 m/s, mean pressure gradient ≥60 mm Hg, aortic valve area (AVA) <0.6 cm2, indexed AVA <0.4 cm2/m2 (<0.45 cm2/m), or dimensionless index <0.20, has almost twice the risk of annual mortality compared to sAS.30-32 Natural history study of 1375 asymptomatic patients with VSAS in HAVEC registry showed 4-year survival of 20% without AVR.33 Current AS study, largest observational series on asymptomatic sAS, found 3% annual incidence of SCD and cumulative primary outcome of 9% per year in VSAS patient cohort.8 In total, 5-year event-free survival of VSAS patients in this series was noted to be dismal 11%. Registry,34 as well as randomized35 data, has brought out benefits of early AVR in VSAS. Patients with valve area ≤0.75 cm2 managed conservatively had ~10-fold higher mortality compared to early surgery with a median follow-up of 6 years.35 This was even after the fact that 74% of patients in conservative arm underwent AVR on follow-up. Recovery trial can be considered pivotal in being the first and the only published randomized trial addressing the role of early AVR in asymptomatic sAS patients.35
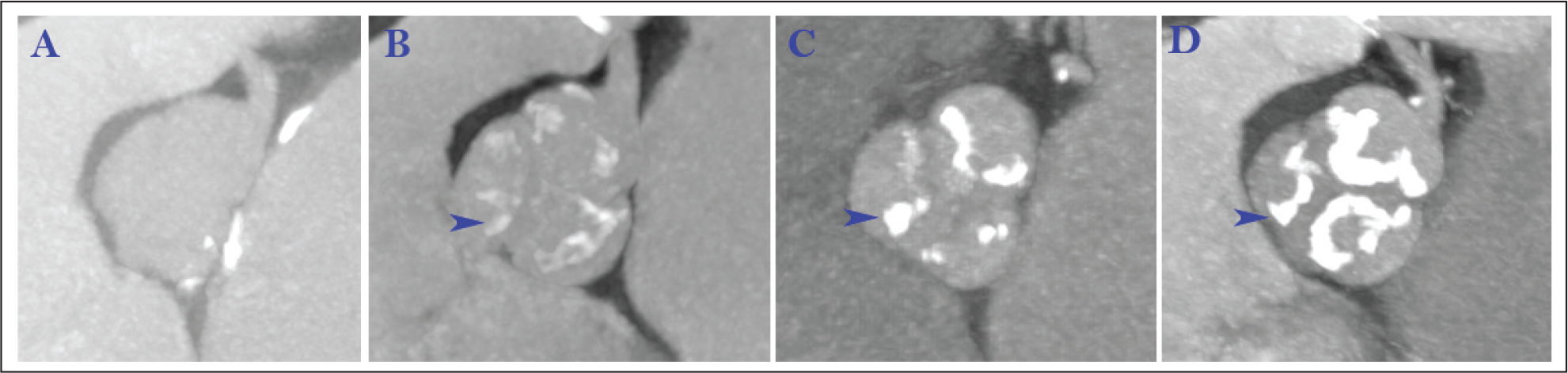
While the rate of disease progression is highly variable among individuals, increase in Vmax >0.3 m/s/year has been associated with symptom onset or mortality of 79% at 2 years.10, 28, 36 High aortic valve calcium on CT imaging correlates well with the amount of calcium present (Figure 1), is a predictor of rapid disease progression, and is associated with lower event-free survival.10, 37 A calcium score of 1200 AU (Agatston Unit) for females and 2000 AU for males is often used as standard cutoff values.38 High global ventricular afterload, represented by Zva >5 mm Hg/mL/m2, signifies a higher degree of valvular stenosis and carries poorer prognosis.11, 16, 39 Increase in mean aortic gradient during stress echocardiogram by >20 mm Hg is correlated with worse outcome,9, 40 although stress echocardiogram is rarely performed for this indication. There is paucity of data defining role of dobutamine stress echo (DSE) in asymptomatic patient. Unmasked symptoms during DSE has been shown to predict need for AVR within 1 year. Indices like steep pressure drop/flow rate41 and reduced valve compliance42 as assessed during DSE are also implicated of having discriminative value. Nevertheless, DSE can be associated with hypotension and/or arrhythmia is patients with sAS and should be used with caution.
Left Ventricular Outflow
Low flow state, defined as LV stroke volume index <35 mL/m2, is reported in 22% to 35% of the sAS patients with preserved LVEF43, 44 and may reflect an advanced stage in asymptomatic disease spectrum. The underlying pathology is thought to be an increase in global LV afterload, pathological concentric remodeling, and intrinsic myocardial dysfunction including reduced LV long-axis function. Low flow state is an independent predictor of poor prognosis, with a 2-fold increase in cardiac event rate and 30% event-free survival at 2 years.44 “Low flow low gradient” state likely represents very-late hemodynamic phenotype and has worst clinical outcome with 3-years event-free survival one-fifth that of “normal flow low gradient” pattern.43, 44
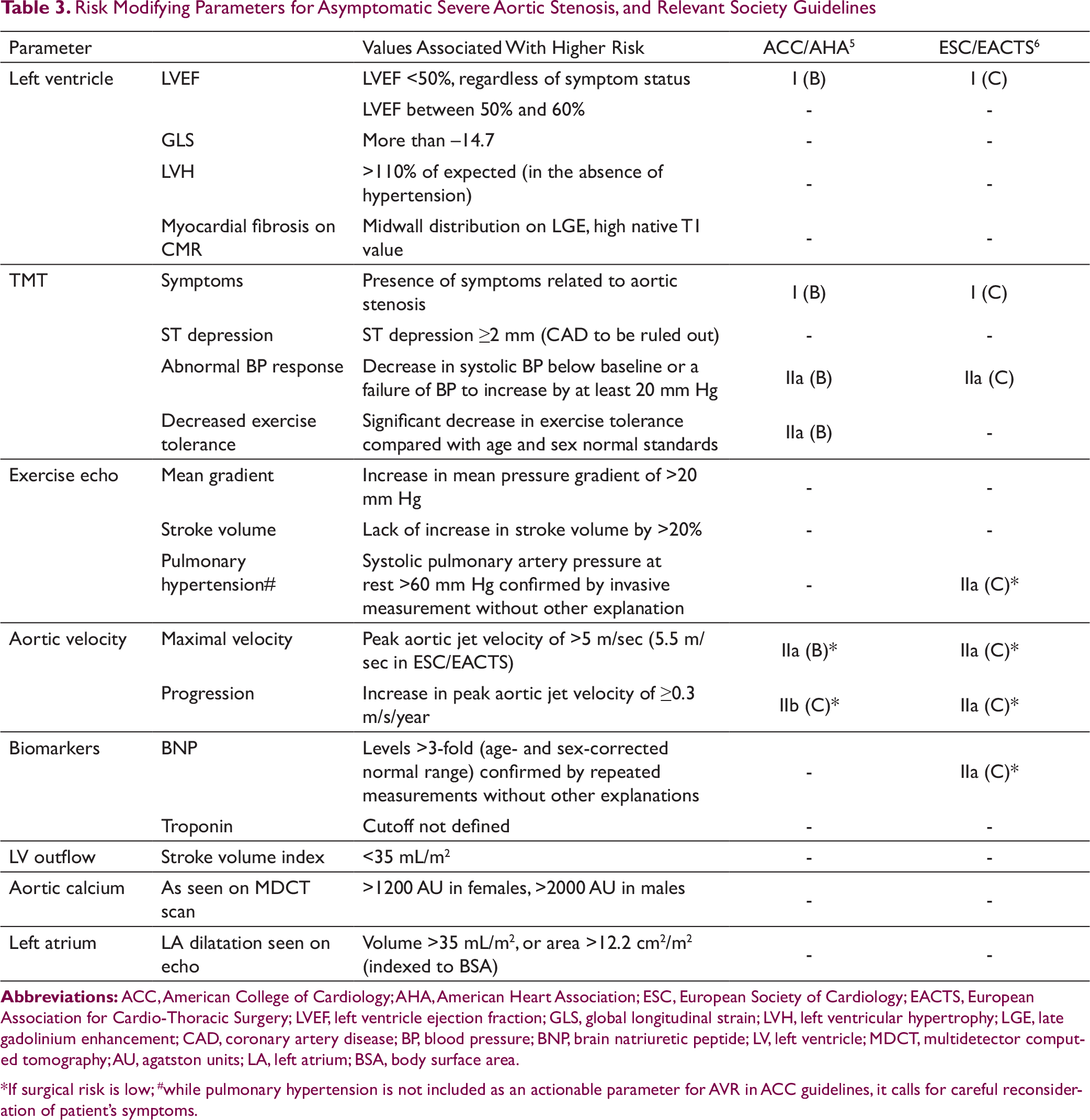
. Risk Modifying Parameters for Asymptomatic Severe Aortic Stenosis, and Relevant Society Guidelines
>110% of expected (in the absence of hypertension)
-
-
Myocardial fibrosis on CMR
Midwall distribution on LGE, high native T1 value
-
-
TMT
Symptoms
Presence of symptoms related to aortic stenosis
I (B)
I (C)
ST depression
ST depression ≥2 mm (CAD to be ruled out)
-
-
Abnormal BP response
Decrease in systolic BP below baseline or a failure of BP to increase by at least 20 mm Hg
IIa (B)
IIa (C)
Decreased exercise tolerance
Significant decrease in exercise tolerance compared with age and sex normal standards
IIa (B)
-
Exercise echo
Mean gradient
Increase in mean pressure gradient of >20 mm Hg
-
-
Stroke volume
Lack of increase in stroke volume by >20%
-
-
Pulmonary hypertension#
Systolic pulmonary artery pressure at rest >60 mm Hg confirmed by invasive measurement without other explanation
-
IIa (C)*
Aortic velocity
Maximal velocity
Peak aortic jet velocity of >5 m/sec (5.5 m/sec in ESC/EACTS)
IIa (B)*
IIa (C)*
Progression
Increase in peak aortic jet velocity of ≥0.3 m/s/year
IIb (C)*
IIa (C)*
Biomarkers
BNP
Levels >3-fold (age- and sex-corrected normal range) confirmed by repeated measurements without other explanations
-
IIa (C)*
Troponin
Cutoff not defined
-
-
LV outflow
Stroke volume index
<35 mL/m2
-
-
Aortic calcium
As seen on MDCT scan
>1200 AU in females, >2000 AU in males
-
-
Left atrium
LA dilatation seen on echo
Volume >35 mL/m2, or area >12.2 cm2/m2 (indexed to BSA)
-
-
Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; EACTS, European Association for Cardio-Thoracic Surgery; LVEF, left ventricle ejection fraction; GLS, global longitudinal strain; LVH, left ventricular hypertrophy; LGE, late gadolinium enhancement; CAD, coronary artery disease; BP, blood pressure; BNP, brain natriuretic peptide; LV, left ventricle; MDCT, multidetector computed tomography; AU, agatston units; LA, left atrium; BSA, body surface area.
*If surgical risk is low; #while pulmonary hypertension is not included as an actionable parameter for AVR in ACC guidelines, it calls for careful reconsideration of patient’s symptoms.
Subclinical Left Ventricular Dysfunction
Patients with sAS and depressed LVEF (stage C2) regardless of their symptom status should be referred for AVR.5 In clinical practice though, only 0.4% of patients with depressed LVEF are asymptomatic. Recent studies have emphasized that patients with LVEF between 50% and 60% experience higher CV event rate compared to patients with LVEF >60%.33 This can be explained by the presence of subclinical LV systolic dysfunction, which is demonstrated in almost 50% of patients using advanced imaging like speckle tracking echocardiogram or CMR.45 An abnormal global longitudinal strain of more than –14.7 is associated with 2.5-fold higher mortality.44, 46-48 Strain parameters derived from 3D speckle tracking echocardiogram may have higher predictive value.49 CMR defined midwall myocardial fibrosis is related with higher clinical events18, 50-55 also is less likely to improve after successful AVR56 leading to a higher incidence of heart failure and CV mortality. Clinical impact of myocardial fibrosis seems to be dose-dependent with a higher volume of late gadolinium enhancement leading to poorer outcome.50 Noncontrast mapping of T1 relaxation time on 3T-CMR represents diffuse myocardial fibrosis and has been correlated with poor prognosis. Highest tertiles of native T1 values are associated with worst event-free survival in the untreated cohort, and higher clinical event rate post-AVR at 28-month follow-up.57
Double oblique computed tomography images of aortic valve demonstrating calcification grading. Grade 1 (A), no calcification; grade 2 (B), mild calcification (small isolated spots of calcification); grade 3 (C), moderate calcification (multiple larger spots of calcification); and grade 4 (D), heavy calcification (extensive calcification of all aortic valve leaflets)Source:
Other Echocardiographic Markers
LA size increases in response to diastolic dysfunction and reflects chronic LV volume overload. LA volume >35 mL/m2 or area >12.2 cm2/m2 in patients with sAS is predictive of increased cardiac events11, 44, 58 even after successful AVR.59 Chronic hemodynamic myocardial stress advances to resting or exercise-induced pulmonary hypertension, both of which herald dismal prognosis.60, 61 Tissue doppler indices like reduced mitral annular systolic velocity (s′ < 4.5 cm/sec), or reduced late diastolic velocity (a′ < 9 cm/s) have also been associated with worse cardiac events.62
Biomarkers
Various biomarkers have been studied to risk stratify asymptomatic sAS patients, with multiple biomarkers elevation associated with worse clinical outcome.63 Among the novel biomarkers, brain natriuretic peptide (BNP) is the most studied.62, 64 BNP level seems to correlate well with the degree of AS severity once other causes of BNP elevation are ruled out. Patients with elevated BNP level, measured at rest or during peak exercise (treadmill), have poor long-term outcome and may benefit from an early AVR.65, 66 Levels higher than 3 times that of age-gender matched can be a trigger point for considering preemptive AVR if surgical risk is low.6 Elevated high sensitive troponin I (hsTnI) in sAS is suggested to be a marker of myocyte death associated with pathologic hypertrophy and is correlated with poor clinical outcome.67 Collectively these studies show that elevation in biomarkers reflects a maladaptive state to chronic pressure overload, which is reflected in clinical outcomes. Since biomarker levels change based on age, gender, renal function among others, an absolute cutoff value is less likely to have a clinical significance. On the other hand, rising trends observed over time can identify patients who are at risk for decompensation.
Summary
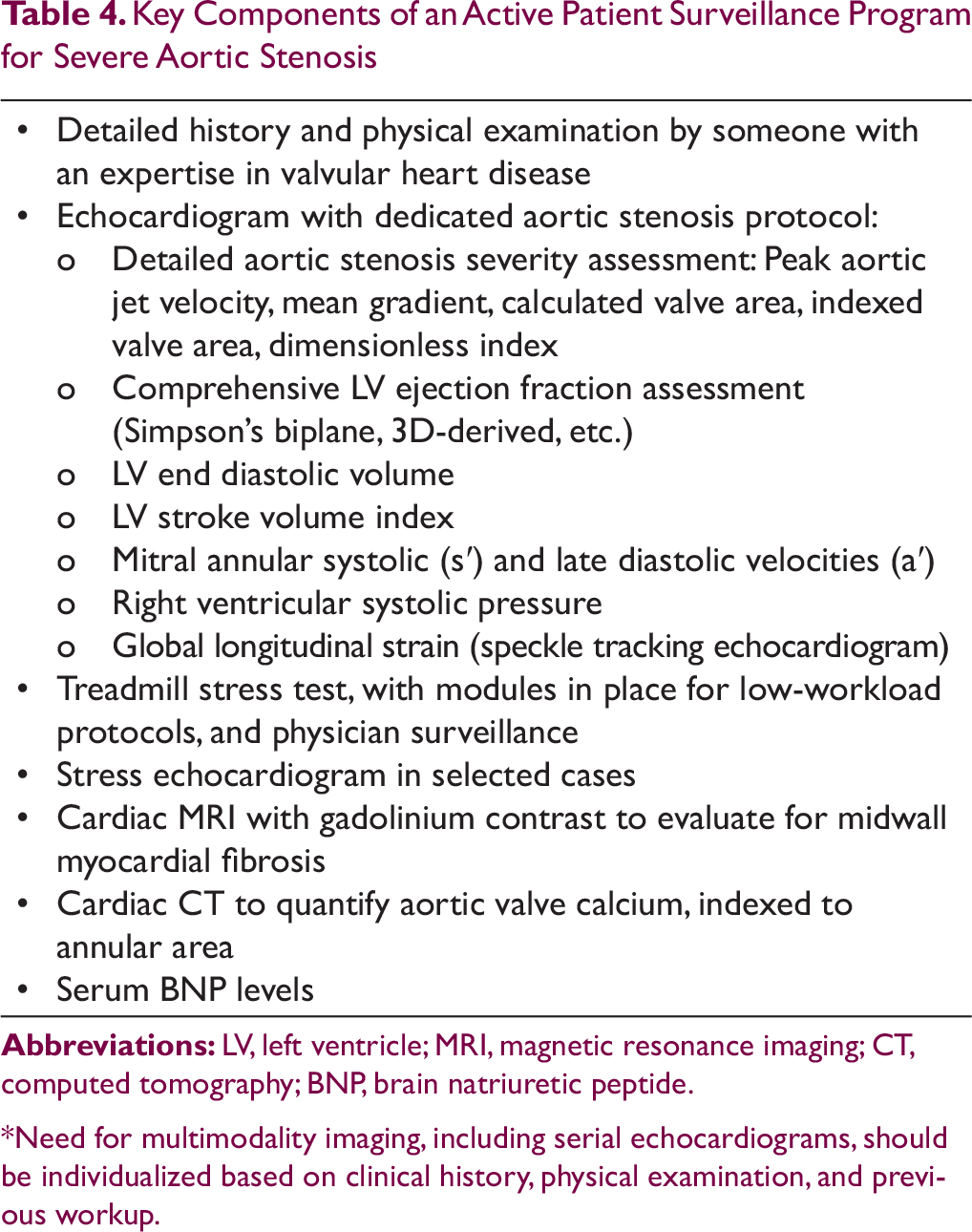
AS is a relentless disease with a steady yet unpredictable progression. Medical therapy has proven to be ineffective in improving major clinical outcome. AVR is the only effective and durable option to improve disease-related morbidity and mortality. Clinical tools most often utilized to aid in decision making for AVR relies on detecting gross myocardial impairment or associated clinical syndrome. Since myocardial damage is a continuous process ranging from subclinical to overt, biomarkers and contemporary multimodality imaging enable us to detect subclinical damage early in the course of the disease. While multiple studies correlate subclinical damage to worse CV outcome, there is clinical equipoise on the benefits of preemptive surgical AVR. Available data suggest however that it is reasonable to lower the threshold for AVR in certain high risk patient cohort, particularly if perioperative mortality risk is low (Table 3).5 A recent meta-analysis of 4075 asymptomatic sAS patients with 11,901 patient-years of follow-up showed a 62% reduction in long-term mortality with early AVR.68 Expectant management in asymptomatic sAS patients probably endangers their lives in ways previously not well appreciated. Management strategy should include an early consultation or referral to a Heart Valve Centre of Excellence. A proactive clinical approach integrating available risk modifying parameters is the need of the hour. A simplified risk-scoring algorithm from a single center in France has been proposed taking a few of these high risk features into account.66 The score is calculated using the formula: [peak aortic jet velocity (m/s) × 2] + (natural logarithm of BNP × 1.5) + 1.5 (if female sex). Patients with score in highest quartile had <10% event-free survival at the end of 20 months. Patients who do not qualify for early AVR, aggressive surveillance should be the default strategy. A vigilant follow-up program should aim at picking up early signs of myocardial distress and act before irreversible damage ensues. A robust surveillance framework can be designed at an institute level, taking local factors into consideration. Salient features of such framework are summarized in Table 4.
Key Components of an Active Patient Surveillance Program for Severe Aortic Stenosis
• Detailed history and physical examination by someone with an expertise in valvular heart disease• Echocardiogram with dedicated aortic stenosis protocol:
o Detailed aortic stenosis severity assessment: Peak aortic jet velocity, mean gradient, calculated valve area, indexed valve area, dimensionless index
o Comprehensive LV ejection fraction assessment (Simpson’s biplane, 3D-derived, etc.)
o LV end diastolic volume
o LV stroke volume index
o Mitral annular systolic (s′) and late diastolic velocities (a′)
o Right ventricular systolic pressure
o Global longitudinal strain (speckle tracking echocardiogram)• Treadmill stress test, with modules in place for low-workload protocols, and physician surveillance• Stress echocardiogram in selected cases• Cardiac MRI with gadolinium contrast to evaluate for midwall myocardial fibrosis• Cardiac CT to quantify aortic valve calcium, indexed to annular area• Serum BNP levels
Abbreviations: LV, left ventricle; MRI, magnetic resonance imaging; CT, computed tomography; BNP, brain natriuretic peptide.
*Need for multimodality imaging, including serial echocardiograms, should be individualized based on clinical history, physical examination, and previous workup.
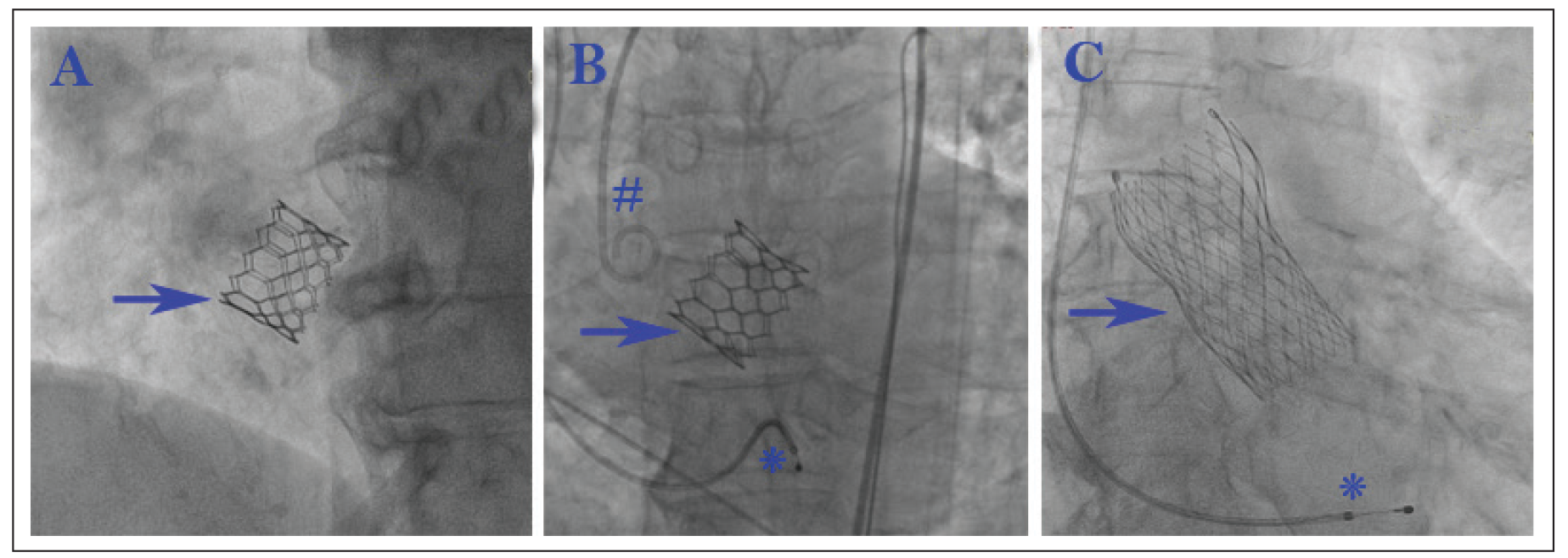
Transcatheter aortic valve replacement (TAVR) (Figure 2) with its excellent 30-day outcome in low surgical risk patients is bound to revisit the traditional treatment paradigm in asymptomatic sAS. As of this writing though, TAVR is not approved for asymptomatic sAS. Renaissance of preemptive AVR in asymptomatic sAS has triggered multiple strategy trials comparing early AVR to expectant management. EARLY TAVR will randomize asymptomatic sAS patients age >65 with a normal TMT to early TAVR vs clinical surveillance (NCT03042104). EVOLVED trial will include patients with elevated hsTnI and midwall fibrosis who do not qualify for AVR with the current standard of care and randomize them to TAVR vs routine clinical care (NCT03094143). AVATAR is an ongoing trial studying the role of surgical AVR in asymptomatic sAS patients (NCT02436655).
While the earlier discussion focuses on sAS, it is reasonable to question whether any degree of AS is detrimental to myocardial function. Increased ventricular afterload of any severity is bound to trigger compensatory mechanisms and a “normal” heart is expected to adapt to the excess workload. Yet, recent data has called in to question this established notion. Prospective and observational studies from France and Australia report poor long-term survival in patients with moderate AS when compared to patients without AS.69, 70 The hemodynamic burden of modest AS will conceivably have a higher clinical impact in patients with compromised LV, ischemic cardiomyopathy for instance.71 A novel risk assessment model combining cardiac damage staging classification and the valvular grading severity classification is proposed to identify patients who can potentially benefit with preemptive AVR in nonsevere AS.20 Role of TAVR in unloading the LV by preemptive treatment of nonsevere AS is being studied in the ongoing TAVR UNLOAD trial (NCT02661451). Our understanding of the interplay between the hemodynamic burden of AS and myocardial response is poised to change. It seems fair to consider AS as a disease of the aortic valve as well as the myocardium and include both in any clinical decision-making algorithm.13
Note: *Temporary pacing wire, #pigtail catheter.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
References
1.
YadavS, ArokiasamyP.Understanding epidemiological transition in India. Glob Health Action. 2014;7:23248. doi:10.3402/gha.v7.2324.
2.
Collaborators IS-LDBI. Nations within a nation: variations in epidemiological transition across the states of India, 1990-2016 in the Global Burden of Disease Study. Lancet. Dec 2017;390(10111):2437-2460. doi:10.1016/S0140-6736(17)32804-.
3.
NegiPC, SondhiS, AsotraS, MahajanK, MehtaA.Current status of rheumatic heart disease in India. Indian Heart J. 2019 Jan-Feb;71(1):85-90. doi:10.1016/j.ihj.2018.12.00.
NishimuraRA, OttoCM, BonowRO. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. Jun 2014;129(23):2440-2492. doi:10.1161/CIR.000000000000002.
6.
BaumgartnerH, FalkV, BaxJJ. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 09 2017;38(36):2739-2791. doi:10.1093/eurheartj/ehx39.
7.
PaiRG, KapoorN, BansalRC, VaradarajanP.Malignant natural history of asymptomatic severe aortic stenosis: benefit of aortic valve replacement. Ann Thorac Surg. Dec 2006;82(6):2116-2122. doi:10.1016/j.athoracsur.2006.07.04.
8.
TaniguchiT, MorimotoT, ShiomiH. Initial surgical versus conservative strategies in patients with asymptomatic severe aortic stenosis. J Am Coll Cardiol. Dec 2015;66(25):2827-2838. doi:10.1016/j.jacc.2015.10.00.
9.
MaréchauxS, HachichaZ, BellouinA. Usefulness of exercise-stress echocardiography for risk stratification of true asymptomatic patients with aortic valve stenosis. Eur Heart J. Jun 2010;31(11):1390-1397. doi:10.1093/eurheartj/ehq07.
10.
RosenhekR, BinderT, PorentaG. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med. Aug 2000;343(9):611-617. doi:10.1056/NEJM20000831343090.
11.
LancellottiP, DonalE, MagneJ. Risk stratification in asymptomatic moderate to severe aortic stenosis: the importance of the valvular, arterial and ventricular interplay. Heart. Sep 2010;96(17):1364-1371. doi:10.1136/hrt.2009.19094.
12.
LumleyM, WilliamsR, AsrressKN. Coronary physiology during exercise and vasodilation in the healthy heart and in severe aortic stenosis. J Am Coll Cardiol. Aug 2016;68(7):688-697. doi:10.1016/j.jacc.2016.05.07.
13.
DweckMR, BoonNA, NewbyDE.Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol. Nov 2012;60(19):1854-1863. doi:10.1016/j.jacc.2012.02.09.
14.
CioffiG, FaggianoP, VizzardiE. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. Feb 2011;97(4):301-307. doi:10.1136/hrt.2010.19299.
15.
DuncanAI, LoweBS, GarciaMJ. Influence of concentric left ventricular remodeling on early mortality after aortic valve replacement. Ann Thorac Surg. Jun 2008;85(6):2030-2039. doi:10.1016/j.athoracsur.2008.02.07.
16.
LancellottiP, DonalE, MagneJ. Impact of global left ventricular afterload on left ventricular function in asymptomatic severe aortic stenosis: a two-dimensional speckle-tracking study. Eur J Echocardiogr. Jul 2010;11(6):537-543. doi:10.1093/ejechocard/jeq01.
17.
KusunoseK, GoodmanA, ParikhR. Incremental prognostic value of left ventricular global longitudinal strain in patients with aortic stenosis and preserved ejection fraction. Circ Cardiovasc Imaging. Nov 2014;7(6):938-945. doi:10.1161/CIRCIMAGING.114.00204.
18.
BingR, CavalcanteJL, EverettRJ, ClavelMA, NewbyDE, DweckMR.Imaging and impact of myocardial fibrosis in aortic stenosis. JACC Cardiovasc Imaging. Feb 2019;12(2):283-296. doi:10.1016/j.jcmg.2018.11.02.
19.
TreibelTA, LópezB, GonzálezA. Reappraising myocardial fibrosis in severe aortic stenosis: an invasive and non-invasive study in 133 patients. Eur Heart J. Feb 2018;39(8):699-709. doi:10.1093/eurheartj/ehx35.
20.
GénéreuxP, PibarotP, RedforsB. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J. Dec 2017;38(45):3351-3358. doi:10.1093/eurheartj/ehx38.
21.
PellikkaPA, SaranoME, NishimuraRA. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation. Jun 2005;111(24):3290-3295. doi:10.1161/CIRCULATIONAHA.104.49590.
22.
GénéreuxP, StoneGW, O’GaraPT. Natural history, diagnostic approaches, and therapeutic strategies for patients with asymptomatic severe aortic stenosis. J Am Coll Cardiol. May 2016;67(19):2263-2288. doi:10.1016/j.jacc.2016.02.05.
23.
RafiqueAM, BinerS, RayI, ForresterJS, TolstrupK, SiegelRJ.Meta-analysis of prognostic value of stress testing in patients with asymptomatic severe aortic stenosis. Am J Cardiol. Oct 2009;104(7):972-977. doi:10.1016/j.amjcard.2009.05.04.
24.
RedforsB, PibarotP, GillamLD. Stress testing in asymptomatic aortic stenosis. Circulation. May 2017;135(20):1956-1976. doi:10.1161/CIRCULATIONAHA.116.02545.
25.
MagneJ, LancellottiP, PiérardLA.Exercise testing in asymptomatic severe aortic stenosis. JACC Cardiovasc Imaging. Feb 2014;7(2):188-199. doi:10.1016/j.jcmg.2013.08.01.
26.
LancellottiP, KarseraD, TumminelloG, LeboisF, PiérardLA.Determinants of an abnormal response to exercise in patients with asymptomatic valvular aortic stenosis. Eur J Echocardiogr. May 2008;9(3):338-343. doi:10.1016/j.euje.2007.04.00.
27.
DhobleA, SaranoME, KopeckySL, ThomasRJ, HayesCL, AllisonTG.Safety of symptom-limited cardiopulmonary exercise testing in patients with aortic stenosis. Am J Med. Jul 2012;125(7):704-708. doi:10.1016/j.amjmed.2012.01.01.
28.
OttoCM, BurwashIG, LeggetME. Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome. Circulation. May 1997;95(9):2262-2270. doi:10.1161/01.cir.95.9.226.
29.
ConnollyHM, OhJK, OrszulakTA. Aortic valve replacement for aortic stenosis with severe left ventricular dysfunction. Prognostic indicators. Circulation. May 1997;95(10):2395-2400. doi:10.1161/01.cir.95.10.239.
30.
TribouilloyC, RusinaruD, BohbotY, MaréchauxS, VanoverscheldeJL, Enriquez-SaranoM.How should very severe aortic stenosis be defined in asymptomatic individuals. J Am Heart Assoc. Feb 2019;8(3):e011724. doi:10.1161/JAHA.118.01172.
31.
RosenhekR, ZilberszacR, SchemperM. Natural history of very severe aortic stenosis. Circulation. Jan 2010;121(1):151-156. doi:10.1161/CIRCULATIONAHA.109.89417.
32.
KanamoriN, TaniguchiT, MorimotoT. Prognostic impact of aortic valve area in conservatively managed patients with asymptomatic severe aortic stenosis with preserved ejection fraction. J Am Heart Assoc. Feb 2019;8(3):e010198. doi:10.1161/JAHA.118.01019.
33.
LancellottiP, MagneJ, DulgheruR. Outcomes of patients with asymptomatic aortic stenosis followed up in heart valve clinics. JAMA Cardiol. Nov 2018;3(11):1060-1068. doi:10.1001/jamacardio.2018.315.
34.
KangDH, ParkSJ, RimJH. Early surgery versus conventional treatment in asymptomatic very severe aortic stenosis. Circulation. Apr 2010;121(13):1502-1509. doi:10.1161/CIRCULATIONAHA.109.90990.
35.
KangDH, ParkSJ, LeeSA. Early surgery or conservative care for asymptomatic aortic stenosis. N Engl J Med. Jan 2020;382(2):111-119. doi:10.1056/NEJMoa191284.
36.
EleidMF, SorajjaP, MichelenaHI, MaloufJF, ScottCG, PellikkaPA.Flow-gradient patterns in severe aortic stenosis with preserved ejection fraction: clinical characteristics and predictors of survival. Circulation. Oct 2013;128(16):1781-1789. doi:10.1161/CIRCULATIONAHA.113.00369.
37.
ClavelMA, PibarotP, Messika-ZeitounD. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: results of an international registry study. J Am Coll Cardiol. Sep 2014;64(12):1202-1213. doi:10.1016/j.jacc.2014.05.06.
HachichaZ, DumesnilJG, PibarotP.Usefulness of the valvuloarterial impedance to predict adverse outcome in asymptomatic aortic stenosis. J Am Coll Cardiol. Sep 2009;54(11):1003-1011. doi:10.1016/j.jacc.2009.04.07.
40.
LancellottiP, PellikkaPA, BudtsW. The clinical use of stress echocardiography in non-ischaemic heart disease: recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. Feb 2017;30(2):101-138. doi:10.1016/j.echo.2016.10.01.
41.
TakedaS, RimingtonH, ChambersJ.Prediction of symptom-onset in aortic stenosis: a comparison of pressure drop/flow slope and haemodynamic measures at rest. Int J Cardiol. Dec 2001;81(2-3):131-137; discussion 138-139. doi:10.1016/s0167-5273(01)00544-.
42.
DasP, RimingtonH, SmeetonN, ChambersJ.Determinants of symptoms and exercise capacity in aortic stenosis: a comparison of resting haemodynamics and valve compliance during dobutamine stress. Eur Heart J. Jul 2003;24(13):1254-1263. doi:10.1016/s0195-668x(03)00235-.
43.
HachichaZ, DumesnilJG, BogatyP, PibarotP.Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. Jun 2007;115(22):2856-2864. doi:10.1161/CIRCULATIONAHA.106.66868.
44.
LancellottiP, MagneJ, DonalE. Clinical outcome in asymptomatic severe aortic stenosis: insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol. Jan 2012;59(3):235-243. doi:10.1016/j.jacc.2011.08.07.
45.
ChinCW, PawadeTA, NewbyDE, DweckMR.Risk stratification in patients with aortic stenosis using novel imaging approaches. Circ Cardiovasc Imaging. Aug 2015;8(8):e003421. doi:10.1161/CIRCIMAGING.115.00342.
46.
MagneJ, CosynsB, PopescuBA. Distribution and prognostic significance of left ventricular global longitudinal strain in asymptomatic significant aortic stenosis: an individual participant data meta-analysis. JACC Cardiovasc Imaging. Jan 2019;12(1):84-92. doi:10.1016/j.jcmg.2018.11.00.
47.
NgACT, PrihadiEA, AntoniML. Left ventricular global longitudinal strain is predictive of all-cause mortality independent of aortic stenosis severity and ejection fraction. Eur Heart J Cardiovasc Imaging. Aug 2018;19(8):859-867. doi:10.1093/ehjci/jex18.
48.
VollemaEM, SugimotoT, ShenM. Association of left ventricular global longitudinal strain with asymptomatic severe aortic stenosis: natural course and prognostic value. JAMA Cardiol. 09 2018;3(9):839-847. doi:10.1001/jamacardio.2018.228.
49.
NagataY, TakeuchiM, WuVC. Prognostic value of LV deformation parameters using 2D and 3D speckle-tracking echocardiography in asymptomatic patients with severe aortic stenosis and preserved LV ejection fraction. JACC Cardiovasc Imaging. Mar 2015;8(3):235-245. doi:10.1016/j.jcmg.2014.12.00.
50.
DweckMR, JoshiS, MuriguT. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol. Sep 2011;58(12):1271-1279. doi:10.1016/j.jacc.2011.03.06.
51.
ChinCWL, EverettRJ, KwiecinskiJ. Myocardial fibrosis and cardiac decompensation in aortic stenosis. JACC Cardiovasc Imaging. Nov 2017;10(11):1320-1333. doi:10.1016/j.jcmg.2016.10.00.
52.
DelgadoV, BaxJJ.Will cardiac magnetic resonance change the management of severe aortic stenosis patients. JACC Cardiovasc Imaging. Jul 2018;11(7):984-986. doi:10.1016/j.jcmg.2017.11.03.
53.
ChinCW, Messika-ZeitounD, ShahAS. A clinical risk score of myocardial fibrosis predicts adverse outcomes in aortic stenosis. Eur Heart J. Feb 2016;37(8):713-723. doi:10.1093/eurheartj/ehv52.
54.
Barone-RochetteG, PiérardS, De Meester de RavensteinC. Prognostic significance of LGE by CMR in aortic stenosis patients undergoing valve replacement. J Am Coll Cardiol. Jul 2014;64(2):144-154. doi:10.1016/j.jacc.2014.02.61.
55.
VassiliouVS, PerperoglouA, RaphaelCE. Midwall fibrosis and 5-year outcome in moderate and severe aortic stenosis. J Am Coll Cardiol. Apr 2017;69(13):1755-1756. doi:10.1016/j.jacc.2017.01.03.
56.
TreibelTA, KozorR, SchofieldR. Reverse myocardial remodeling following valve replacement in patients with aortic stenosis. J Am Coll Cardiol. Feb 2018;71(8):860-871. doi:10.1016/j.jacc.2017.12.03.
57.
LeeH, ParkJB, YoonYE. Noncontrast myocardial T1 mapping by cardiac magnetic resonance predicts outcome in patients with aortic stenosis. JACC Cardiovasc Imaging. Jul 2018;11(7):974-983. doi:10.1016/j.jcmg.2017.09.00.
58.
ChristensenNL, DahlJS, Carter-StorchR. Relation of left atrial size, cardiac morphology, and clinical outcome in asymptomatic aortic stenosis. Am J Cardiol. Nov 2017;120(10):1877-1883. doi:10.1016/j.amjcard.2017.07.10.
59.
BeachJM, MihaljevicT, RajeswaranJ. Ventricular hypertrophy and left atrial dilatation persist and are associated with reduced survival after valve replacement for aortic stenosis. J Thorac Cardiovasc Surg. Jan 2014;147(1):362-369.e8. doi:10.1016/j.jtcvs.2012.12.01.
60.
MagneJ, PibarotP, SenguptaPP, DonalE, RosenhekR, LancellottiP.Pulmonary hypertension in valvular disease: a comprehensive review on pathophysiology to therapy from the HAVEC Group. JACC Cardiovasc Imaging. Jan 2015;8(1):83-99. doi:10.1016/j.jcmg.2014.12.00.
61.
LevyF, BohbotY, SanhadjiK. Impact of pulmonary hypertension on long-term outcome in patients with severe aortic stenosis. Eur Heart J Cardiovasc Imaging. May 2018;19(5):553-561. doi:10.1093/ehjci/jex16.
62.
LancellottiP, MoonenM, MagneJ. Prognostic effect of long-axis left ventricular dysfunction and B-type natriuretic peptide levels in asymptomatic aortic stenosis. Am J Cardiol. Feb 2010;105(3):383-388. doi:10.1016/j.amjcard.2009.09.04.
63.
LindmanBR, BreyleyJG, SchillingJD. Prognostic utility of novel biomarkers of cardiovascular stress in patients with aortic stenosis undergoing valve replacement. Heart. Sep 2015;101(17):1382-1388. doi:10.1136/heartjnl-2015-30774.
64.
Bergler-KleinJ, GyöngyösiM, MaurerG.The role of biomarkers in valvular heart disease: focus on natriuretic peptides. Can J Cardiol. Sep 2014;30(9):1027-1034. doi:10.1016/j.cjca.2014.07.01.
65.
ClavelMA, MaloufJ, MichelenaHI. B-type natriuretic peptide clinical activation in aortic stenosis: impact on long-term survival. J Am Coll Cardiol. May 2014;63(19):2016-2025. doi:10.1016/j.jacc.2014.02.58.
66.
MoninJL, LancellottiP, MonchiM. Risk score for predicting outcome in patients with asymptomatic aortic stenosis. Circulation. Jul 2009;120(1):69-75. doi:10.1161/CIRCULATIONAHA.108.80885.
67.
ChinCW, ShahAS, McAllisterDA. High-sensitivity troponin I concentrations are a marker of an advanced hypertrophic response and adverse outcomes in patients with aortic stenosis. Eur Heart J. Sep 2014;35(34):2312-2321. doi:10.1093/eurheartj/ehu18.
68.
GahlB, ÇelikM, HeadSJ. Natural history of asymptomatic severe aortic stenosis and the association of early intervention with outcomes: a systematic review and meta-analysis. JAMA Cardiol. Jul 2020;5(10). doi:10.1001/jamacardio.2020.249.
69.
DelesalleG, BohbotY, RusinaruD, DelpierreQ, MaréchauxS, TribouilloyC.Characteristics and prognosis of patients with moderate aortic stenosis and preserved left ventricular ejection fraction. J Am Heart Assoc. Mar 2019;8(6):e011036. doi:10.1161/JAHA.118.01103.
70.
StrangeG, StewartS, CelermajerD. Poor long-term survival in patients with moderate aortic stenosis. J Am Coll Cardiol. Oct 2019;74(15):1851-1863. doi:10.1016/j.jacc.2019.08.00.
71.
van GilsL, ClavelMA, VollemaEM. Prognostic implications of moderate aortic stenosis in patients with left ventricular systolic dysfunction. J Am Coll Cardiol. May 2017;69(19):2383-2392. doi:10.1016/j.jacc.2017.03.02.