
Abstract
A 52-year-old dyslipidemic gentleman with no previous cardiovascular symptoms presented with acute typical angina for 4 h. The electrocardiogram (ECG) demonstrated ST-elevation in leads III, aVR, and V1, ST-segment depression in I, aVL, and V6, and hyperacute T-waves in leads V2-V6. Emergent angiography revealed critical single-vessel disease of the mid-left anterior descending artery (LAD) involving the first septal artery (S1) and proximal to the first diagonal artery (D1). This case illustrates how a significant ST-elevation myocardial infarction involving the mid-left anterior descending artery can potentially be underestimated in the electrocardiogram due to vector shifts related to the ramus intermedius artery. ST-elevation in leads III and aVF with upsloping ST-segment depression in V2-V6 may suggest a mid-left anterior descending artery acute anterior wall myocardial infarction in patients with a large ramus intermedius artery or an early obtuse marginal artery.
Keywords
A 52-year-old dyslipidemic gentleman with no previous cardiovascular symptoms has presented with acute typical angina for 4 h. He was hemodynamically stable at presentation with a pulse rate of 98 beats/min, blood pressure 138/80 mmHg, and a room air oxygen saturation of 99%. The first heart sound was soft; no other abnormalities were appreciated on the precordial examination. The lung bases were clear.
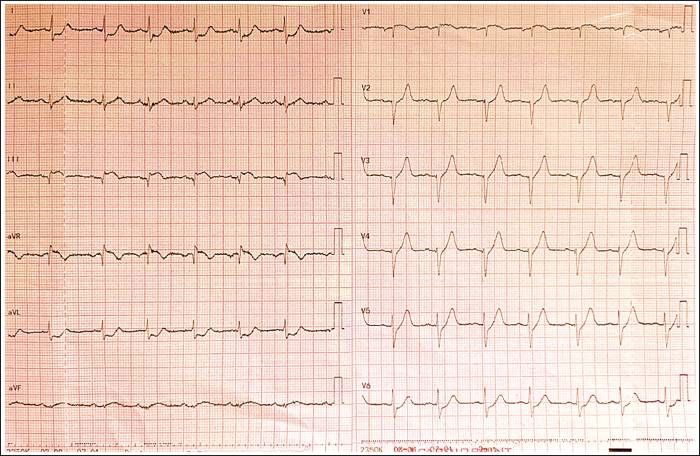
The electrocardiogram (ECG) demonstrated ST-elevation in leads III, aVR, and V1, ST-depression in I, aVL, and V6, and hyperacute T-wave abnormalities in leads V2-V6 (Figure 1). Poor R-wave progression was noted in leads V2-V5. Echocardiography revealed moderate left ventricular dysfunction with hypokinesia of the entire anterior wall and anteroseptum. The left ventricular ejection fraction was 40%. There was no clot in the cardiac chambers, no significant valve regurgitation, or pericardial effusion.
Twelve-lead Electrocardiogram of the Patient at Presentation with Acute Chest Pain.
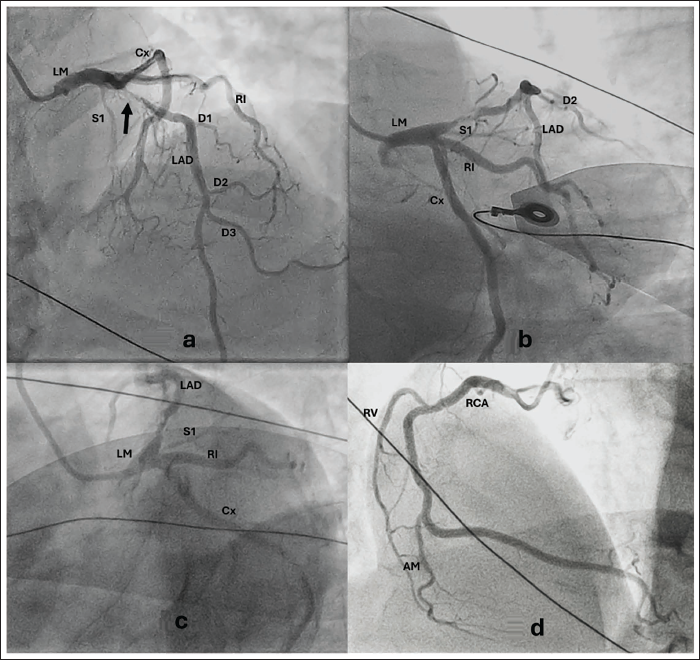
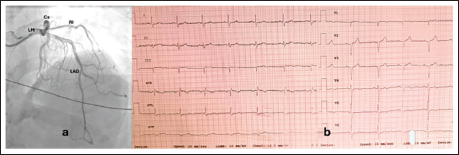
The patient was immediately taken up for primary angioplasty. Coronary angiography revealed a right-dominant coronary system. The left main coronary artery was a trifurcating vessel. While the left circumflex and ramus intermedius artery were normal, there was critical single-vessel disease of the mid-left anterior descending artery (LAD) involving the first septal artery (S1) and proximal to the first diagonal artery (D1) (Figure 2a, 2b). The right coronary artery was normal (Figure 2c). A 3.5 × 30 mm Zotarolimus-eluting stent was deployed in the LAD, with good results, and thrombolysis in myocardial infarction (TIMI) grade 3 flow was achieved (Figure 3a). Post-procedure ECG showed resolution of ST-segment changes, partial regeneration of R-waves, and biphasic T-waves in V4 and V5 (Figure 3b). The patient was discharged on day 4 post-angioplasty on dual antiplatelet therapy, high-intensity statin, angiotensin receptor neprilysin inhibitor, mineralocorticoid antagonist, beta-blocker, and sodium-glucose co-transporter-2 inhibitor. He remains asymptomatic at the 6-week follow-up, and the left ventricular ejection fraction improved to 45%.
Post-angioplasty Left Coronary Angiogram in Postero-anterior View with Cranial Angulation (Panel a) Demonstrating Good Result. Type 4 Left Anterior Descending Artery (LAD) is Noted. Panel b is the Post-angioplasty Electrocardiogram (ECG) Showing Resolution of ST-segment Changes, Partial Regeneration of R-waves, and Biphasic T-waves in V4 and V5.
The electrocardiogram depicts an unusual yet characteristic pattern with acute occlusion of the mid-LAD. The LAD from its ostium to the first major septal or diagonal is traditionally considered the proximal LAD; mid-LAD refers to the segment from the first major septal or diagonal to the origin of the distal major diagonal artery; distal LAD refers to the segment thereafter till its termination. 1 ST-elevation in V1, loss of R-waves, and hyperacute T-waves in the anterior precordial leads are markers to suggest an acute LAD occlusion. 2
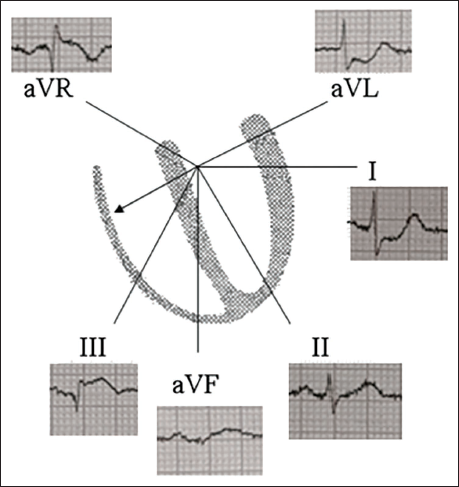
ST-segment deviation involving leads III and aVF is useful to localize acute LAD occlusion in relation to D1. While the sum of ST-depression in leads III and aVF ≥2.5 mm suggests an occlusion proximal to D1, ST-elevation in leads III and aVF points to an occlusion beyond D1. 3 In the index patient, with the lesion being proximal to D1, the ST-elevation in III and aVF is explained by the large ramus intermedius artery that perfused the diagonal territory. Consequently, the ST vector is directed inferiorly and rightward, mimicking a lesion distal to D1 (Figure 4). The ∑ (ST-segment deviation in aVR + V1 – V6) <0 is a marker of the lesion distal to S1. 3
Vectorcardiogram Demonstrating the Inferior and Rightward Net ST-vector in the Index Case.
Summary
The absence of ST-elevation in the precordial leads, barring V1, should not preclude the diagnosis of acute anterior wall myocardial infarction. The proposed etiology of the widespread upsloping ST-depression includes endocardial conduction delay related to an anatomical variation of Purkinje fibers, or the lack of activation of sarcolemmal adenosine triphosphate (ATP)-sensitive potassium channels by ischemic ATP depletion.4, 5 This case illustrates how a significant ST-elevation myocardial infarction involving the mid-LAD can potentially be underestimated in the ECG due to vector shifts related to the ramus intermedius artery. ST-elevation in leads III and aVF, with upsloping ST-depression in leads V2-V6, may suggest a mid-LAD acute anterior-wall myocardial infarction in a patient with a large ramus intermedius artery or early obtuse marginal artery.
Footnotes
Abbreviations
D1: First diagonal artery; LAD: Left anterior descending artery; STEMI: ST-elevation myocardial infarction; S1: First septal artery.
Authors Contribution
Dr. Pramod Kumar and Dr. Arun Gopalakrishnan prepared the manuscript. Dr. Sanjay Ganapathi contributed to the data acquisition and edited the manuscript. All authors approved the final version.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its amendments.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written consent was taken from the patient concerned for publication of this manuscript by masking patient identifiers.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.