
Abstract
Background
The increasing burden of hypertension in Asia poses significant challenges to healthcare systems, necessitating innovative strategies for its effective management. Telemedicine is increasingly recognized as a practical strategy to enhance accessibility, treatment adherence, and clinical outcomes for individuals with hypertension. This review synthesizes evidence on the effectiveness of telemedicine compared with conventional face-to-face care for hypertension management among adults in Asia.
Methods
A systematic review and meta-analysis were conducted in accordance with PRISMA-P and Cochrane methodological standards and were prospectively registered in PROSPERO. Eligible studies were randomized controlled trials involving Asian adults with hypertension that compared telemedicine-based care with routine in-person management. Trials reporting changes in systolic and diastolic blood pressure were included. Literature searches were conducted in PubMed and EMBASE, and bibliographies were screened for studies published between 2013 and 2023. Two reviewers independently performed study selection, data extraction, and risk-of-bias assessment using the RoB-2 tool. Statistical analysis was conducted using RevMan 5.4, employing a random-effects model when heterogeneity (I2 > 50%) was detected.
Results
Of the 397 identified records, 5 randomized controlled trials met the eligibility criteria. The telemedicine interventions used across these studies included remote blood pressure monitoring, mobile health applications, and virtual consultations. When compared with standard care, telemedicine produced a statistically significant but clinically modest reduction in systolic blood pressure (mean difference: –1.55 mmHg; 95% confidence interval: –2.67 to –0.43; P = .007). There was no meaningful change in diastolic blood pressure (mean difference: 0.32 mmHg; 95% confidence interval: –1.59 to 2.22; P = .74). Several trials also reported secondary outcomes, including medication adherence, lifestyle modifications, and metabolic measures.
Conclusion
Telemedicine yielded a modest improvement in systolic blood pressure but did not demonstrate superiority over clinic-based care for diastolic blood pressure control. While it offers a valuable platform for improving access and continuity, evidence suggests its clinical advantage remains limited. Larger, rigorously designed studies are required to better understand long-term outcomes and feasibility in resource-constrained settings.
Introduction
Hypertension remains one of the most significant contributors to cardiovascular morbidity and mortality worldwide. Asian countries face rising hypertension prevalence due to demographic, cultural, and lifestyle transitions.1, 2 The increasing burden of hypertension in Asia poses considerable challenges to healthcare systems, necessitating effective preventive and management strategies to reduce its impact on heart health.
Numerous extensive studies and epidemiological surveys have offered valuable insights into hypertension prevalence in Asian nations. For example, the InterASIA study found hypertension prevalence ranging from 26.0% to 41.8% across different Asian regions. 3 Recent data on Asian hypertension trends (HOPE report) reveal higher rates of undiagnosed hypertension in low- and middle-income countries in East and South Asia compared to wealthier countries (46%-55% vs. 29%-34%). 4 Effective hypertension management is critical to mitigate associated risks and enhance patient outcomes. However, achieving optimal blood pressure control and long-term treatment adherence is challenging due to limited access to healthcare, geographical barriers, and time constraints. Addressing this mounting health concern is imperative, necessitating tailored hypertension prevention and control strategies in the Asian context.
In recent times, telemedicine has emerged as a promising solution to overcome barriers in hypertension care and enhance patient outcomes. Telemedicine, encompassing virtual consultations, remote monitoring, and patient education, offers a transformative approach to hypertension management, fostering patient engagement and supporting healthcare professionals. 5 While individual studies have explored telemedicine’s potential benefits in hypertension management, a comprehensive assessment of existing evidence through meta-analysis is needed for more robust and generalizable conclusions. 6 This method allows for an objective and quantitative synthesis of data from multiple studies, enhancing the statistical power and precision of findings. Such an approach enables a thorough evaluation of telemedicine’s clinical effectiveness in hypertension management, considering diverse outcomes, study designs, and patient groups. This meta-analysis systematically examines the clinical effectiveness of telemedicine in hypertension management across Asian populations, comparing outcomes to those achieved through conventional clinic-based care.
Materials and Methods
Methodology and Registration
The meta-analysis followed the methodologies outlined by the Cochrane Collaboration and adhered to the guidelines presented by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P). 7 Furthermore, this review was registered in the International Prospective Register of Systematic Reviews.
Inclusion Criteria
All included original studies were sourced from randomized controlled trials that featured a control group and were conducted among adult patients diagnosed with hypertension in an Asian country. Included studies directly compared telemedicine interventions with usual in-person care and reported changes in systolic and diastolic blood pressure (SBP and DBP) from baseline to the end of follow-up for both groups. We excluded case reports, case series, narrative and systematic reviews, letters, and non-English articles that did not present measurable outcomes relevant to the analysis.
Sources of Data and Search Procedure
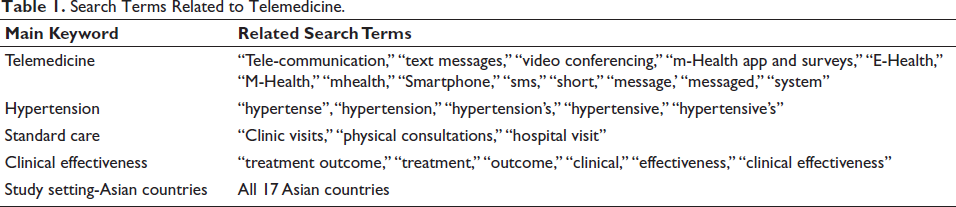
Published studies meeting the eligibility criteria were identified through searches in the PubMed and EMBASE databases. Additionally, reference lists of relevant articles and reports were reviewed to capture any missed publications. The search covered studies published between January 2013 and June 2023. The keywords used in the search strategy are summarized in Table 1.
Search Terms Related to Telemedicine.
Data Extraction Process
Data were extracted from all studies that met the inclusion criteria. Two reviewers independently screened and selected studies, with disagreements resolved by a third reviewer. Extracted information included study identifiers (first author, title, year of publication), study setting and design, duration, participant demographics (age and sex distribution), the type of telemedicine intervention, and mean SBP and DBP values (in mmHg) for both the intervention and usual care groups.
Evaluation of Bias Risk
The methodological quality of the chosen studies was assessed by two separate investigators using the “Risk of Bias for Randomized Studies of Intervention (RoB-2)” tool. 8 RoB-2 is primarily designed for systematic reviews and gauges the strength of evidence concerning the potential impact of an intervention on an outcome. RoB-2 explicitly outlines the estimated causal effect for each study concerning the outcome under examination. Risk-of-bias ratings (“low,” “high,” or “unclear”) were assigned by two independent reviewers who examined study features such as how randomization was conducted, the adequacy of allocation concealment, the extent of blinding for participants and assessors, completeness of outcome reporting, avoidance of selective reporting, and whether intention-to-treat procedures were implemented.
Statistical Evaluation
RevMan 5.4 and Rayyan QCRI were utilized to perform the statistical analyses, focusing on the differences in SBP and DBP from baseline to the end of follow-up for both the telemedicine and the standard clinic-visit groups. For studies that did not report change-score means or standard deviations, these values were derived using baseline and post-intervention summary statistics following Cochrane-recommended procedures. 9 All pooled estimates were presented with 95% confidence intervals. Between-study variability was examined using the Cochran Q test and the chi-square statistic. At the same time, heterogeneity was quantified using the I2 statistic, which reflects the proportion of variation not explained by random error. When heterogeneity exceeded 50%, indicating considerable variability across studies, a random-effects model based on the DerSimonian–Laird approach was applied. 10 Forest plots were constructed to display mean differences (MDs) and their associated confidence intervals. Statistical significance was interpreted at the P < .05 threshold.
Assessment of publication bias was not undertaken due to the small number of included trials. As recommended in methodological guidelines, funnel plot-based evaluations are considered unreliable when fewer than 10 studies are available, as the tests lack adequate power to detect true asymmetry. 11
Results
Study Selection
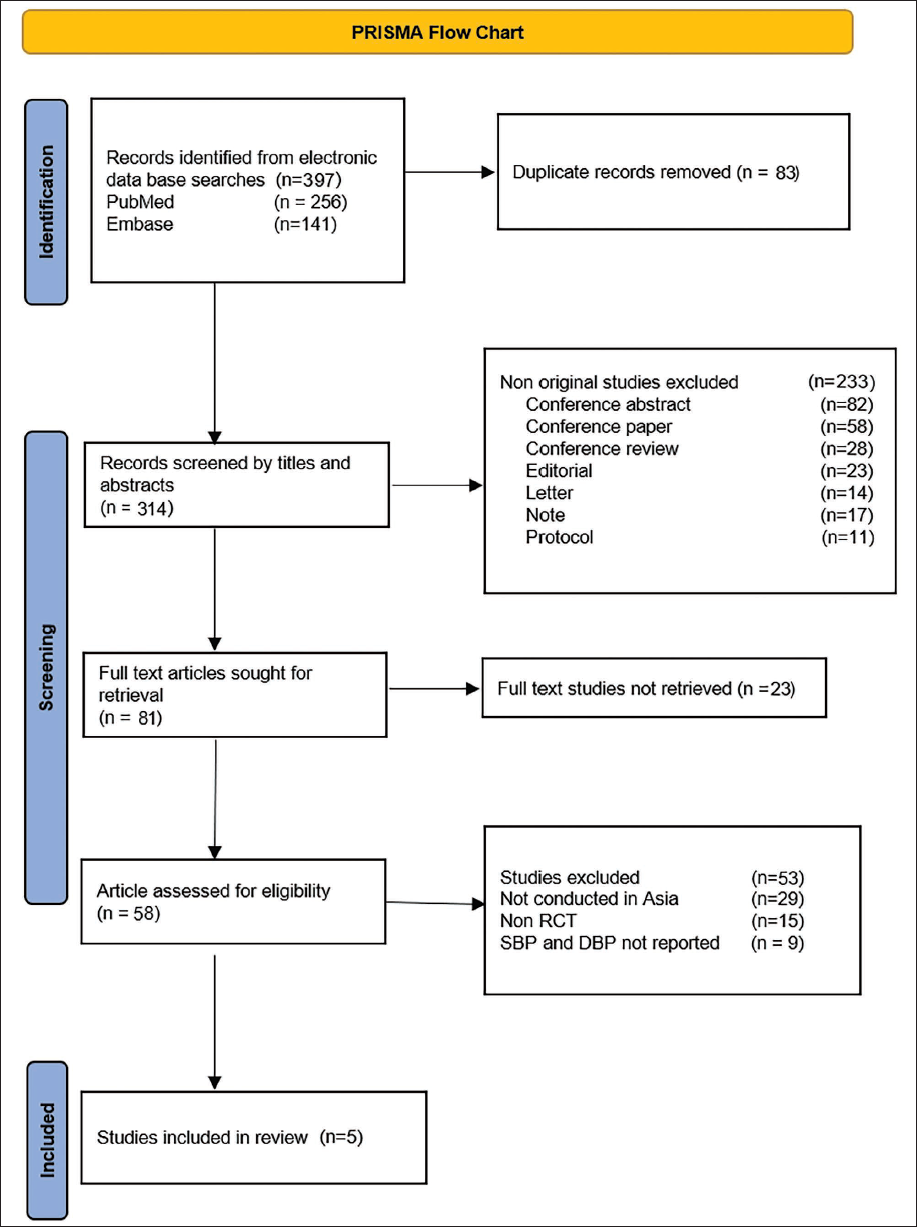
The electronic search of PubMed and Embase databases identified 397 records. The selection protocol is presented as per the PRISMA flowchart (Figure 1).
PRISMA Flow Diagram for Selection of Studies.
Characteristics of the Included Studies
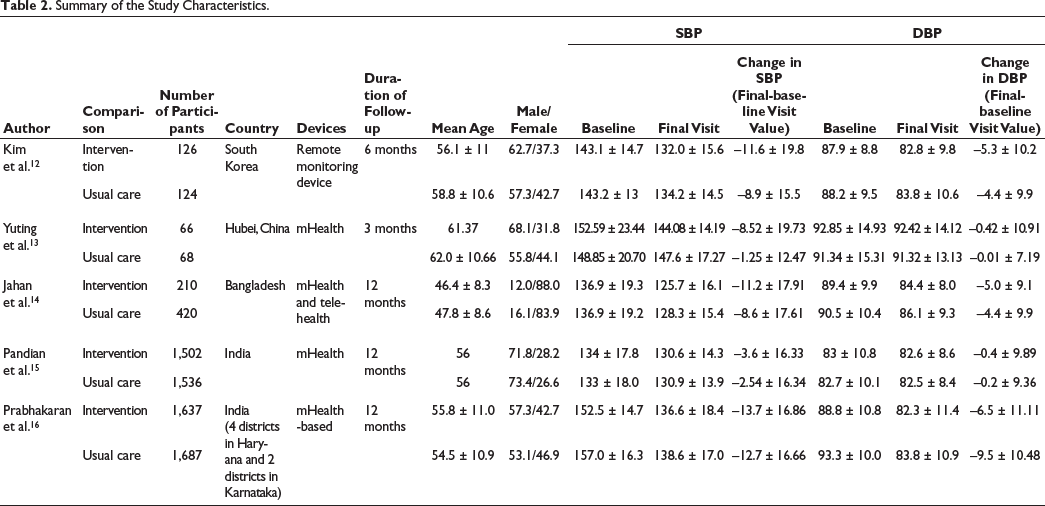
A total of five studies12–16 met the inclusion criteria, together involving 3,541 participants assigned to telemedicine-based care and 3,835 individuals receiving standard face-to-face management. Intervention durations varied widely, ranging from 3 months to 1 year. The digital approaches used across these trials included home blood pressure monitoring, mobile health applications, and various telehealth communication methods, as summarized in Table 2. Overall, the included studies showed a low risk of bias in completeness of outcome data, accuracy of outcome assessment, and consistency in reporting results (Table 3). Some methodological concerns were noted in domains related to randomization and allocation procedures, primarily because blinding participants was not feasible given the nature of the intervention.
Summary of the Study Characteristics.
Risk of Bias Scoring for Included Studies.

Results of the Meta-analysis
Effect on Systolic Blood Pressure
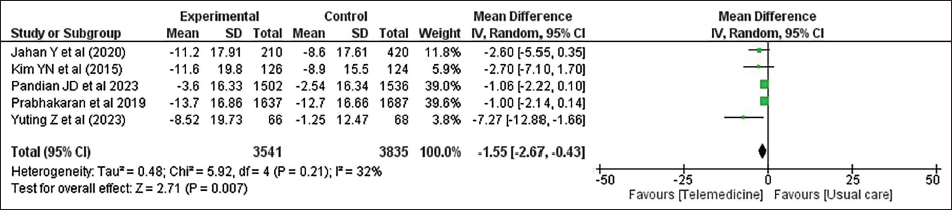
Given the substantial variability among the included studies, a random-effects model was applied to estimate the difference in SBP changes between participants receiving telemedicine support and those receiving routine in-person care (I2 = 88%). Pooling the results showed that the telehealth groups experienced a statistically significant reduction in SBP from baseline to follow-up compared with the usual-care groups, yielding a MD of –1.55 mmHg (95% CI: –2.67 to –0.43; P = .007). These findings are illustrated in Figure 2.
Forest Plot Showing Change in Systolic Blood Pressure Between Telemedicine and Clinic-visit Group.
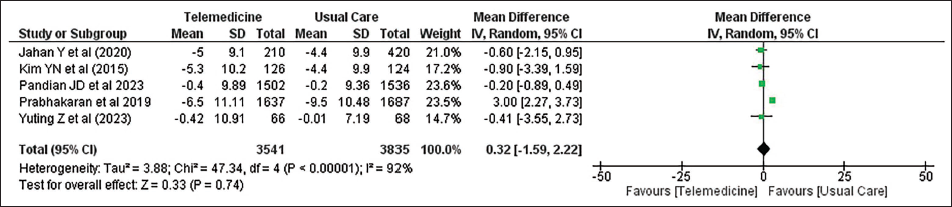
Effect on Diastolic Blood Pressure
For DBP, the included studies showed considerable variability, reflected by an I2 value of 92%. Owing to this marked heterogeneity, the analysis of differences in DBP between the telemedicine and standard care groups was conducted using a random-effects model. The decrease in DBP at follow-up was greater in the telemedicine intervention group (telehealth) than in the clinic-visit group in four studies.12–15 Prabhakaran et al. 16 reported the most significant decrease in DBP of 6.5 ± 11.11 mmHg, which was lower than the 9.5 ± 10.48 mmHg decrease in the clinic-visit group. The pooled analysis indicated that telemedicine did not produce any meaningful change in DBP when compared with conventional care. The overall effect estimate was 0.32 mmHg (95% CI: –1.59 to 2.22), with a nonsignificant P value of .74. These findings are illustrated in Figure 3.
Forest Plot Showing Change in Diastolic Blood Pressure Between Telemedicine and Clinic-visit Group.
Secondary Outcomes
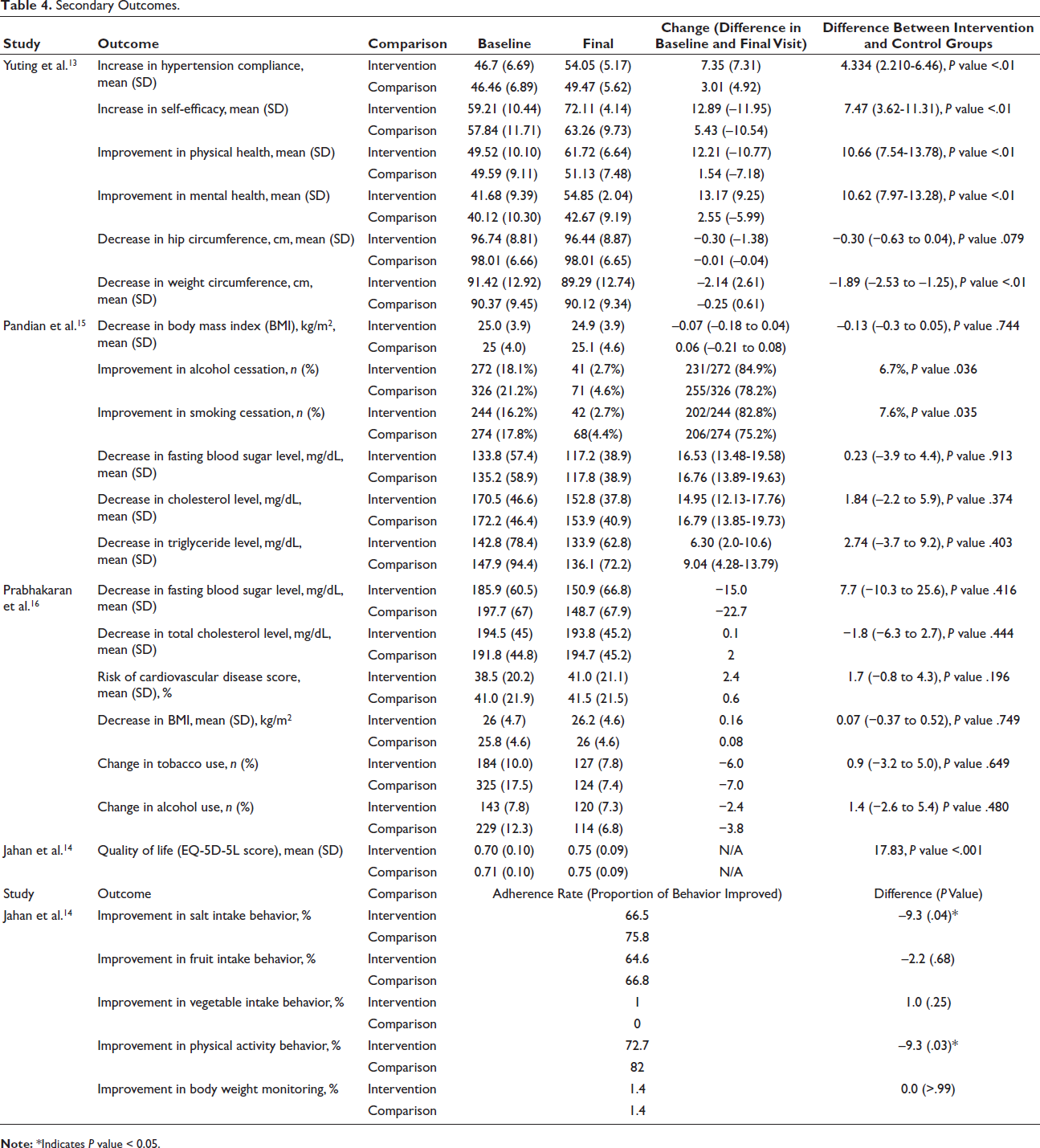
Four of the included trials also reported a range of secondary outcomes, including treatment adherence, patient confidence in managing hypertension, overall well-being, metabolic indicators, and various lifestyle behaviors as shown in Table 4. Yuting et al. observed notable gains in self-efficacy, adherence to hypertension management, and quality of life among participants receiving the digital intervention, along with a more pronounced reduction in waist circumference. 13 In contrast, Pandian et al. found that their semi-interactive stroke prevention program significantly enhanced smoking and alcohol cessation over 12 months. 15 Prabhakaran et al., who assessed an mHealth-supported decision system, detected no meaningful differences between the intervention and control groups for measures such as fasting glucose, cholesterol, or behavioral modifications. 16 Meanwhile, Jahan et al. reported that participants in the standard clinic-visit group showed slightly better adherence to salt restriction and physical activity. However, both study arms experienced improvements in quality of life, with the telemedicine group demonstrating a somewhat larger gain. 14
Secondary Outcomes.
Discussion
This meta-analysis, which pooled data from a large sample, sought to determine how telehealth-based approaches influenced SBP and DBP compared with traditional in-person care. In this meta-analysis, we included studies focusing on Asian countries, among which two were from India, one each from China, South Korea, and Bangladesh, and all were conducted among adults aged 40 years and above. Out of five studies, four used mHealth as a telemedicine intervention. The duration of these interventions ranged from 3 to 12 months. The results showed a statistically significant but not clinically significant decline in SBP and no difference in DBP in the telehealth intervention group. Evidence on improvement in secondary outcomes related to quality of life and treatment compliance remained inconclusive. Several earlier investigations have compared telemedicine-based hypertension care with conventional in-person management, with many demonstrating notable reductions in SBP in favor of remote interventions. The findings of our review align with these trends, showing a similar pattern; however, the pooled systolic reduction of –1.55 mmHg observed in our analysis is unlikely to have a meaningful clinical impact.17–20 Ma et al., in a broader meta-analysis assessing telemedicine use in chronic disease care, also reported a statistically significant drop in systolic pressure among patients using telehealth platforms. In contrast, diastolic measurements did not differ between intervention and control groups. 21 This finding was consistent with our study. Multiple studies attribute this decrease in blood pressure to the continuous monitoring and timely feedback of telemedicine. Additionally, studies have shown that telemedicine enhances treatment adherence through reminders and increases accessibility for patients residing in remote or rural areas. Patients are empowered to actively participate in their hypertension management by increasing engagement through educational resources and tracking tools, thereby contributing to effective blood pressure control.22–24
Notably, Yap et al. found meaningful reductions in both SBP and DBP in all three intervention categories—mHealth, telehealth, and their combined use—in their comprehensive review of digital health strategies for hypertension management. 25 Their conclusions were based on a much larger evidence base, incorporating 74 studies with over 92,000 participants from diverse global settings. In a similar vein, another meta-analysis focusing on randomized trials conducted in the USA reported that telemedicine-supported hypertension care (TM-HTN) achieved greater improvements in blood pressure control than standard clinic-based management. 26 The nonsignificant decline in DBP as reported in our article could be attributed to several limitations that hinder the widespread adoption and effectiveness of telemedicine. Limited access to necessary technology, such as smartphones and reliable internet connections, particularly in rural and underserved areas, poses a significant challenge. This digital divide restricts the reach of telemedicine services to populations that may benefit the most. Varying levels of trust and acceptance of telemedicine across different cultures can impact patient engagement. Socio-economic factors, including income and educational levels, can affect patients’ ability to engage with telemedicine services. 27
Overall, findings from the five included randomized controlled trials indicate that telemedicine-based care produced a statistically detectable, though clinically modest, decline in DBP, with a pooled MD of –1.55 mmHg (95% CI: –2.67 to –0.43). No corresponding improvement in diastolic pressure was observed. While the reduction in systolic values is slight, it represents a stable combined effect across diverse study environments rather than random fluctuation. Even subtle shifts in SBP at the population level can meaningfully influence cardiovascular risk; for example, lowering SBP by just 5 mmHg is associated with an approximate 10% reduction in cardiovascular events.28, 29 Although some variability across studies may stem from differences in measurement techniques or devices, the randomized designs would have minimized differential measurement error between the intervention and comparison arms. The analysis also highlighted improvements in medication adherence, health behaviors, and selected metabolic indicators. The results of this review offer essential guidance for expanding the use of telemedicine in blood pressure management throughout low- and middle-income regions of Asia. Strengthening its overall effectiveness will require a multifaceted strategy—one that prioritizes improved digital infrastructure, adapts interventions to local cultural contexts, and is supported by enabling policy frameworks. As telemedicine continues to evolve and takes a central role in healthcare delivery, this research stands to provide essential insights into the dynamic evolution of hypertension management, ultimately improving patient care and outcomes for this widespread chronic condition across diverse Asian populations.
Strengths and Limitations
The meta-analyses comprised five studies, in which the risk of bias was low for the domains of missing outcome data, measurement of the outcome, and selection of the reported result. The variability observed across the included studies may have affected both the accuracy and the broader applicability of the pooled estimates. Differences in methodological approaches, participant characteristics, intervention formats, and outcome measurements likely contributed to this divergence. Although a random-effects model was applied to accommodate these inconsistencies, many sources of variation could not be fully identified or adjusted for, which may limit the overall strength of the conclusions.
In addition, publication bias cannot be ruled out entirely. If present, it may have skewed the evidence base toward studies reporting more favorable effects of telemedicine, thereby inflating the apparent impact on blood pressure control.
Our reliance on summary data rather than individual patient data limited our capacity to conduct subgroup analyses or control for confounding variables at the individual patient level. The inclusion of studies using a wide range of telemedicine tools adds another layer of complexity, as the differing formats, technologies, and delivery mechanisms may influence both the direction and size of the observed effects on blood pressure. Variation in the length of the interventions also makes it difficult to distinguish between immediate benefits and sustained long-term impact. Additionally, because blinding is rarely feasible in telemedicine trials, the findings may be affected by performance or detection bias, potentially shaping how outcomes were reported or measured. Differences in what constituted “usual care” across studies may also have contributed to inconsistencies in the control group outcomes. Taken together, these factors highlight the need to interpret the results with caution and reinforce the importance of future research employing more uniform methodologies, standardized intervention protocols, and rigorous trial designs.
Footnotes
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the IEC Committee of ICMR-NCDIR (NCDIR/IEC/3067/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.