
Abstract
We report the case of a 37-year-old woman with no prior comorbidities who presented with progressive breathlessness, cough, and fever. Clinical examination revealed icterus and bilateral pitting pedal edema. The patient had palpable axillary, cervical lymphadenopathy, and thyromegaly. Cardiovascular examination showed elevated jugular venous pressure with muffled heart sounds, suggestive of cardiac tamponade physiology. Further evaluation confirmed acute cardiac tamponade secondary to pericardial effusion in the setting of Graves’ disease. This presentation is rare and potentially life-threatening if not recognized and managed promptly. This case highlights an unusual cardiac manifestation of Graves’ disease and underscores the importance of considering endocrine etiologies, particularly thyrotoxicosis, while evaluating patients with pericardial effusion and cardiac tamponade.
Introduction
The etiologies of pericardial effusion are manifold, including lymphoproliferative disorder, connective tissue disorder, metastasis, tuberculosis, and hypothyroidism. The protean cardiovascular manifestations in hyperthyroid illness are as follows: tachycardia; tachyarrhythmia like atrial fibrillation, supraventricular tachycardia, atrial flutter; high-output cardiac failure; hypertension, and tachyarrhythmia-induced cardiomyopathy. It is uncommon for Graves’ disease to present as a massive pericardial effusion going in for catastrophic cardiac tamponade. The plausible mechanism includes autoimmune pericarditis, increased capillary permeability due to thyrotoxicosis, and deposition of glycosaminoglycans, like chondroitin sulfate and hyaluronic acid, which, by their hygroscopic nature, cause seepage of fluid into the pericardial sac. A high index of clinical suspicion and prompt aggressive treatment with emergency pericardiocentesis, steroids, beta-blockers, and anti-thyroid drugs are needed to tide over the thyroid storm associated with cardiac tamponade.
Case Report
A 37-year-old female presented to our hospital with complaints of breathlessness, fever, cough, chest tightness, and easy fatiguability of 1 week duration. She also reported significant loss of weight and loss of appetite over the past 1 month. No prior comorbid illness.
Family history revealed that her mother expired 5 years ago due to metastatic breast cancer.
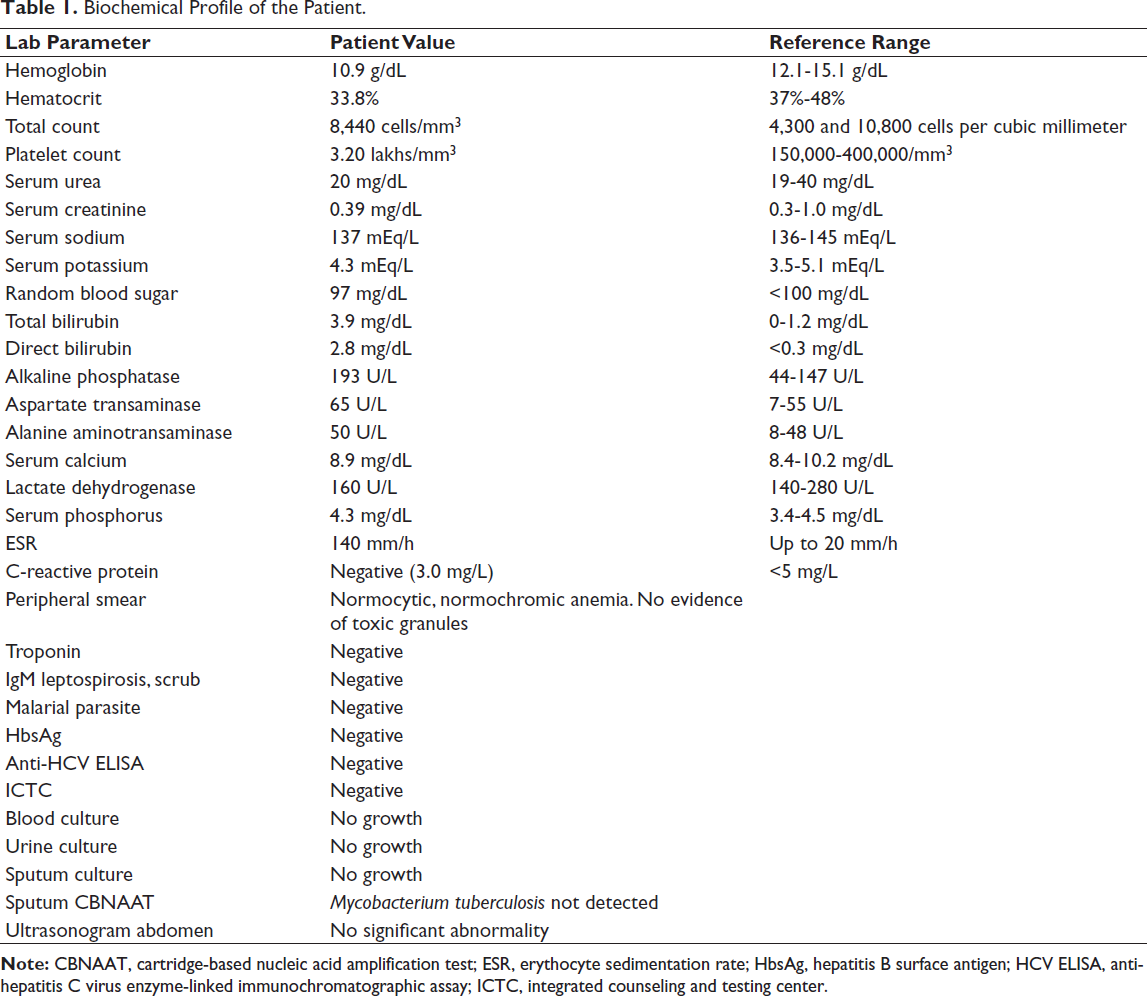
On clinical examination, the patient was conscious, oriented, febrile, dyspneic, tachypneic, and diaphoretic. Icterus and bilateral pitting pedal edema were present. Left-sided level 2, 3, and 4 multiple matted cervical nodes were palpable and the largest of them measured, 2.5 × 1 cm. The left axillary node was palpable (2 × 1 cm). No breast lump was palpable. Thyromegaly was noted. There was no evidence of cyanosis and clubbing. Heart rate was 140/min, respiratory rate was 25/min, blood pressure was 130/80 mmHg, oxygen saturation was 89% at room air, and jugular venous pressure (JVP) was elevated. Capillary blood glucose was noted to be at 123 mg/dL. Examination of the cardiovascular system revealed muffled S1 and S2 heart sounds. Evaluation of the other systems was normal. The biochemical investigations are summarized in Table 1.
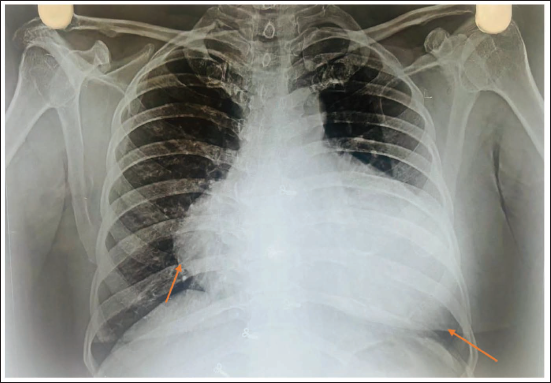
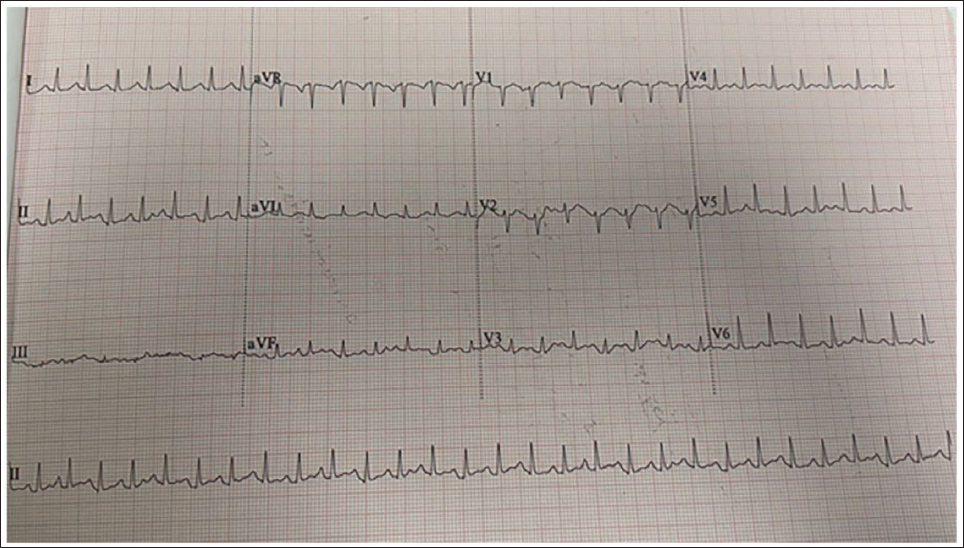
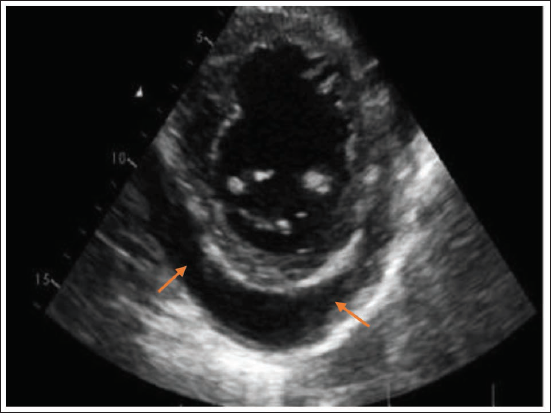
Chest X-ray (Figure 1) revealed an enlarged cardiac silhouette. Electrocardiogram (Figure 2) showed sinus tachycardia with low-voltage complexes in the chest leads and electrical alternans in lead V3. Echocardiography (Figure 3) showed an ejection fraction—60%, normal left ventricular systolic function, and massive pericardial effusion with collapse of the right atrium and right ventricle. Respiratory variation in tricuspid and mitral inflow velocity was present. The echocardiographic findings were suggestive of cardiac tamponade.
Chest Radiograph Showing Enlarged Cardiac Silhouette. The Arrows Mark the Pencil Border of the Pericardium Suggesting Effusion.
Electrocardiogram Showing Sinus Tachycardia, Low Voltage Complex on the Chest Leads and Electrical Alternans in Lead V3.
2D Echocardiography Short Axis View of the Heart Showing Echo Lucent Space (Arrows) Showing Pericardial Effusion.
Biochemical Profile of the Patient.
As a life-saving measure, immediate emergency therapeutic pericardiocentesis was done. A pigtail catheter was inserted into the pericardial cavity, and serous fluid of 260 mL was drained.
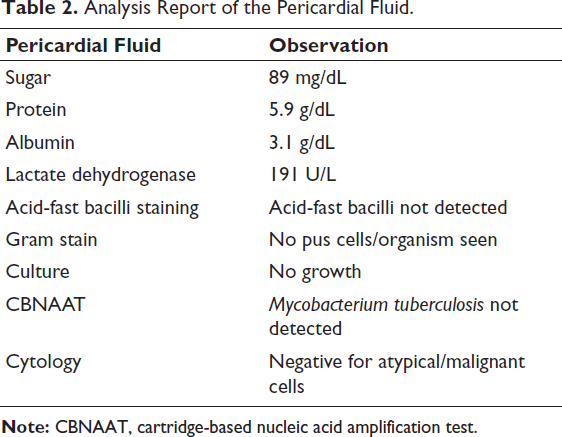
The pericardial fluid laboratory analysis was exudative. The culture of the pericardial fluid did not reveal growth of microbes. Pericardial fluid was negative for a broad viral targeted multiplex polymerase chain reaction panel covering enterovirus, adenovirus, cytomegalovirus, Epstein–Barr virus, herpes simplex virus, influenza, and parvovirus B19, ruling out infectious etiologies of pericardial effusion.
The pericardial fluid and sputum cartridge-based nucleic acid amplification test (CBNAAT) did not detect Mycobacterium tuberculosis, ruling out the tubercular etiology of pericardial effusion.
Pericardial fluid cytology was negative for atypical or malignant cells, ruling out malignancy/metastasis as the cause of pericardial effusion (Table 2).
Analysis Report of the Pericardial Fluid.
Anti-nuclear antibody profile was negative, thus ruling out connective tissue disorders, which can manifest as pericardial effusion.
Ultrasonogram of the neck showed multiple enlarged lymph nodes with preserved fatty hilum on the left side of the neck at levels IB, 2, 3, and 4, with the largest node measuring 2.5 × 1.2 cm. Ultrasonogram of the breast showed normal fibroglandular tissue with no focal lesion, indicating bilateral breast imaging-reporting and data system (BIRADS) 1 status. Ultrasonogram of the axilla showed an enlarged left axillary node measuring 2.1 × 0.7 cm, with preserved fatty hilum. Ultrasonogram of the inguinal region showed a few enlarged inguinal nodes, the largest measuring 1.3 × 0.8 cm, with preserved fatty hilum on the left side. Contrast-enhanced computed tomography scan of the thorax and abdomen did not reveal lymphadenopathy or features suggestive of malignancy. Fine needle aspiration cytology of the cervical and axillary lymph nodes showed reactive lymphadenitis. At this point, we were able to rule out nodal malignancies and lymphoproliferative disorders, which can manifest as pericardial effusion.
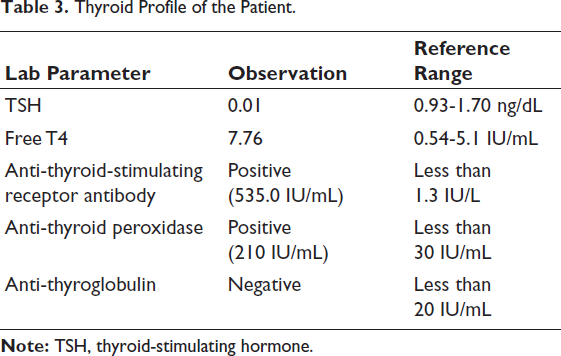
Since thyromegaly was noted, a thyroid function test was done. Free T4 was significantly elevated, and thyroid-stimulating hormone (TSH) was well suppressed, indicating hyperthyroidism. Ultrasonography of the thyroid showed thyroid imaging reporting and data system (TIRADS) 3 status. Anti-thyroid-stimulating hormone receptor and anti-thyroid peroxidase antibodies were elevated in high titers. Anti-thyroglobulin antibody was negative (Table 3). There was no evidence of thyroid dermopathy or thyroid-associated orbitopathy.
Thyroid Profile of the Patient.
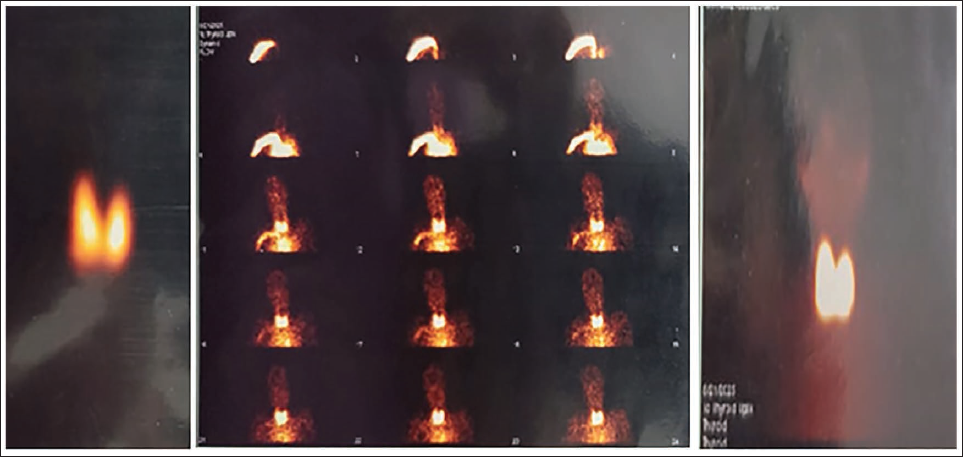
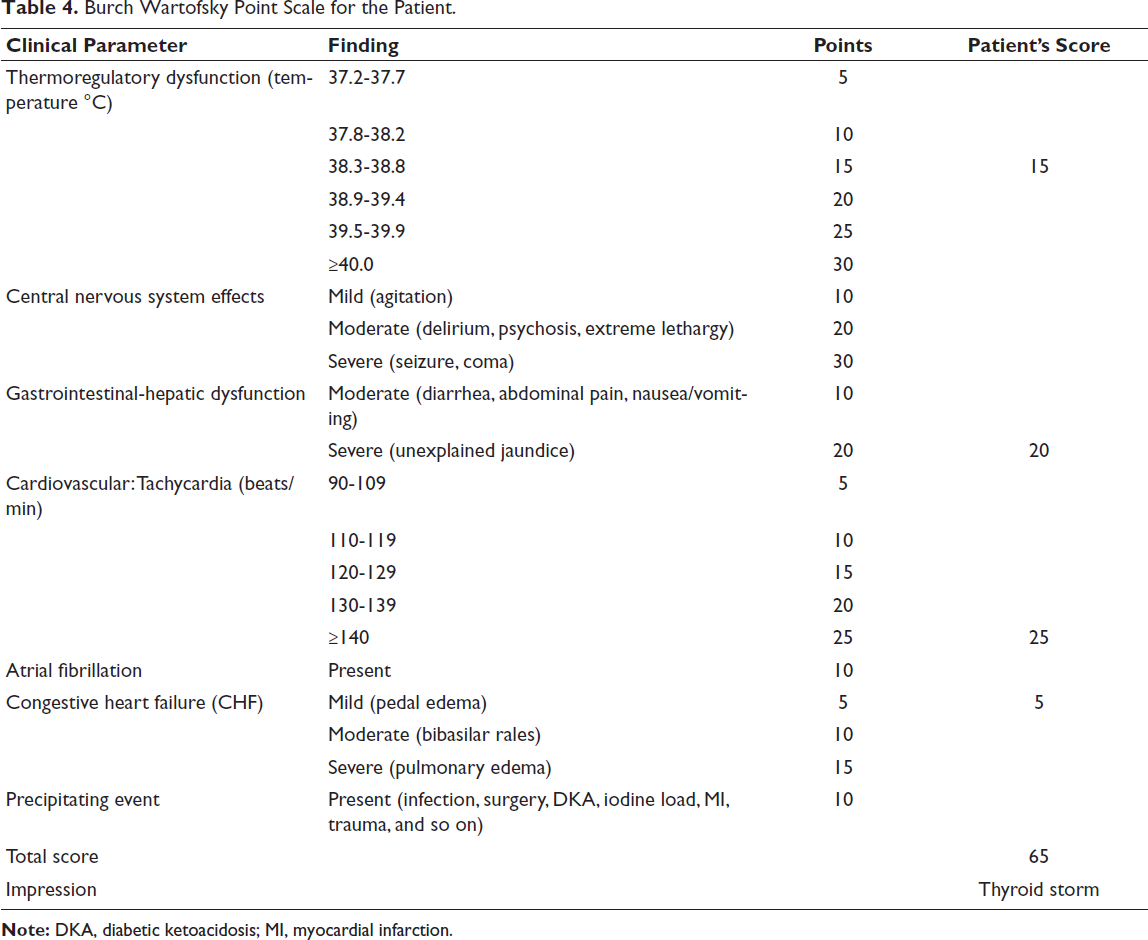
To assess the functional status of the thyroid gland, we did a radionucleotide TC99m thyroid scintigraphy scan. Early dynamic images demonstrated prominent blood flow in both lobes of the thyroid gland. Delayed static images demonstrated that the thyroid gland was enlarged and had intense radiotracer uptake of up to 16.9%. The findings of the radionucleotide scan (Figure 4) of the thyroid gland were compatible with Graves’ disease. When the clinical findings of the patient were matched onto the Burch Wartofsky Point Scale, we obtained a score of 65 points, strongly favoring the diagnosis of thyroid storm in our patient (Table 4).
Radionucleotide TC99m Thyroid Scintigraphy Showing Diffuse Enlargement of Both Lobes of Thyroid Glands with Intense Radiotracer Uptake.
Burch Wartofsky Point Scale for the Patient.
The patient was promptly treated with propranolol to combat the adrenergic sympathetic drive and injection of hydrocortisone, in view of thyroid storm, and carbimazole, an anti-thyroid drug blocking the peripheral conversion of T4 to T3.
Therefore, we would like to bring to the notice of a rare presentation which was encountered in our patient, hyperthyroidism secondary to Graves’ disease presenting upfront as a massive pericardial effusion going in for catastrophic cardiac tamponade.
Discussion
Graves’ disease is an autoimmune disorder characterized by the presence of autoantibodies against the TSH receptor (90%-100%), thyroid peroxidase (60%-70%), and thyroglobulin (30%-40%). The common clinical features encountered in Graves’ disease are weight loss, heat intolerance, diarrhea, menstrual irregularities, tremors, and ophthalmopathy. The protean cardiovascular manifestations in hyperthyroid illness are as follows: tachycardia; tachyarrhythmia, like atrial fibrillation, supraventricular tachycardia, atrial flutter; high output cardiac failure; hypertension; and tachyarrhythmia-induced cardiomyopathy.1-10 Cardiac tamponade as the presenting manifestation of Graves’ disease is sparsely reported in the literature, making this a rare and clinically novel manifestation.
The several proposed mechanisms of pericardial effusion in Graves’ disease include autoimmune pericarditis, increased capillary permeability, and interstitial fluid shifts as a part of thyrotoxicosis leading to pericardial fluid accumulation; deposition of glycosaminoglycans, like chondroitin sulfate and hyaluronic acid, which, by their hygroscopic nature, causes seepage of fluid into pericardial sac, is analogous to what happens in thyroid orbitopathy and dermopathy.1, 4, 5, 7-10
The pericardial fluid is usually serous and transudative in nature in case of Graves’ disease. It is imperative to rule out other coexistent causes of pericardial effusion that might impact the course of the clinical illness, like lymphoproliferative disorders, connective tissue disorders, metastasis, infection, and tuberculosis, particularly in endemic areas.1-10
The cause of icterus in our case is due to cholestatic and/or congestive hepatopathy, not primary liver disease. Liver dysfunction usually reverses with a euthyroid state. It is also prudent to remember that normotension does not rule out tamponade, as the sympathetic overdrive in the setting of thyroid storm maintains the blood pressure.
It is also important to note that the occurrence of thyroid eye disease and dermopathy might antedate, coincide, or postdate the occurrence of other clinical manifestations encountered in Graves’ disease.2, 5, 6
Clinicians must also actively search for occult causes, like infection, iodine exposure, surgery, withdrawal of anti-thyroid drugs, diabetic ketoacidosis, and sepsis, which might precipitate thyroid storm.1-5, 7
There can occur a temporal association between cardiac tamponade and thyroid storm, as was encountered in our case. It is prudent for clinicians to understand that cardiac tamponade can more often herald the onset of catastrophic and life-threatening thyroid storm.
The crux of the management lies in treating the thyroid storm and the tamponade simultaneously. A prompt diagnosis with electrocardiogram, echocardiography, and thyroid function tests, alongside removal of the mechanical obstruction by life-saving emergency pericardiocentesis, is of pivotal importance to tide over the tamponade. Initiate beta-blockers to combat the excess adrenergic drive and catecholamine activity. Anti-thyroid drugs like carbimazole/propylthiouracil and steroids like hydrocortisone block the peripheral conversion of T4 to the biologically more active T3. The treatment for thyroid storm is stopped when the patient is afebrile, hemodynamically stable, with no features of heart failure, has normal mentation and is tolerating oral intake. Definitive treatment options like radioiodine ablation of the thyroid can be considered after stabilization and improvement of the general condition of the patient.1-10
Early recognition and prompt aggressive treatment involving a multidisciplinary team of cardiologists, endocrinologists, and critical care physician improve outcomes and decreases morbidity and mortality.1-10
Conclusion
With the timely diagnosis and prompt initiation of treatment, there was a dramatic resolution of the symptoms, and the patient started doing well. At the time of discharge, the electrocardiogram revealed sinus rhythm and normalization of voltage; there was no pericardial collection noted on echocardiography. The patient was discharged with a prescription for carbimazole and propranolol and is doing well on further follow-up.
Footnotes
Acknowledgment
The authors are deeply grateful to their professors for their valuable guidance and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting an individual case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written patient consent for publication of the case and images has been obtained from the patient.