
Abstract
Objectives
Determine patient and provider perspectives on widespread rapid telemedicine implementation, understand the key components of a surgical telemedicine visit and identify factors that affect future telemedicine use.
Summary of background data
Compared to other specialties, the field of surgery heretofore has had limited adoption of telemedicine. During the COVID-19 pandemic Healthcare, including the surgical specialties, saw new widespread use of telemedicine.
Methods
We conducted a prospective cohort study during the COVID-19 California stay-at-home and physical distancing executive orders. Utilization data were collected from clinics and compared to usage data during the same time 1 year later. All patients and providers who participated in a telemedicine visit during the study period were asked to complete a survey after each encounter and the surveys were analyzed for trends in opinions on future use by stakeholders.
Results
Over the 10-week period, the median percentage of telemedicine visits per clinic was 33% (17%–51%) which peaked 3 weeks into implementation. One hundred and ninety-one patients (48% women) with a median age of 64 years (IQR 53–73) completed the patient survey. Patients were first-time participants in telemedicine in 41% (n = 79) of visits. Fifty-seven percent (n = 45) of first-time users preferred that future visits be in-person versus 31% of prior users (p = 0.007). The median travel time from home to the clinic was 40 min (IQR = 20–90). Patients with longer travel times were not more likely to use telemedicine in the future (61% with longer travel vs. 53% shorter, p = 0.11). From the 148 provider responses, 90% of the visits providers were able to create a definitive plan with the telemedicine visit. A physical exam was determined not to be needed in 45% of the visits. An attempt at any physical exam was not performed in 84% of routine follow-up or new-patient visits, compared to 53% of post-op visits (p = 0.001).
Conclusion
Telemedicine is a viable ambulatory visit option for surgical specialists and their patients. During rapid telemedicine deployment, travel distance did not correlate with increased use of telemedicine, and in-person visits are still preferred. However, nearly half of all visits did not need a physical exam, which favors telemedicine use.
Introduction
Telehealth is specifically defined as the practice of medicine using technology to deliver care at a distance, and telemedicine is the use of video-based platforms to deliver that care.1,2 Using telemedicine increases access to specialty providers, improves communication between patients and providers, provides health care education, and increases the cost-effectiveness of care. 3 Telemedicine in surgery began in the 1990s with the use of video to diagnose neonatal conditions but has been expanded into most surgical specialties. 4 Patients who use telemedicine report high satisfaction with the technology. 5 Despite the widespread availability of telemedicine, adoption in surgery specialties has remained low with only 10%–15% of surgeons using the tool. 6 This is potentially due to low reimbursement rates, the perception that a physical exam is required as part of all surgical evaluations, and limited familiarity with technology by surgeons and their patients.
In March 2020, the rapid worldwide spread of the SARS-CoV-2 virus, also known as COVID-19, resulted in the closure of businesses, physical distancing mandates, limited access to healthcare facilities, and the transition of many medical services to virtual with the expansion of Centers for Medicare and Medicaid Services waivers through the 2020 Coronavirus Aid, Relief, and Economic Security (CARES) Act. 7 The rapid implementation of telemedicine in surgery set up a natural experiment in which providers that may have been resistant to telemedicine use were compelled to use it to protect patients, providers, and other healthcare essential workers. This work aimed to evaluate the utilization of telemedicine during the pandemic's early months of California's executive stay-at-home and physical distancing orders, and the sustainability of telemedicine use in surgical clinics 1 year later. We also surveyed patients and providers to determine perceptions of and willingness to continue to use telemedicine in the future post-pandemic.
Methods
Study setting
The study was conducted as a prospective quality improvement project at a tertiary academic medical center within the Department of Surgery over a 10-week period. The Institutional Review Board approved the review of all quality improvement data collected.
Telehealth utilization data
Ambulatory surgery visits during the statewide COVID-19 California executive orders for stay-at-home and physical distancing (19 March to 29 May 2020) were evaluated. Surgical specialty clinics were Bariatric/Minimally Invasive Surgery (MIS), Cardiac, Colorectal, General, Plastics, Surgical Oncology, Thoracic, Transplant, Trauma, and Vascular. Each week a report was run for all department of surgery clinics. This report included the number of visits each provider performed classified as in-person, telephone, or telemedicine. Telemedicine visits were scheduled encounters that began as live synchronous video based. Visits were also classified by the type of care the patients received. New patient visits were visits to a provider the patient had never seen before. These included new consultations for surgical care. Pre-operative visits were those a patient had right before a scheduled surgery to discuss any last-minute details about the surgery, answer questions, or discuss new diagnostic findings. Post-operative visits were considered any visit for a patient who had surgery within the prior 90 days. Finally, follow-up visits were considered routine visits for patients who were seeing surgeons as part of long-term care. This is more common in cancer or vascular patients who have relationships that span years, and not all specialties see patients for follow-up visits.
Every week, the percentage of visits performed through each modality was determined by the provider. Baseline telemedicine utilization was determined by running a report of all telemedicine visits performed in the department of surgery for the same timeframe in 2019.
One year sustainability of telemedicine utilization was determined by reviewing the use of phone, video, and in-person visits during the same time frame (March–May) in 2021.
Patient cohort
All patients who were seen in a department of surgery clinic through telemedicine were included. After their telemedicine visit, each patient was contacted via automated text messaging and asked to complete a short electronic survey. Patients are automatically set up to receive text messages when they sign up for the online electronic medical record patient platform. They may request to opt out later. If patients did not respond to the initial request to participate, they were contacted again in 48 h and asked to participate. Patients who did not opt-out or who responded yes to participation were sent a link to complete the survey via text messaging. The survey queried patients on demographic information, video and audio connection experience, number of prior video visits by the patient, the distance they would normally travel to the clinic, and the likelihood to do subsequent video visits. The survey was created using an online electronic program (Qualtrics, Provo, UT).
Provider survey
All faculties, who treat adult patients, in the department or surgery were asked to complete a 1-min online survey immediately after each video visit. The survey queried faculty on the quality of the video and internet connection if the visit was able to be completed by video, if any type of physical exam was performed, and the ability to develop a plan as they would have in person. The 1-min survey was also created using Qualtrics (Provo, UT). A web link for the survey was emailed to the faculty. Weekly reminders with the survey link were sent out during the entire study period.
Statistical Analysis
Means and standard deviations were used to describe normally distributed continuous variables. For non-parametric data, median and interquartile range (IQR) were reported. Frequencies and percentages are used for categorical variables. Continuous variables were compared using the Wilcoxon rank sum test for non-parametric data or the Student's t-test for normally distributed data. Categorical values using χ2 tests with a p = value of 0.05 were considered statistically significant. All statistical analyses were completed in R Programming for Statistical Analysis (R Foundation for Statistical Computing) version 3.6.3.
Results
Telehealth utilization and sustainability
During the 2020 10-week pandemic stay-at-home and physical distancing period, a total of 2384 ambulatory visits were performed by 10 clinical specialty groups. Seven hundred and eighty-one (33%, range: 17%–51%) total encounters, with 482 patients, were performed via telemedicine. An additional 129 encounters (5%) were performed via audio-only telephone visits. Utilization peaked in weeks 2–4 (51%) and decreased to nadir levels (17%) in week 9 (Figure 1). Control data from the same 10-week time period in 2019 showed video visit utilization in the surgical clinics of 1% (0%–2%). Over the same time in 2021, 2740 total ambulatory encounters (video, phone, and in-person) were performed, which was an increase of 14% from during the pandemic stay-at-home and physical distancing period. Of these encounters, 366 visits (13%) were performed via telemedicine and 109 (4%) were performed by telephone visit.

Weekly utilization of telemedicine during the first 10 weeks of the COVID-19 pandemic and percentage of telemedicine video visits by year (2019 data not included due to the low values).
Telemedicine use varied among the 10 department of surgery specialty groups. The median percentage of telemedicine visits done in each clinic during the 2020 restrictions was 32% (6.6%–46.3%) (Figure 2). Bariatric/MIS and Thoracic Surgery had the highest percent utilization of telemedicine visits, with Transplant, and Surgical Oncology having the lowest utilization. There was a decrease in the percentage of telemedicine visits in 2021 down to 13% (p < 0.001). All clinics decreased their percentage utilization of video visits from 2020 to 2021, however, the high utilization groups (Bariatric/MIS and Thoracic) continued to have usage of over 20% of clinical visits (Figure 3).

A median number of video visits per week by the clinic during the pandemic lockdown in 2020. Provider video visits as a percentage of total visits.

Change in the utilization of video visits per clinical area by year. Median video visits as a percentage of total visits.
Patient perceptions
The patient survey was completed by 191 patients with a response rate of 45%.
The median patient age was 64 years old (IQR 53–73), and 48% of the respondents self-identified as female (Table 1). Ninety-seven percent (n = 187) of telemedicine visits were performed with the patients at their homes. Only three patients (2%) were at work when attending their telemedicine visit, and one patient was in a public location. Patients reported the visit started on time in 86% (n = 166) of cases. In the 14% of visits that did not start on time, the patient was late in 4%, and the physician was late in the other 10%. In 95% (n = 182) of telemedicine visits, the entire visit was able to be completed by video. Thirty-one (16%) patients needed help doing the visit. Of those, five had a physical limitation as their reason to need assistance, and the remaining 26 were uncomfortable with the technology or the app (13%).
Comparison of patients using telemedicine for the first time to those that had used it before. IQR = interquartile range.

In 41% (n = 79) of the visits, patients were using telemedicine for the first time (Table 1). The remaining 104 patients (55%) had experience with one to five prior telemedicine visits and 8 (4%) had more than five prior telemedicine visits. There were no racial or insurance differences between patients using telemedicine for the first time compared to those who had used it before. Of note, 46% of all users had Medicare. Fifty-seven percent (n = 45) of first-time telemedicine users would either prefer not to use telemedicine in the future (n = 9, 11%) or would use it only if required (n = 36, 46%). In contrast, patients who had used telemedicine prior were more likely to use it again in the future (69%, p = 0.001).
The most common visit type reported by patients was a routine follow-up visit (n = 86, 45%) (Table 2). New patient visits accounted for 28% (n = 54) of encounters while post-operative (21%, n = 41) and pre-operative visits (5%, n = 10) accounted for the remainder of encounters. Patients reported that in 73% of the visits (n = 139) a physical exam was not needed. There was a difference found in physical exams performed by type of visit (p = 0.002). Specifically, patients reported that in 83% of the new and routine follow-up visits, a physical exam was not conducted, but in 56% of post-operative visits, a virtual physical exam was performed. In 12% of encounters where a physical exam was attempted, patients reported the video quality was not adequate to execute the exam.
Patient-reported components of the telemedicine experience by type of visit.

The median travel time from home to the surgery clinic was 40 min (IQR = 20–90). There was no difference in travel times for patients who were participating in telemedicine for the first time, compared to those that had used it before (p = 0.59) (Table 1). Longer travel times also did not correlate with increased an likelihood to use telemedicine in the future (61% with longer travel vs. 53% shorter, p = 0.11).
Provider perceptions
The provider survey was completed for 148 telemedicine visits by 17 physicians, for a response rate of 20%. The survey was completed for more than 10 visits by four providers. Providers reported that 29% of the visits were new patient visits (n = 43), 28% were post-operative visits within 30 days of surgery (n = 28%), and 43% were longer-term follow-up visits. Providers reported poor video quality in 22 visits (15%) which caused the visit to be converted to audio telephone only. The visit started on time in 74% (110) of encounters. For the 26% of cases where the visit started late, this was more commonly because the provider was late (63%) rather than the patient being late (37%). Overall patients were the cause of 10% of visits starting late.
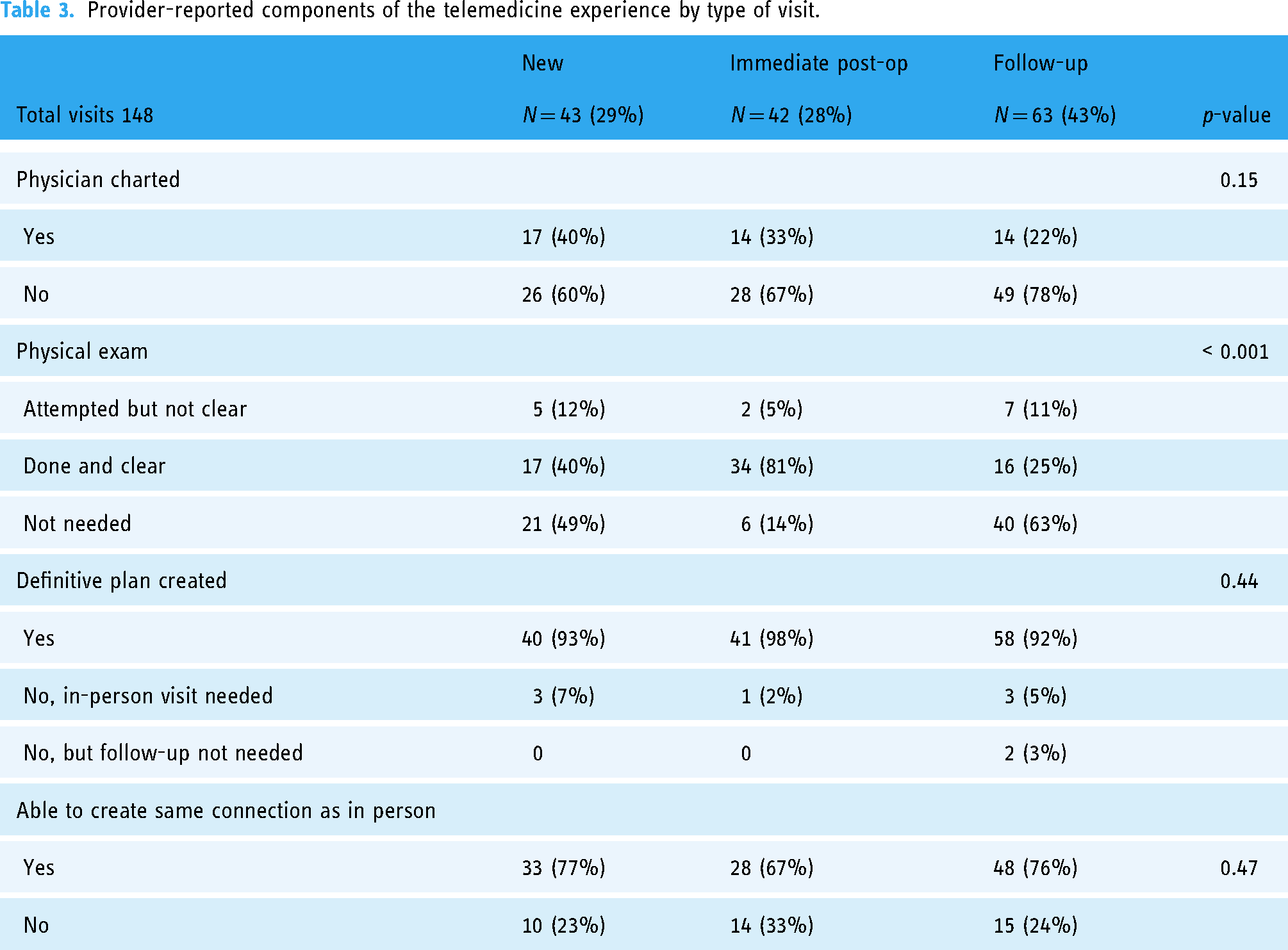
Respondents felt an in-person physical exam was needed in 45% (n = 67) of telemedicine visits, and this varied by visit type (Table 3). Providers concurrently charted in the electronic medical record while interacting with the patient in 30% of telemedicine visits (n = 45). Providers felt they were able to create a definitive plan in over 90% of visits, including 93% of new patient visits. Providers reported they were able to create the same interpersonal connection, as they would in an in-person visit, in 77% of new patient visits, 67% of post-operative visits, and 77% of follow-up visits.
Provider-reported components of the telemedicine experience by type of visit.
Discussion
Our work has shown that telehealth is feasible in all 10 specialty groups in a department of surgery, although certain provider groups gravitated to the resource more readily than others. We demonstrated that while providers were able to ramp up telemedicine utilization quickly during the stay-at-home order, use at one year decreased even further than at the end of the shutdown time. Patients easily pivoted to using telemedicine, but the majority still prefer in-person visits even if it would save them significant travel time to get to the clinic. Finally, we found that a physical exam was not needed in most surgical telemedicine visits, including new patient visits.
Within the stay-at-home and physical distancing period, surgery providers were able to increase the use of telemedicine to over 50% of weekly visits. One year later the degree of video visit utilization was between 10% and 20% of weekly visits. While many patients and providers were able to pivot to using telemedicine, there is still a strong preference for patients to come in to be seen. This is expected as many patients feel the need to see a provider face-to-face to gauge who they are and develop a relationship. 8 Providers also value the in-person visit, as they felt that in 23% of telemedicine visits, they were not able to make the same type of connection they would in the clinic setting. Within this study, providers in Bariatric/MIS and Thoracic Surgery exhibited the highest utilization during the pandemic and continue to use telemedicine regularly. When questioned about why their field is well suited for using telemedicine providers in Bariatric/MIS attributed the ability to use telemedicine to the high number of visits the patient goes through prior to making the decision for bariatric surgery. Both Bariatric/MIS and Thoracic providers also felt that much of surgical planning is done based on imaging and testing. Many of the patients who are seen by these specialty groups are part of the institution's tertiary referral network and have already obtained imaging tests. Because the imaging is done in advance, it can be reviewed and a plan developed at the time of the video visit. From their perspective, the video visit is mainly about seeing the patient, establishing a rapport, and determining if the patient is fit for surgery, which is feasible through video.
The mean age of patients who elected to use telemedicine during the rapid implementation was 64 years old, and 47% of patients had Medicare as their primary insurance. While most private insurance companies have covered the use of direct-to-consumer telemedicine, Medicare has been the most restrictive. Before the 2020 Coronavirus Aid, Relief, and Economic Security (CARES) Act, Medicare only allowed for direct-to-consumer telemedicine in the setting of home dialysis or opioid addiction treatment. The waivers for telemedicine put in place by the CARES Act opened the door for many to use the technology, and in our study, 58% of patients would use telemedicine again frequently. In the United States, 61% of patients over the age of 65 have a smartphone, and even more, patients have a tablet or computer device with internet capability. 9 Because 39% of the US population over the age of 65 does not have a smartphone, the ability to do video visits on alternative platforms besides just a smartphone is important. During our rapid implementation phase, the most common method used was through a smartphone, but 5% of patients required telephone audio-only visits because they did not have a suitable video-enabled device. Changing current telemedicine mandates for the Centers for Medicaid and Medicare Services (CMS) requires an act of Congress, and as the upcoming deadline for the CARES waivers approaches, bipartisan support is needed to make changes that will expand care for all patients through telemedicine, but not exacerbate disparities by not covering phone only care.
For many long-practicing physicians, the art of the physical exam, from their perspective, may be lost and is not being taught thoroughly in medical school. 10 In our study, patients reported a physical exam was not needed in 83% of new patient visits and 81% of long-term follow-up visits. Providers reported this number was markedly lower. Telemedicine use in surgery has been limited by concerns about how to do an adequate physical exam through video. 11 This dilemma has caused national organizations to develop a comprehensive visual physical assessment or a telemedicine physical exam. 12 Many specialty organizations have also developed guidelines for how to do an online physical exam. 13 Diagnostic imaging has become routine in an effort not to “miss anything” when primary care providers are seeing patients, and in many surgical fields, the entire surgery can be planned based on diagnostic imaging. Surgery specialties that are centered on imaging make them uniquely positioned to leverage telemedicine. For most surgeons a significant part of their visits with patients is presenting radiographic images and describing the surgery, this can still be done with video-based visits. For portions of the physical exam that are considered essential, surrogates can perform the exam, alternatively, the visit is done with the patient using wearable technology or in a remote clinic with coordinated care by a practitioner. All these scenarios give rise to new possibilities for providing convenient and equitable care.
We found that there was no significant difference in the willingness to use telemedicine in the future based on the time patients had to travel to get to the clinic. In our study, the median travel time was 40 min to get to the clinic. This is somewhat longer than other studies where travel time was 15–20 min, and it is possible that patients who are used to driving longer have come to accept this as part of their routine visits. It is also possible that a more in-depth analysis of travel distance vs time for different conditions or types of visits could better delineate which patients are willing to travel for what reasons. It is also possible that because the study site is a tertiary referral center, patients elect to travel specifically seeking higher-level care. While we only considered travel time, for patients, there are many other social determinants that factor into a clinical visit, such as time from work, cost of parking, gas, etc. All of these aspects have been shown to benefit from the use of telemedicine. 14 The benefit may be exponential since many patients with chronic illnesses have to rely on caregivers to coordinate travel dates and time. 8 Telemedicine also has the potential to significantly decrease the carbon footprint of many healthcare facilities. 15
This work has several limitations. First, patient survey results were not linked to their clinical visits. This would have allowed us to track visits over time and determine if there were changes in opinions about utilization. In addition, not all patients completed the survey, which does introduce bias. Second, providers participated in a selective fashion. All providers did not complete the survey, and it is possible the bias introduced by those that choose to participate could skew our conclusions. Finally, when pulling clinical utilization data, we did not collect the type of visit and cannot analyze how providers are using telemedicine for 1 year.
Conclusion
During rapid telemedicine deployment, providers drastically increased utilization, but this was not sustained at the same level one year later. Patients will use telemedicine, but many still prefer in-person visits, and distance to travel does not specifically correlate with increased use of telemedicine. Finally, the use of the visual telemedicine physical exam may go unrecognized by patients but is a useful tool for providers to understand and use.
Footnotes
Acknowledgements
We would like to acknowledge all surgeons at UC Davis who completed the survey.
Authors’ note
This work was presented at the American Surgical Congress, in February 2022, in Orlando Florida.
Contributorship
MDH researched literature and conceived the study. JM MDH, DTC, and AS were involved in protocol development, gaining ethical approval, and data collection. TH, JM, and PY collected data and sent out patient surveys. JM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MDH has received funding from the NHLBI and Society for Vascular Surgeons.
Ethical approval
The ethics committee of the University of California Davis approved this study (number 1626011-1).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute (grant no. K23HL134178).
Guarantor
MDH