
Abstract
Acute myocardial infarction (MI) in young people continues to be a major public health problem globally and in developing countries like India. A retrospective record-based study was conducted using data from 206 patients with acute MI (aged between 18 and 45 years) at Tulip Heart Centre, Anand, Gujarat, India. Demographic data, medical history, risk factors, clinical presentation, diagnosis, treatments (medications and surgery), and outcomes were recorded. Out of 206 enrolled patients (151 males and 55 females), a higher number of male and female patients were recorded in the age group of 41-45 years and from the urban area. ST-elevation MI was more prevalent in men (54.30% vs. 38.18%) with higher non-ST-elevation MI in women (45.69% vs 61.81%). Significant gender differences were observed in the prevalence of risk factors, with higher rates of diabetes mellitus (27.15% vs 41.81%, P < .05), hypertension (29.8% vs 54.54%, P < .05), and smoking (39.74% vs 7.27%, P < .05), while heart disease (12.58% vs 9.09%) and obesity (3.31% vs 3.63%) were not significantly different among both genders. Furthermore, data of clinical presentation, coronary obstruction, electrocardiogram changes, two-dimensional echocardiogram, regional wall motion abnormalities, and left ventricular ejection fraction were also not significantly different between the male and female groups. The antihypertensives, antiplatelets, antianginals, anticoagulants, and antihyperlipidemic drugs prescribed were similar in both men and women. The rates for re-hospitalization for surgery and follow-up were similar in both groups. Thus, the abovementioned findings highlight gender disparities, urban-rural differences, and risk factors in acute MI prevalence in young Indians. The modifiable risk factors causing MI need addressing so as to reduce the prevalence of MI in the Indian population.
Keywords
Introduction
For decades, cardiovascular diseases (CVDs) have been the leading cause of death globally. In 2021, 20.5 million people died from cardiovascular conditions, a figure that accounted for around one-third of all global deaths and was a significant increase from the 12.1 million CVD deaths recorded in 1990. 1 The global incidence of acute myocardial infarction (MI) has been steadily rising, with a prevalence of 3.8% in individuals under 60 years old.1, 2 In India, the age-standardized CVD death rate is 272 per 100,000, higher than the global average of 235 per 100,000.3, 4 Despite wide disparity in the prevalence of cardiovascular risk factors across different regions, CVD is characterized by a higher relative risk burden, an earlier age of onset, higher case fatality, and higher premature deaths in all parts of India, especially among young patients.5, 6 The increasing incidence of MI in younger individuals can be attributed to the presence of multiple modifiable risk factors, including elevated blood pressure, smoking, diabetes, obesity, high cholesterol, inactivity, an unbalanced diet, binge drinking alcohol, and related substances.5, 6
Both ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI) are caused by critical stenosis or total occlusion of coronary arteries (mostly due to thrombosis on atherosclerotic plaque) and manifest with a similar clinical presentation. Recent epidemiological studies suggest that the relative incidence of STEMI and NSTEMI is inversely correlated, with the incidence of STEMI decreasing and that of NSTEMI increasing with a prognosis that is worse at short-term follow-up for STEMI but comparable at long-term. Current management differs; as for STEMIs, immediate reperfusion is recommended, while for NSTEMIs, risk stratification is mandatory in order to stratify patients’ risk and then decide the timing for coronary angiography. Periprocedural and technical aspects of interventional management, as well as antithrombotic medications, are for the most part similarly implemented in the two types of MI. Both STEMI and NSTEMI can lead to long-term complications, such as cardiogenic shock, arrhythmias, reduced quality of life, and increased mortality rate. Percutaneous coronary intervention and timely reperfusion therapy with fibrinolytic for STEMI and coronary angiography in NSTEMI can significantly improve outcomes. However, the choice of treatment depends on the patient’s characteristics, clinical setting, comorbidities, and modality of revascularization. 7
Coronary artery disease that manifests at a younger age can have devastating consequences for an individual, the family, and society. While differences in symptomatology and pathophysiology between males and females are well-documented, a possible link between the two has not been studied extensively. The present study aims to review the rising trends in acute MI, with particular emphasis on the risk factors, clinical presentation, evaluation, and treatment of male and female young Indian patients.
Methodology
A record-based retrospective study was conducted at a tertiary care hospital in Anand, Gujarat. After obtaining approval from the ethics committee, data on acute MI cases registered from January 2022 to January 2024 were retrieved from the hospital’s case record register. Young patients (age 18-45 years) of either sex diagnosed with acute MI were included. Case records for these patients were accessed through their register numbers from the medical record department of the hospital, and their details were transferred to predesigned study forms. Data related to the patient’s demographic details (age and gender), presenting complaints on admission, previous history, risk factors, diagnostic tests (angiography, two-dimensional echocardiography [2D ECHO], and electrocardiography), treatments, and outcomes were included. The data were analyzed using SPSS (version 20.0), and Chi-square tests were performed to identify associations between variables, with a significance level set at P < .05. Descriptive statistics were calculated using frequencies and percentages.
Results
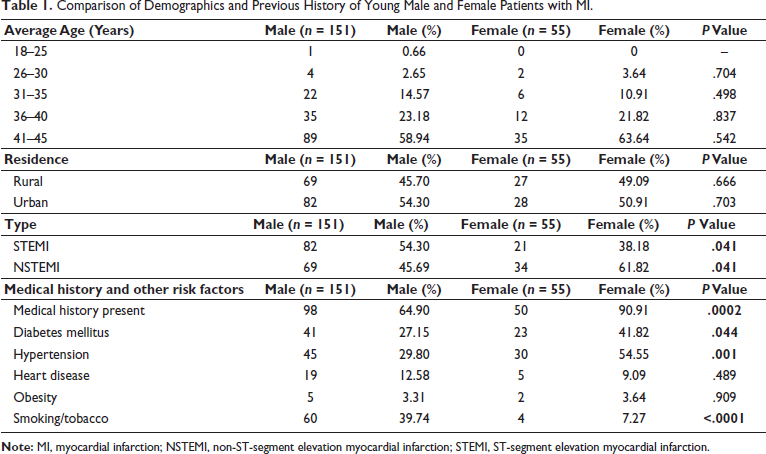
Out of the total 206 cases collected for the study, male (151) patients were higher than female (55) patients. The analysis of MI characteristics and history of comorbidities in both genders is shown in Table 1. No statistically significant difference was observed in the prevalence of MI between male and female age groups. The prevalence of STEMI was significantly higher in men (54.30% vs 38.18%) than in women, while females had a significantly higher frequency of NSTEMI than male patients (45.69% vs 61.81%). The frequency of medical history for comorbidities was significantly higher in females than in males. Medical history of hypertension, diabetes mellitus, heart disorders, and obesity in men and women are shown in Table 1. The proportion of women suffering from hypertension and diabetes was significantly higher than that of men. Further analysis revealed higher odds ratios (ORs) for hypertension (OR: 0.40, confidence interval [CI]: 0.21-0.76 vs OR: 2.48, CI: 1.30-4.75) and diabetes (OR: 0.67, CI: 0.36-1.32 vs OR: 1.47, CI: 0.75-2.76) in females compared to males, indicating a strong association of these risk factors with MI in females. Higher frequency and OR of smoking (OR: 8.40, CI: 2.95-22.5 vs OR: 0.11, CI: 0.04- 0.33) in males compared to females suggest a strong association between smoking and MI in males.
Comparison of Demographics and Previous History of Young Male and Female Patients with MI.
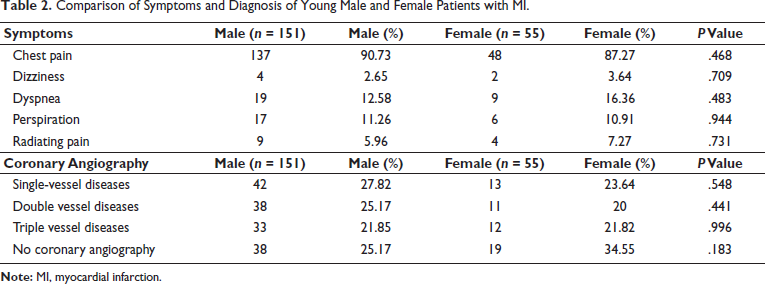
The frequency of symptoms experienced in both genders is shown in Table 2. A higher percentage of males (90.72%) reported chest pain compared to females (87.27%). Although atypical symptoms, such as dyspnea, dizziness, and radiating pain, were more common in females, no statistically significant difference in the frequency of symptoms was observed between the two sexes. Coronary angiography data showed that single-vessel obstruction (27.81% vs 23.63%), double vessel obstruction (25.1655% vs 20%), and triple vessel obstruction (21.85% vs 21.81%) were more observed in male patients compared to female patients. However, no statistically significant difference was found in these results (Table 2).
Comparison of Symptoms and Diagnosis of Young Male and Female Patients with MI.
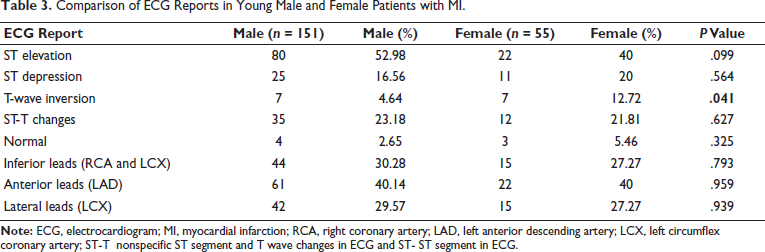
Data analysis of electrocardiogram (ECG) reports for both genders revealed no significant differences in ECG patterns except for T-wave inversion (Table 3).
Comparison of ECG Reports in Young Male and Female Patients with MI.
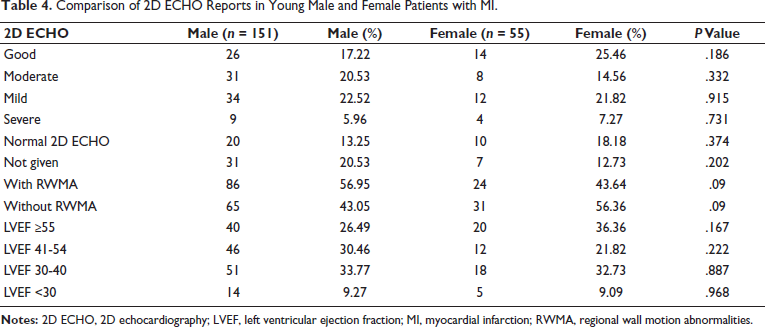
The 2D ECHO and left ventricular ejection fraction (LVEF) data for men and women are shown in Table 4. The distribution of LVEF categories—good LVEF (<55%), mild LVEF (41%-54%), moderate LVEF (30%-40%), and severe LVEF (<30%)—was not significantly different between men and women. Male patients had a higher prevalence of regional wall motion abnormalities (RWMA) compared to female patients. Although no statistically significant difference was observed between the two genders.
Comparison of 2D ECHO Reports in Young Male and Female Patients with MI.
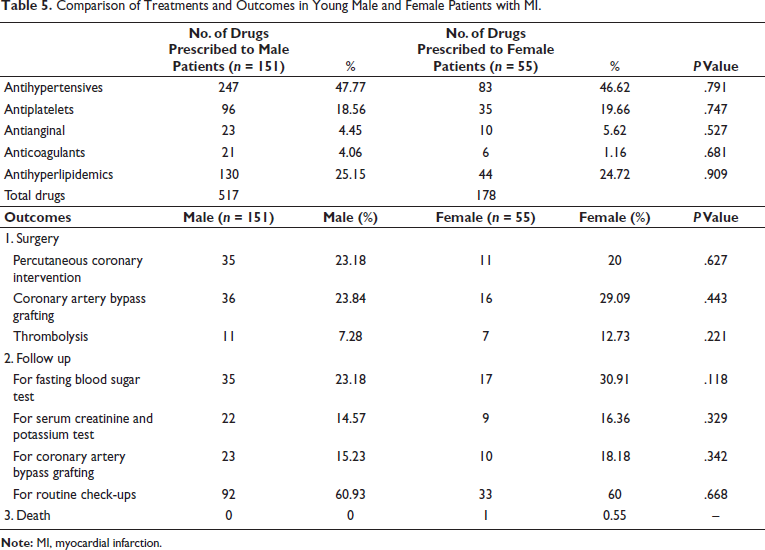
The frequency of drugs prescribed and treatment outcomes in young patients with MI are shown in Table 5. There was no statistically significant difference observed in the prescription of antihypertensive drugs (spironolactone, furosemide/torsemide, bisoprolol, amlodipine, clonidine, ramipril, and telmisartan), antiplatelets (clopidogrel, aspirin, and ticagrelor), antianginals (isosorbide dinitrate, ranolazine, and trimetazidine), anticoagulants (enoxaparin and rivaroxaban), and antihyperlipidemics (atorvastatin and rosuvastatin) between men and women. Outcomes were recorded in terms of re-hospitalization, follow-up, or death. Patients were re-hospitalized for surgery (percutaneous coronary intervention or coronary artery bypass surgery) or for thrombolysis using streptokinase. Data analysis showed that the frequency of re-hospitalization was not significantly different between male and female patients. Follow-up assessments included monitoring fasting blood sugar, serum creatinine, and potassium levels, as well as check-ups at the outpatient department or evaluations for surgery. No significant difference in follow-up data was observed between males and females, although mortality was reported in one female patient.
Comparison of Treatments and Outcomes in Young Male and Female Patients with MI.
Discussion
Although the risk of experiencing an MI increases with age, the incidence of MI in younger patients (<45 years of age) has progressively risen over time. In our study, MI was more frequently observed in men, particularly in the age group of 41-45 years, and ST-elevation MI was the most common presentation. Similar studies indicate that men are more susceptible to MI than women at younger ages, possibly due to the protective effects of hormones on the cardiovascular system in females.8–10 Research finding 10 have shown that females tend to have a lower atherosclerotic burden (ST-elevation MI) than males and a higher incidence of MI not related to plaque rupture, erosion, or increased microvascular resistance (non-ST-elevation MI), which was also observed in our study. The prevalence of MI was higher among urban patients than rural patients in our study, although this difference was not statistically significant, a pattern consistent with other studies from India.11, 12 Co-morbid conditions were more commonly observed in female patients with MI than in male patients with MI. Traditional risk factors, such as hypertension, diabetes, and obesity, were more prevalent in young females, whereas a history of heart disease and smoking was more commonly observed in young males, a pattern reflecting similar findings in Indian populations.12–15
In terms of symptoms, typical presentations such as chest pain were common in both sexes in the present study. However, females reported more atypical symptoms, such as dizziness, dyspnea, and radiating pain, consistent with earlier research. 11 Angiographic data showed a greater prevalence of single-vessel disease and multi-vessel involvement (double and triple vessel disease) in young male patients compared to young female patients. Anterior MI was most commonly observed, with the left anterior descending artery identified as the most affected coronary artery, consistent with findings from an Indian study. 15
In our study, the number of male patients with MI with “good” and normal 2D ECHO results was lower than that of female patients, although no statistically significant difference was observed in the overall echocardiography findings between the two groups. In both groups, 42% of patients had an LVEF <40%, a finding also reported in an Indian study. 16 RWMA were more frequent in male patients than in females, although this difference was not statistically significant. 17 Young male and female participants showed similar drug treatment patterns, with antihypertensives being the most frequently prescribed drugs, followed by antihyperlipidemics, antiplatelets, and anticoagulants, aligning with other research studies.18–21 Furthermore, the frequency of surgeries and follow-up appointments among young patients with MI was statistically comparable between females and males.
Salient Points and Limitations of the Study
This cardiovascular study focused on young adults with MI in India, a group often overlooked in research, and explored gender differences in the prevalence of risk factors (e.g., diabetes, hypertension, and smoking) and clinical outcomes. The findings offer valuable insights for public health strategies aimed at reducing the MI burden, emphasizing urban-rural disparities in healthcare access and lifestyle factors across regions. Importantly, no gender differences were found in treatment regimens (e.g., antihypertensives and antiplatelets), suggesting clinical equality in care. However, as a single-center, retrospective study with a limited sample size, further research is needed to improve statistical power and generalizability. The absence of causal relationships and long-term follow-up data are additional study limitations.
Conclusion
The findings indicate that the prevalence of ST-elevation MI in young males was higher than in young females, with no significant differences observed between urban and rural populations. This pattern suggests a multifactorial aspect of MI in the Indian population. An association was observed between modifiable risk factors: hypertension and diabetes were more common in females, while smoking was more prevalent in males. Clinical features, diagnosis, treatment patterns, and outcomes were similar between both genders, highlighting the need for further research in larger populations to better address modifiable risk factors and mitigate MI prevalence among young people in India.
Footnotes
Acknowledgment
The authors sincerely thank Himanshu Meghnathi and Pruthvirajsingh Puwar for providing hospital data from Tulip Heart Centre, Anand, Gujarat.
Authors’ Contributions
Varsha J. Galani conceived of the study.
All authors developed the research protocol and performed the data analysis.
All authors contributed to the development of the manuscript content.
All authors read and approved the final manuscript.
Data Sharing and Data Availability Statement
Quantitative descriptive analysis of the data is available for sharing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethics Approval
The study was conducted after the approval from the ethics committee of CHARUSAT University with approval no. IEC/CHARUSAT/23/149.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
As the present study was a record-based retrospective study, there was no direct involvement of patients. So, informed consent was not taken.