
Abstract
Background:
Pericardial effusion (PE) is an abnormal fluid volume in the pericardial space and is a common clinical entity. The incidence of PE is estimated diversely and depends on risk factors, etiologies, and geographic locations.
Objectives:
This study aimed to assess the clinical characteristics, etiologic spectrum, echocardiographic features, and outcomes among patients with different types of PE.
Method:
This retrospective observational study included 93 patients with confirmed PE. Their medical records were reviewed in the hospital information system of Mogadishu Somali Turkish Training and Research Hospital between April 2022 and September 2022. Patient demographics, clinical characteristics, chest X-rays, echocardiography, laboratory findings, management approaches, and outcome reports were reviewed and recorded.
Results:
Out of the 3000 participants, 3.1% (n = 93/3000) met the definition of definitive PE. In this study, we included 51 females and 42 males. Among the patients, 86% (n = 80) had at least one comorbidity, with diabetes (38.7%) and hypertension (37.6%) being the most common. The most frequently reported clinical presentation findings were shortness of breath (67.7%), chest pain (49.4%), cough (47.3%), and palpitations (47.3%). Cardiac tamponade developed in 9.7% (n = 9) of the patients. Pericardial taps were performed in 64.5% of the cases. Our analysis showed that the most common cause of PE was cardiac disease (n = 33, 35.4%), followed by tuberculosis (TB) (n = 25, 26.8%), uremic pericarditis (n = 24, 25.8%), and hypothyroidism (n = 10, 10.7%). Regarding the severity of PE based on echocardiographic findings, nearly half of the patients (n = 46, 49.4%) had mild PE, whereas 26.8% (n = 25) had moderate PE, and 23.6% (n = 22) had severe PE. Two-thirds of the cases (66.6%) were managed with furosemide, 48 (51.6%) patients were treated with an anti-inflammatory, hemodialysis was performed in 24 (25.8%) patients and antituberculous medications were administered to 7 (7.5%) patients. Out of the 93 patients, 24 (25.8%) died during the hospital stay. It was determined that the mortality risk of patients with renal failure was 7.518 times higher than those without (p = 0.004), and the risk for those with TB was 5.554 times higher than those without (p = 0.011). Other variables were not influential on mortality (p > 0.050).
Conclusion:
Our study results demonstrate the epidemiological profile of PE in Somalia. The leading causes of PE were cardiac diseases, uremic pericarditis, TB, and hypothyroidism. PE is a significant cause of morbidity and mortality in Somalia, especially in individuals with renal failure and TB infection.
Introduction
The pericardial cavity is a potential space between two layers of serous pericardium surrounding the heart. It typically contains a small amount (25–35 ml) of ultrafiltration of plasma, which reduces surface tension and lubricates the heart, facilitating its free movement. 1
Pericardial effusion (PE) is an abnormal accumulation of fluid in the pericardial space and is a common clinical condition. It can be asymptomatic or present as a life-threatening cardiac tamponade, which results from increased intracardiac pressure, progressive limitation of ventricular diastolic filling, and reduced cardiac output. 2 The most prominent clinical presentations of PE include shortness of breath, fatigue, and chest pain. Patients may also experience peripheral oedema, pulsus paradoxus, Kussmaul’s sign, and pericardial friction rub upon auscultation.3,4
The incidence of PE varies depending on risk factors, etiologies, and even geographic locations. A wide range of conditions can lead to PEs, including chronic heart failure, chronic pericarditis, nephrotic syndrome, hepatic cirrhosis, neoplasms (with or without direct pericardial involvement), myxedema, renal insufficiency, pregnancy, aortic or cardiac rupture, tuberculosis (TB), trauma, and idiopathic cases. 5 In general, PE can be categorized as exudate or transudate, as well as hemorrhagic or chylous effusion. Exudate is commonly seen in inflammatory diseases such as infections, neoplasms, uremia, trauma, surgical procedures, radiation therapy, autoimmune conditions (e.g. systemic lupus erythematosus), or myocardial infarction. Transudate is associated with heart failure and liver failure. Hemorrhagic effusion occurs in traumatic vascular or cardiac events, such as acute aortic injury, aortic dissection, acute cardiac injury, cardiac trauma, and malignancies. On the other hand, chylous effusion is infrequent and can occur when there is damage or obstruction of the lymphatic drainage system, often seen in malignancies. 6
Several studies have identified factors contributing to poor prognosis in PE, including fever (>38°C), immunocompromised status, severe PE, cardiac tamponade, tuberculous pericarditis (especially in patients coinfected with HIV), and the use of oral anticoagulant therapy.7–9
In the present study, we retrospectively evaluated the medical records of consecutive patients who underwent echocardiography for therapeutic or diagnostic reasons at a tertiary teaching hospital between 2016 and 2020. This study aimed to assess the clinical characteristics, etiologic spectrum, echocardiographic features, and outcomes among patients with different types of PE.
Method
Study setting, design, and population
This retrospective observational study was conducted at Mogadishu Somali Turkish Training and Research Hospital (MSTTRH) in Mogadishu, Somalia. Three thousand patients underwent echocardiographic investigations at MSTTRH from April 2022 to September 2022. The medical records of 93 patients confirmed to have different types of PE were reviewed by the hospital information system.
Eligibility criteria
Our study included only patients who underwent echocardiography and met the echo criteria for PE. We excluded young patients under 18 years of age, participants with incomplete records, and those who did not have a definitive diagnosis.
Study procedure
Patient demographics and clinical characteristics were recorded on the data collection sheet. Chest X-rays (CXR), echocardiography, and laboratory reports were reviewed and documented. The patients’ treatments and outcomes were also recorded on the data collection sheet. Outcome information was retrieved whenever available. The primary endpoint of the study was defined as in-hospital mortality. Data collection was completed over 3 months.
Diagnosing significant PE based on clinical findings alone can often be challenging. All patients with PE underwent a standard transthoracic echocardiogram. Two-dimensional transthoracic echocardiography is the preferred radiological modality for evaluating PE and cardiac tamponade, and it should also be used to guide pericardiocentesis.10,11
On echocardiography, a PE appears as an echo-free space behind the heart with no pericardial motion. Effusions are commonly described as small (<100 ml) or (1 cm), moderate (100–500 ml) or (2 cm), or large (>500 ml) or (>2 cm), based on a visual estimate of fluid volume, its location, and the size of the heart relative to the fluid space. 12 Features indicating the presence of cardiac tamponade include right atrial and right ventricular collapse during diastole and a swinging heart. 12 Other features include a dilated inferior vena cava with a lack of inspiratory collapse.
Computer tomography (CT) is a valuable additional modality when more precise localization and quantification of pericardial fluid are required, especially in complex or loculated effusions or a clot.11,13 Chest magnetic resonance imaging is rarely used as a primary radiology modality for evaluating PE. However, it provides a more precise description of PE’s localization and volume than an echocardiogram, similar to a CT scan.13,14 The researchers obtained the data as it was, without any modification, to enhance objectivity, and a double check was performed. Information bias was minimized by obtaining at least 95% of the required clinical documents. There was no selection bias, as all records were included.
Data entry and statistical analysis
Data analysis was performed using SPSS version 23.0 software. Continuous data are presented as mean ± SD, and categorical data as frequency (percentage). Patients were grouped based on their outcomes (survival and non-survival) to explore outcome-specific differences. Continuous data were compared using the Student’s t-test, and categorical data were compared using the chi-square or Fisher’s exact test. Binary logistic regression analysis was used to identify risk factors for in-hospital mortality. All variables found statistically significant in univariate analysis were included in the multivariate model. The results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). A p value of less than 0.05 was considered statistically significant.
Ethical consideration
Ethical permission to conduct the study was requested and obtained from Mogadishu Somali Turkish Training and Research Hospital (Ref: MSTH/10303). Since this was a retrospective study, consent forms were not required. However, personal identification information was protected during data collection. This study was conducted following the principles outlined in the Helsinki Declaration.
Results
Sociodemographic characteristics, prevalence, and comorbidities
A total of 3000 patients underwent echocardiography, of whom 93 met the criteria for PE and had no missing data. Their sociodemographic characteristics and comorbidities are summarized in Table 1. Among the 3000 participants, 3.1% (n = 93/3000) met the definitive PE definition. The participants were categorized into four age groups: 18–29 years (34.4%), 30–49 years (21.5%), 50–69 years (30.1%), and ⩾70 years (13.9%). A statistically significant difference was found between the age groups of the participants and the outcome (p = 0.022). The difference was observed in the distribution between the 18–29 age group and the 50–69 age group. A slight female predisposition was detected; 54.8% of all cases were female, whereas 45.2% were male, and there was no statistically significant difference between the gender distribution and outcome (p = 0.580). Regarding comorbidities, 86% (n = 80) of the patients had at least one comorbidity; 38.7% (n = 36) had diabetes mellitus; 37.6% (n = 35) had hypertension; and 36.5% (n = 34) had cardiomyopathy. A statistically significant difference was found between the distribution of comorbidities and the outcome variable (p = 0.004). The difference was observed in the distribution of those with diabetes mellitus, cardiomyopathy, and retroviral infection.
Examination of the distribution of the sociodemographic characteristics of the participants according to the outcome variable.

a and b, There is no difference between groups with the same letter.
Pearson chi-square test.
Multiple response.
Clinical presentation of the participants
The clinical presentation of the participants is shown in Figure 1, which displays the frequencies of clinical presentation categories according to the outcome. The blue columns in the figure represent survivors, and the frequencies of survivors in all categories were higher. Among patients with PE in the survival group, shortness of breath was the most common symptom (n = 44), followed by chest pain (n = 29) and cough (n = 26). Dyspnea, palpitation, cough, and chest pain were the most common presenting symptoms in patients in the non-survival groups, with n = 19, n = 18, and n = 17, respectively.

Clinical presentation of the participants according to the outcome variable.
Tamponade and pericardial tap findings of the participants
The findings of the tamponade and pericardial tap are presented in Table 2. Among the PE patients, 9.7% (n = 9) developed cardiac tamponade. There was no statistically significant difference between the distribution of tamponade status and the outcome variable (p = 0.690). The rate of tamponade in the survival group was 8.7%, whereas it was 12.5% in the non-survival group. There was also no statistically significant difference between the distribution of pericardial tap findings and the outcome variable (p = 0.703). The rate of not performing pericardial tap in the survival group was 47.8%, compared to 58.3% in the non-survival group. The rate of exudates in the survival group was 23.2%, whereas it was 16.7% in the non-survival group. The rate of transudates in the survival group was 76.8%, compared to 83.3% in the non-survival group.
Examination of tamponade and pericardial finding distributions according to outcome variable.

Fisher’s exact test.
Yates correction.
Etiological distributions according to the outcome variable
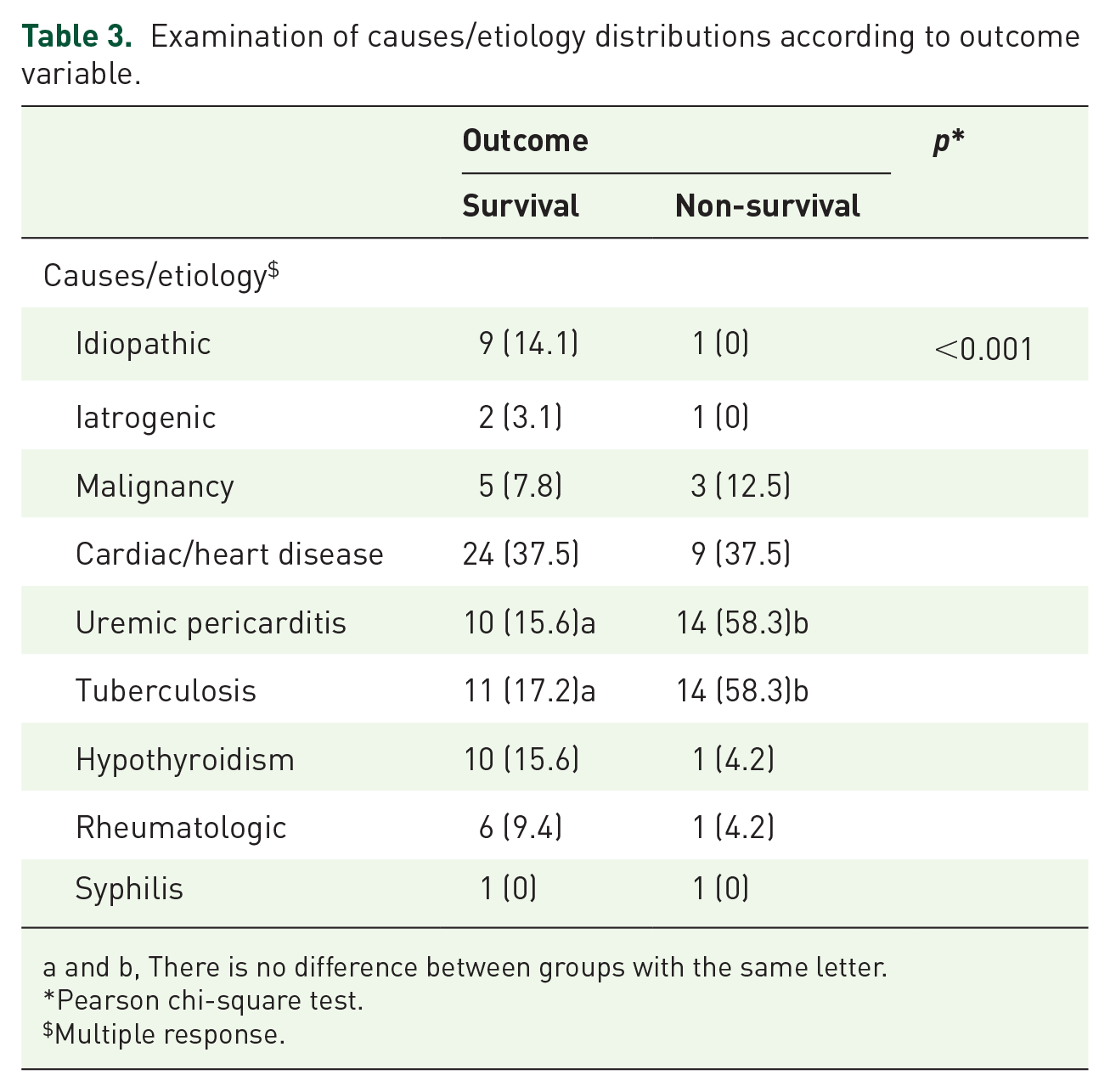
The etiological distributions according to the outcome variable are presented in Table 3. The most common cause of PE was cardiac disease (n = 33, 35.4%), followed by TB (n = 25, 26.8%), uremic pericarditis (n = 24, 25.8%), and hypothyroidism (n = 10, 10.7%). A statistically significant difference was found between the distributions of causes and etiology and the outcome variable (p < 0.001). The difference was observed in the distribution of those with uremic pericarditis and TB. The rate of those with uremic pericarditis in the survival group was 15.6%, compared to 58.3% in the non-survival group. The rate of those with TB in the survival group was 17.2%, compared to 58.3% in the non-survival group.
Examination of causes/etiology distributions according to outcome variable.
a and b, There is no difference between groups with the same letter.
Pearson chi-square test.
Multiple response.
Echocardiographic and radiological findings distributions
The distributions of echocardiographic and radiological findings are described. Based on echocardiographic findings, nearly half of the patients (n = 46, 49.4%) had mild PE, 26.8% (n = 25) had moderate PE, and 23.6% (n = 22) had severe PE. A statistically significant difference was found between the echocardiographic distributions and the outcome variable (p < 0.001) (Table 4).
Comparison of echocardiographic distributions by outcome variable.

a and b, There is no difference between groups with the same letter.
Pearson Chi-Square test.
On the other hand, according to the type of lesions on the CXR, cardiomegaly was the most common radiographic finding, present in 52 patients (54.1%). This was followed by bilateral pleural effusion in 25 patients (26.8%), left pleural effusion in 19 patients (20.4%), and right pleural effusion in 18 patients (19.3%). A statistically significant difference was found between the distribution of radiological findings and the outcome variable (p < 0.001) (Table 5).
Comparison of distribution of radiological findings according to outcome variable.

a and b, No difference between groups with the same letter.
Pearson chi-square test.
Multiple responses.
CXR, chest X ray; PE, pericardial effusion.
Management distributions according to outcome variables
Regarding the management of PE, out of the 93 patients, two-thirds of the cases (62 patients, 66.6%) were managed with furosemide, 48 patients (51.6%) were treated with an anti-inflammatory medication, 24 patients (25.8%) underwent hemodialysis, and 7 patients (7.5%) received antituberculous medications (Table 6). The distribution of management approaches did not differ according to the outcome variable (p = 0.071).
Comparison of management distributions according to outcome variable.

Pearson chi-square test.
Multiple response.
Factors predicting mortality
Among the 93 patients, 24 patients (25.8%) died during their hospital stay. A binary logistic regression analysis examined the risk factors influencing mortality. The univariate analysis observed that the risk of mortality increased by 1.024 times with each increase in age (p = 0.037). Patients with cardiomyopathy had a 2.701 times higher risk of mortality compared to those without (p = 0.041). Patients with uremic pericarditis had an 8.26 times higher risk of mortality compared to those without (p < 0.001). Correspondingly, patients with TB had a 7382 times higher risk of mortality compared to those without (p < 0.001). The risk of mortality was 21,176 times higher for patients with moderate PE compared to those with mild PE (p = 0.005). Patients with severe PE had a 96,429 times higher risk of mortality compared to those with mild PE (p < 0.001). Patients with right-sided pleural effusion on the CXR had a 7.495 times higher risk of mortality compared to those without (p < 0.001). Patients with left-sided pleural effusion on the CXR had a 3.54 times higher risk of mortality compared to those without (p = 0.020). However, bilateral pleural effusion did not significantly affect mortality (p = 0.062).
In the multivariate analysis, it was determined that patients with renal failure had a 7.518 times higher risk of mortality compared to those without (p = 0.004). Patients with TB had a 5.554 times higher risk of mortality compared to those without (p = 0.011). Other variables were not found to be significantly associated with mortality (p > 0.050) (Table 7).
Factors predicting mortality in pericardial effusion patients.
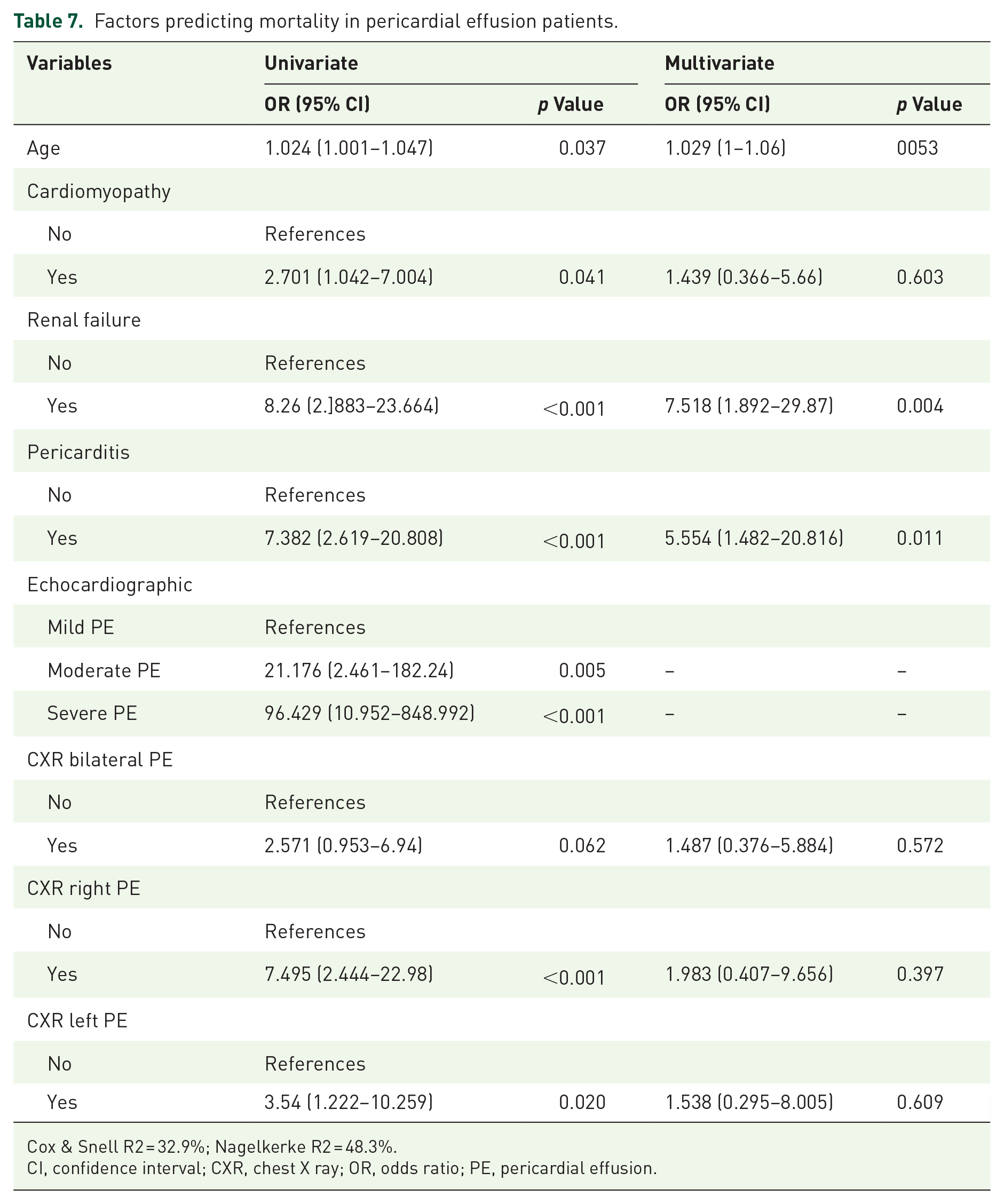
Cox & Snell R2 = 32.9%; Nagelkerke R2 = 48.3%.
CI, confidence interval; CXR, chest X ray; OR, odds ratio; PE, pericardial effusion.
Discussion
PE is a common finding in clinical practice, either as an incidental finding or a manifestation of systemic or cardiac disease. The spectrum of PEs ranges from mild symptomatic effusions to cardiac tamponade. Moreover, PE may accumulate gradually or suddenly.2,5
In this study, we included 93 patients (51 females and 42 males) diagnosed with different types of PE at the tertiary teaching hospital in Somalia. PE is most frequently found in the age group of 18–29 years (34.4%), followed by those aged 50–69 (30.1%). A study conducted by Pratiwi et al. 15 (Indonesia, 2008) showed that the most frequent age group was 11–40 years of age (51.9%), with the highest incidence in 21–30 years of age. In contrast to our findings, a study conducted by Petcu et al. 16 in Africa showed that the mean pericardial patient’s age is 60.5 years old. These differences can be explained by the difference in the incidence and prevalence of underlying diseases between Asia (Indonesia and Thailand) and Africa (Somalia).
This study has a slight female predominance (54.8%) of PE. Still, there was no statistically significant difference between the distributions of gender and outcome (p = 0.580). As stated in a study from Thailand on PE, the ratio between males and females was 1,2:1. 17
Regarding comorbidities, 86% (n = 80) of the patients had at least one comorbid, 36 (38.7%) had diabetes mellitus, 35 (37.6%) had hypertension, and 34 (36.5%) had cardiomyopathy. A statistically significant difference was found between the distribution of the types of comorbidities and the outcome variable (p = 0.004). A study from Colombia reported hypertension (41%), followed by malignancy (31%), chronic kidney disease (20%), and heart failure (16%) as the most observed comorbidities. 18
In the present study, the most common clinical presentation was shortness of breath (74.3%), chest pain (31.2%), and cough (28%). Studies from Kashmir 19 and Bihar 20 reported tachycardia followed by breathlessness as the most observed clinical feature.
According to our study, 9.7% (n = 9) of PE patients experienced cardiac tamponade. About 49.5% of patients had undergone pericardial taps. The exudate rate was 20.5%, whereas the transudate rate was 78.5% in both the survival and non-survival groups.
In a retrospective cross-sectional study from Ethiopia with a total population sampling of 204 patients, pericardial taping was done in 32.84% (67/204). PE was ascertained to be an exudate in 31.86% (65/204). 3 In a 1-year retrospective observational study of 70 patients with PE from a tertiary care center in India, conducted between August 2016 and July 2017, it was discovered that 17 (24.3%) of the patients had tamponade, which was determined through clinical and echocardiographic evaluation. 20
Our analysis showed that the most common cause of PE was cardiac disease (n = 33, 35.4%), followed by TB (n = 25, 26.8%), uremic pericarditis (n = 24, 25.8%), and hypothyroidism (n = 10, 10.7%).
Studies conducted in Ethiopia 3 and India 21 diversely revealed TB as the leading etiological factor, with a prevalence of 27.3% and 57.5%, respectively. These findings do not mean that TB prevalence is high in these Ethiopian and Indian regions, not in Somalia. However, our hospital does not admit TB patients because we do not have many isolation rooms; unless the patient’s condition cannot be treated elsewhere, TB patients are referred to the TB center. In addition, the risk of TB is now confounded by HIV coinfection. HIV, due to its ability to destroy the immune system, has frequently been implicated as a principal cause for the recent resurgence of TB worldwide. It should be noted that HIV infection continues to rise worldwide, increasing the incidence of PE diagnoses related to this condition.22,23 The study by Sagristà and his friends included 322 patients; the most common diagnosis was idiopathic (20%), neoplastic (13%), post-myocardial infract (8%), uremia (6%), collagen vascular disease (5%), and tubercular (2%). 24 In another retrospective study on the diagnosis and treatment of PEs in Turkey, the most common causes of PE were uremic pericarditis (n = 158, 43%), idiopathic and undefined pericarditis (n = 81, 22%), malignant processes invading the pericardium (n = 51, 14%), tuberculous pericarditis (n = 37, 10%), non-tuberculous bacterial pericarditis (n = 18, 5%), trauma (n = 15, 4%), and other (n = 8, 2%): rheumatoid arthritis in three patients, systemic lupus erythematosus in two, periarteritis nodosa in two patients, and hypothyroidism in one. 25
Regarding the severity of PE based on echocardiographic findings, nearly half of the patients (n = 46, 49.4%) had mild PE, 26.8% (n = 25) had moderate PE, and 23.6% (n = 22) had severe PE. In comparison with Dr. George Mukhari Academic Hospital experiences reported by Mphahlele and Motswaledi, mild PE (57.35%) was the most common severity form of PE based on echocardiographic findings, followed by massive PE (26.9%), and moderate PE (15.6%). 3 A study by Singh et al. 20 revealed that severe PE was the most common type of PE based on echocardiographic findings (77.1%, n = 54), followed by moderate PE (about 22.9%, n = 19). A case series of 368 patients with echocardiographic analysis revealed mild effusion in 15 (4%) patients, moderate effusion in 158 (43%) patients, and severe effusion in 195 (53%) patients. 25
In our findings, as stated by the type of lesions on the CXR, cardiomegaly was the most common radiographic finding and was presented in 52 (54.1%) patients, followed by bilateral pleural effusion (n = 25, 26.8%), left pleural effusion (n = 19, 20.4%), and right pleural effusion (n = 18, 19.3%). Several studies have evaluated the radiographic findings of patients with PE. A single-center observational study included 102 patients presenting with moderate-to-severe PE over 2 years, from March 2012 to February 2014, and found that cardiomegaly on CXR was the most radiologic finding, which agreed with our findings. 19 Mphahlele and Motswaledi 3 reported that cardiomegaly on CXR is the most common radiologic finding for about 96.4% of PE.
Considering PE management in our data, two-thirds of the cases (n = 62/93, 66.6%) were managed with furosemide, 51.6% (n = 48/93) were treated with an anti-inflammatory, hemodialysis in 25.8% (n = 24/93), and antituberculous medications in 7.5% (n = 7/93). Determining whether tamponade is present or if characteristics suggest a high likelihood of the development of tamponade shortly is the most crucial first step in the management of PE. Additionally, drainage of PEs has a low diagnostic yield (7%) and no therapeutic effect in the absence of true tamponade or high-risk features, according to Swanson et al and Gluer et al.26,27
A prospective cohort A study of one hundred consecutive cases of idiopathic chronic large PEs evaluated from 2000 to 2015 in three Italian tertiary referral centers for the management of pericardial diseases revealed that pericardiocentesis was the most common management type (n = 30/100, 30.0%), followed by a pericardial window in 12 cases (12.0%), and pericardiectomy in 3 patients (3.0%). 28
The prognosis of PE depends on the underlying aetiology. 24 In the present study, the outcome of PE patients remains poor, with hospital mortality rates of 25.8%. The mortality risk of patients with renal failure was 7.518 times higher than that of those without (p = 0.004). It was determined that the mortality risk of those with TB was 5.554 times higher than that of those without (p = 0.011).
Yaqoob et al. 19 reported on the etiology and outcomes of PE in Kashmir; out of 102 patients, 13 (12.7%) died during hospital stays. The underlying etiology of these patients included malignancy (n = 6), uremia (n = 3), TB (n = 1), post-MI (n = 1), pyogenic PE (n = 1), and congecsive cardiac failure (n = 1).
In a research conducted in Somalia involving patients with end-stage renal disease who were undergoing regular hemodialysis, it was revealed that pericarditis and PE were the third most frequently observed complications among these individuals. 29
Among these patients who died, nine had cardiac tamponade and had undergone pericardiocentesis. 19 Another study of the clinical and laboratory profiles of adult PE patients at Academic Hospital in Ethiopia found that the hospital mortality rate was 8.82%. 3
Limitations and strengths
Our study had several limitations. First, the findings cannot be generalized because this study was conducted at a single center. Second, the study was retrospective. Third, the sample size of the population may have needed to be larger to detect statistically significant differences. Despite these limitations, PE remains a public health challenge, particularly in low-income sub-Saharan African countries. The prevalence, etiological spectrum, echocardiographic features, and outcomes among patients with different types of PE in Somalia have yet to be examined due to the lack of a national registry system, limited knowledge and diagnostic tools, and the unestimated impact of the disease in the country. To our knowledge, this is the first study conceived to emphasize the clinical characteristics, etiological spectrum, echocardiographic features, and outcomes among patients with different types of PE at a tertiary teaching hospital in Somalia between 2016 and 2020. Although the final diagnosis of the cause of PE should be based on specific clinical data, as indicated in clinical guidelines,11,15 the results of the present study may assist in the initial assessment.
Conclusion
The results of our study demonstrate the clinical profile of PE in Somalia. We observed various clinical features associated with PE, with shortness of breath, palpitations, cough, and chest pain being the most common. The foremost causes of PE were cardiac diseases, uremic pericarditis, TB, and hypothyroidism. PE represents a significant cause of morbidity and mortality in Somalia, particularly among individuals with renal failure and those infected with TB.