
Abstract
We present the case of a woman in her mid-50s with suspected arrhythmic syncope while she was driving owing to fever-induced Brugada syndrome. The patient was appropriately managed with prompt antipyretic treatment and an implantable cardioverter-defibrillator. Clinicians should maintain a high index of suspicion for Brugada syndrome in febrile patients presenting with ST-segment elevation and syncope, even in trauma settings. Prompt electrocardiographic monitoring, antipyretic therapy and consideration of implantable cardioverter-defibrillator implantation are crucial in management.
Case Description
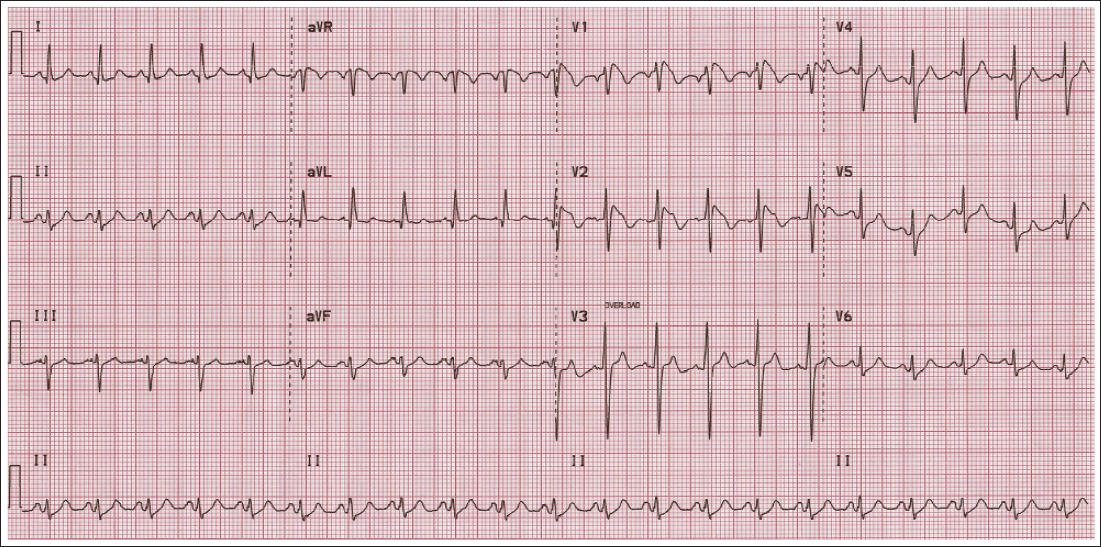
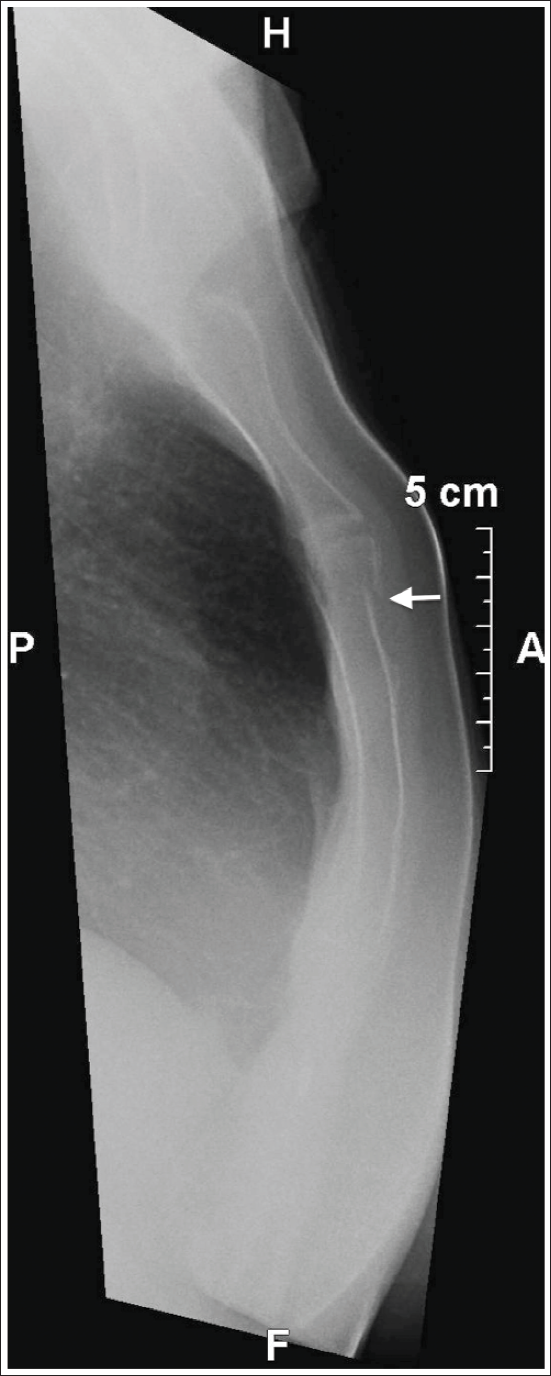
A 56-year-old woman arrived at our hospital by ambulance following a road traffic accident. She was wearing her seat belt at the time of the accident and was fully conscious when paramedics arrived at the scene. On examination, her blood pressure was 140/80 mmHg, pulse rate was 126 beats per minute, respiration rate was 15 breaths per minute, and body temperature was 38.5°C. She was complaining of chest pain and had no memory of the car accident. She gave a 2-day history of fever and sore throat, for which she took no medications. She was previously healthy, denied any alcohol or illicit drug use, and had a family history of sudden unexplained death of her sister in her mid-30s during a febrile illness. Physical examination was unremarkable except for pharyngeal erythema and swelling and localized tenderness over the body of the sternum. Creatine kinase and creatine kinase-myocardial band isoenzyme levels were elevated, but troponin T levels on admission and after 6 h were normal. White blood cell and differential counts were normal, but serum C-reactive protein levels were elevated. The admission electrocardiogram (ECG) is shown in Figure 1. Chest radiography depicted a sternal fracture (Figure 2), but transthoracic echocardiography (TTE) was unremarkable. What is your diagnosis? What would be your next course of action? What is the most appropriate next step in management?
Admission 12-lead Electrocardiogram Showing >2 mm Coved-type ST-segment Elevation at the J Point in Leads V1 and V2 Comprising Concave Downsloping ST-segments With Respect to the Isoelectric Baseline Followed by a Negative T Wave That is Type I Brugada Pattern.
Lateral Chest Radiograph. Note the Discontinuation of the Radiopaque Structure on the Sternal Body, Suggesting a Sternal Fracture (Arrow).
Discussion
Our patient was diagnosed with fever-induced Brugada syndrome (BrS). The BrS constitutes an inherited arrhythmic entity associated with a risk of polymorphic ventricular tachycardia (VT) or ventricular fibrillation (VF), potentially leading to syncope and cardiac arrest or sudden cardiac death (SCD). 1 The electrophysiologic substrate underlying the BrS is transmural dispersion of repolarization in the right ventricular outflow tract due to dysfunction of certain cardiac ion channels and a decrease in gap junction Connexin43 expression. Up to 30% of patients test positive for mutations in the SCN5A gene, which causes a loss-of-function of the cardiac sodium channel (INa). Because accelerated inactivation of the INa can be temperature-sensitive, fever may reduce the inward sodium current, therefore unmasking a BrS phenotype. 2 According to the European Society of Cardiology Guidelines for the management of patients with ventricular arrhythmias (VAs) and the prevention of SCD, arrhythmic syncope is defined as a transient loss of consciousness due to cerebral hypoperfusion, characterized by a rapid onset, short duration, and spontaneous complete recovery, but highly suspicious for intermittent bradycardia, rapid supraventricular tachycardia, or VA. 3 In our case, we ruled out cardiac syncope owing to structural disorders such as severe aortic stenosis, hypertrophic or dilated cardiomyopathy, aortic dissection, obstructive cardiac tumors (i.e., prolapsing atrial myxoma), pulmonary embolus, and cardiac tamponade because TTE was unremarkable. Therefore, referring the patient for CMR was not considered necessary. Our patient had neither risk factors of coronary artery disease nor chest pain or any equivalent prior to the current presentation. Therefore, her clinical likelihood of coronary artery disease was very low. This, in combination with the absence of regional wall motion abnormalities on TTE and the normal serum levels of troponin on admission and after 6 h, suggested that cardiac ischemia-related syncope was unlikely. Yet, our patient’s family history of sudden unexplained death at a young age and presentation with a type I Brugada ECG pattern were suggestive of cardiac syncope, apparently of arrhythmic origin according to the European Society of Cardiology Guidelines for the diagnosis and management of syncope. 4 However, we also considered the possibility of our patient having suffered an episode of neurally mediated syncope, which is common in Brugada patients. 5 Although the relatively low predictive value of the clinical history in the differentiation between arrhythmic and neurally mediated syncope is well-known, one study reported that syncope during driving was a significant variable favoring an arrhythmic origin in Brugada patients, but still with a low positive predictive value (>10%) due to a low rate of events. 6 Subjecting our patient to a head-up tilt test (HUTT) could have helped diagnose neurally mediated syncope without, however, precluding an associated arrhythmic event because increased vagal tone may also act as a trigger for VF in such patients.5, 6 A positive HUTT result would therefore have had to be followed by an electrophysiological study to assess for inducible sustained VAs (VF, polymorphic or monomorphic VT) and therefore help decide upon the need for implantable cardioverter-defibrillator (ICD) implantation. 7 On the other hand, the data regarding the impact of electrophysiological studies on fever-induced BrS are scarce. Considering all of the above and the fact that fever poses a high risk of arrhythmic events for BrS patients, and after discussing all available means of risk stratification, including genetic testing targeting SCN5A mutations, with the patient, we refrained from subjecting her to a HUTT and decided to approach her as having suffered a suspicious arrhythmic syncope.
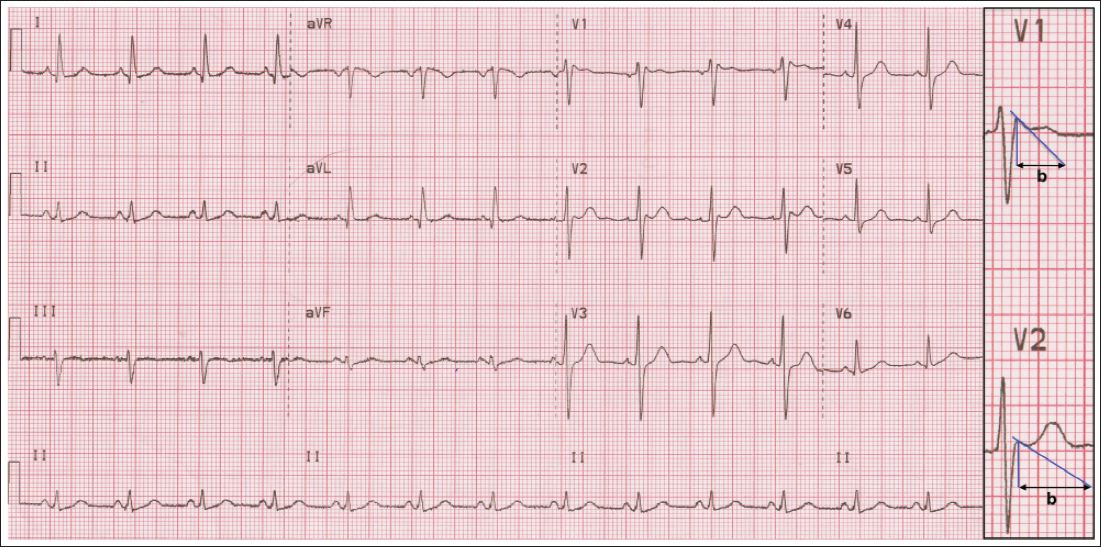
The patient, whose pretest probability of true BrS (family history of suspicious SCD; suspected arrhythmic syncope) was high, presented with a type I Brugada ECG pattern (Figure 1), which is diagnostic of BrS. Furthermore, her stable hemodynamic status, unremarkable TTE, and normal troponin levels made a diagnosis other than fever-induced BrS, such as traumatic aortic dissection with concomitant acute myocardial infarction, myocardial contusion, or a Brugada-like ECG pattern (i.e., Brugada phenocopy) due to acute myocardial ischemia or acute myopericarditis, unlikely. She was promptly prescribed antipyretic therapy and underwent continuous ECG telemetry monitoring without evidence of any VA. After defervescence, regression to a type III Brugada ECG pattern was observed (Figure 3), along with resolution of the upsloping ST-segment depression at the J point in leads II, aVF, and V4-V6 noted on admission. Given the angiographically normal coronary arteries demonstrated after defervescence, the ST-segment depression likely owed not to myocardial ischemia, but to the tachycardia per se, which makes the slope of phase 2 of the ventricular action potential steeper than normal, therefore resulting in differences of the potential persisting during most or all of repolarization. 8
Twelve-lead Electrocardiogram Obtained After Defervescence Showing an rSr’ Pattern in Leads V1 and V2, Followed by a Saddleback-type ST-segment Elevation (~0.5 mm) and a Positive T Wave That is a Type III Brugada Pattern Because of the Broad Base (>4 mm) of the Triangle of the r’ Wave 5 mm Below the Maximum Rise Point.
The diagnosis of BrS was further strengthened after defervescence, which helped establish the association between fever and type I Brugada ECG pattern. Therefore, our patient was diagnosed with probable/definite BrS as per a Shanghai score of >3.5 points (fever-induced type I Brugada ECG pattern [3 points], suspected arrhythmic syncope [2 points], and family history of suspicious SCD [1 point]). 9 Indeed, our patient’s Shanghai score of 7.0 points entailed a high risk of lethal arrhythmic events, estimated at 25% at 10 years. It is therefore plausible that our patient may have experienced arrhythmic syncope owing to a self-terminating culprit VA or aborted cardiac arrest owing to the conversion of the culprit VA to sinus rhythm after blunt chest wall trauma from a car seat belt.10, 11 Either way, she had a Class I indication for ICD implantation. 3 The patient was discharged home in good health after receiving a transvenous single-chamber ICD, and she was instructed to treat any future febrile conditions promptly with antipyretics. Genetic testing targeting SCN5A mutations, which not only are diagnostic of the BrS but also are associated with an increased risk of VT/VF, was recommended to the patient who has no living parents or siblings, nor children.3, 9 Clinicians should maintain a high index of suspicion for BrS in febrile patients presenting with ST-segment elevation and syncope, even in trauma settings. Timely and aggressive control of fever is crucial in preventing fatal arrhythmias, with fever-induced BrS leading to life-threatening arrhythmias, syncope, or cardiac arrest in 36% of patients. 12
Footnotes
Authors’ Contributions
Andreas Y. Andreou: Conceptualization: Lead; Data curation: Lead; Investigation: Lead; Writing—original draft: Lead; Writing—review & editing: Lead. Jesse Lee Zulberg: Data curation: Supporting; Investigation: Supporting; Writing—original draft: Supporting. Anna Angeliniadis: Data curation: Supporting; Investigation: Supporting; Writing—original draft: Supporting.
Data Availability Statement
The data underlying this article are available in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The corresponding author confirms that witnessed verbal consent for submission and publication of this case report, including images and associated text, has been obtained from the patient. The information provided in the article has been sufficiently anonymized so that neither the patient nor anyone else could identify the patient.