
Abstract
Pulmonary endarterectomy is the only potentially curable treatment of choice for chronic thromboembolic pulmonary hypertension, while balloon pulmonary angioplasty has been advocated for peripheral (distal) chronic thromboembolic pulmonary hypertension. In an environment where experts for surgical interventions are not readily available, oral medications should be considered early, especially when the distal pulmonary vessels are affected. We present a 43-year-old male diagnosed with elephantiasis of the left leg at 20 years of age. He presented at the emergency room with a 6-month history of progressive dyspnea, easy fatigability, cough with hemoptysis, and World Health Organization functional class IV. Electrocardiogram findings were consistent with pulmonary embolism. He had transthoracic echocardiography and also chest computed tomography pulmonary angiography, which confirmed peripheral chronic thromboembolic pulmonary hypertension. He was commenced on oral medications with significant improvement in prognostic variables such as 6-minute walk test, World Health Organization functional class, and oxygen saturation even a year after commencement.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is not a frequently seen disease. It is characterized by obstruction of the distal and/or proximal pulmonary vasculature by remnant organized thrombi, leading to elevated pulmonary vascular resistance, progressive pulmonary hypertension (PH), and, in its late stage, right ventricular failure, which often leads to mortality.1–4 CTEPH is one of the cardinal causes of PH and has been categorized into group 4 by the WHO. 5 It is a disease with a high burden of morbidity and mortality.6, 7 The adverse outcome is worsened by its nonspecific symptoms and by being a strong mimic of cardiovascular disease, which often leads to a delay in diagnosis. It complicates about 0.6%-9% of cases of acute pulmonary embolism (PE).3, 7 Among the various causes of severe PH, CTEPH has an outstanding chance of being cured if treated early.3, 4 Pulmonary endarterectomy (PEA) is the treatment of choice in patients with operable CTEPH; it requires a high surgical skill coupled with meticulous preoperative care.3, 8 In case of peripheral or inoperable CTEPH, balloon pulmonary angioplasty (BPA) should be considered. 9 However, various successes have been recorded with the use of oral medications, as documented by case series and reports.3, 4, 8, 10 Among various medications used were prostanoids, endothelin receptor blockers, phosphodiesterase-5 enzyme inhibitors, soluble guanylate cyclase stimulators, and anticoagulants. 8 Thus, we report a 43-year-old who was diagnosed with CTEPH and had significant improvement with the use of oral medications.
Case Report
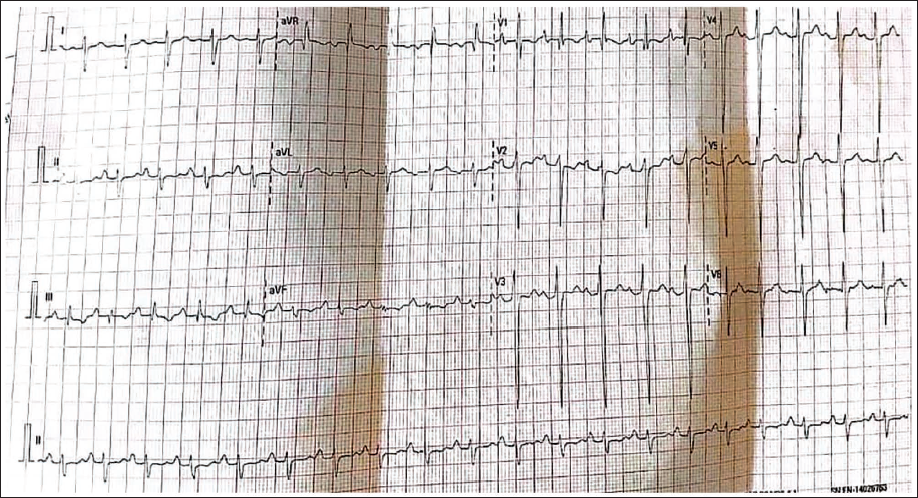
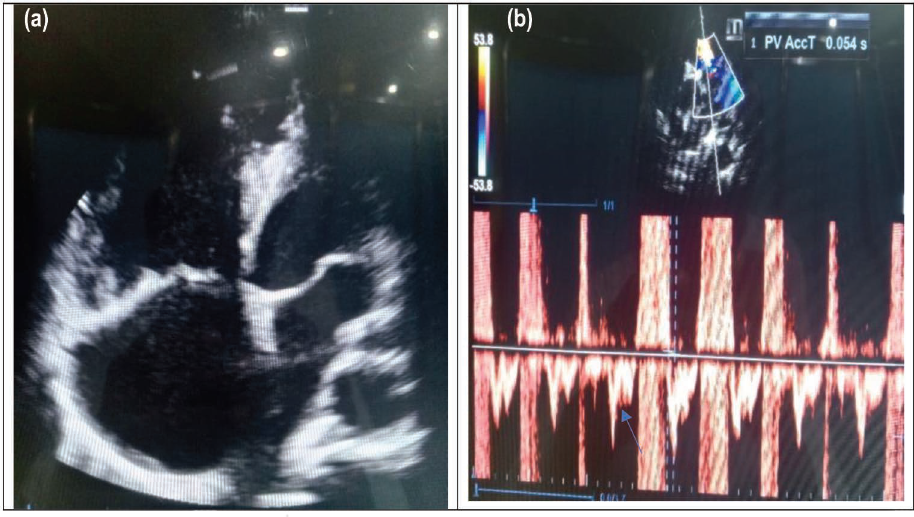
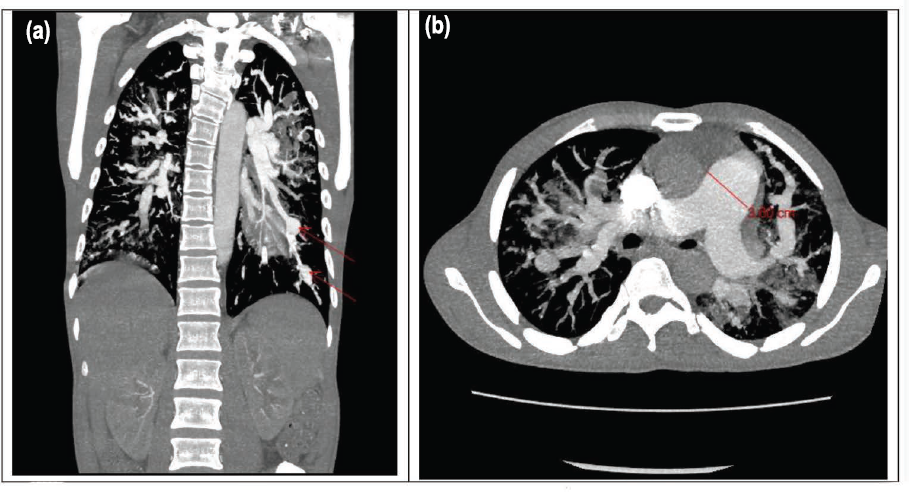
A 43-year-old male truck driver was diagnosed with left lower limb elephantiasis at 20 years of age. He was admitted via the emergency department with progressive dyspnea, easy fatigability, cough with hemoptysis of 6 months duration, and WHO functional class IV. Physical examination revealed blood pressure 130/80 mmHg, pulse rate 114 beats/min, respiratory rate 30 breaths/min, jugular venous distension, and bilateral pedal edema in the lower extremities, worse on the left. His oxygen saturation in ambient air was 80%. Complete blood count was not remarkable; white blood count (WBC): 5.6 × 10 9 /L (WBC differentials: neutrophil: 46%, lymphocyte: 44%, monocyte: 5.5%, eosinophil: 4.0%, basophil: 0.5%), hemoglobin (Hb): 11.3 g/dL, platelet: 223 × 10 9 /L, erythrocyte sedimentation rate (ESR): 34 mm/h, normal renal function (serum creatinine 54 µmol/L), and sputum GeneXpert for pulmonary tuberculosis was negative. Electrocardiogram showed deep S-wave in lead I, Q-wave and inverted T-wave in lead III, typical of PE (Figure 1). Chest X-ray revealed widespread reticulonodular opacities in both lung fields, worse on the right, multiple macronodules of varying size with marginal irregularities, and cardiomegaly. Transthoracic echocardiography (TTE) showed dilated right atrium, right ventricle, and pulmonary trunk. There was right ventricular systolic dysfunction (tricuspid annular plane systolic excursion [TAPSE]: 1.34 cm), severe pulmonary regurgitation, and evidence of PH; mean pulmonary arterial pressure (mPAP): 57 mmHg (Figure 2a and 2b). Doppler ultrasound of the leg confirmed deep vein thrombosis (DVT). Computed tomography (CT) pulmonary angiography showed small pulmonary emboli involving the right and left upper lobe segmental and subsegmental branches, as well as the lower lobe subsegmental pulmonary arteries, multiple aneurysmal dilatations of the segmental and subsegmental pulmonary arteries bilaterally, with dilated pulmonary trunk (Figure 3a and 3b).
Electrocardiogram (ECG) Recorded in the Patient. Deep S-wave in Lead I, Q-wave and Inverted T-wave in Lead III, Typical of Pulmonary Embolism.
(a) Four-apical Echocardiography (ECHO) View with a Dilated Right Atrium (RA) and Right Ventricle (RV). (b) Pulsed Wave Spectrum via the Pulmonary Valve with a Systolic Notch (Blue Arrow) and PV. AccT = 54 ms (Mean Pulmonary Arterial Pressure [mPAP]: 57 mmHg).
(a) Computed Tomography (CT) Pulmonary Angiography Showing Thrombus in the Distal Pulmonary Vessel; Filling Defect (Red Arrow). (b) Dilated Pulmonary Trunk; 3.00 cm (Red Line).
Chronic thromboembolic PH complicated with cor pulmonale was diagnosed. He continued on intranasal oxygen and was commenced on oral rivaroxaban, sildenafil, spironolactone, and furosemide, and discharged home with the same medications alongside domiciliary oxygen. He has had a year clinic follow-up with significant improvement in his condition as evidenced by WHO functional class I, 6-minute walk test (6MWT) increased from 120 to 370 m after a year, TAPSE improved to 1.84 cm, and his most recent mPAP was 20 mmHg as estimated by TTE. He is no longer using domiciliary oxygen, a wheelchair, or additional assistance and support. Further treatment options in future include BPA; however, the index patient has done well on oral medications, which should always be considered in an environment where experts for surgical intervention are not readily available, in addition to the huge cost of the procedure.
In addition to the above, he was referred to the plastic unit of the hospital in view of the lymphedema and has since been attending the clinic. He is using compression stockings alongside limb elevation as a form of conservative treatment. He was also counseled on hygiene to prevent cellulitis/lymphangitis. Future consideration includes debulking surgery; however, the patient is much ambulant at the moment, and the conservative treatment appears to be working well.
Discussion
Chronic thromboembolic pulmonary hypertension is defined as PH associated with an elevated mPAP (greater than 20 mmHg) caused by thromboemboli in the pulmonary arterial system. 2 It is not often seen, though it is more common than previously reported.2, 7 There is equal sex distribution, and most patients present in the sixth decade of life. 11 The index case presented at an earlier age due to the long years of elephantiasis, which is a risk factor for the development of recurrent DVT. 12 In the index case, the Doppler ultrasound showed evidence of DVT in the affected limb, thus giving further credence to the observation of Boo et al. 12 and Hadju et al. 13 who identified filarial lymphedema as a risk factor for the development of CTEPH. Other established risk factors for the development of CTEPH include permanent intravascular devices, autoimmune diseases, malignancy, inflammatory bowel disease, hypothyroidism, splenectomy, thrombophilia, and genetic predisposition.8, 14 There is a dearth of studies of CTEPH in Africa, which may be related to the non-readily available and affordable sophisticated equipment needed for the diagnosis. 10 In recent studies, CTEPH develops in 0.6%-9% of patients who have experienced an acute PE. 7 Unlike acute PE, which has an easily detachable thrombus that consists of a mesh of fibrin alongside red cells, the pathological finding in CTEPH appears yellow and consists of fibroblast, collagen, vessels, and inflammatory cells, which are closely adherent to the vascular wall. Recanalization of the obstructed vessels, especially in the large and medium arteries, leads to the formation of bands, webs, and stenosis, which are characteristic findings in CTEPH. 15 The major pathophysiology is the partial or complete occlusion of the pulmonary vascular bed by a nonresolving thromboemboli, leading to increased pulmonary vascular resistance, progressive PH, and, in its later stage, right ventricular failure, which often leads to mortality.3, 7 In addition, the development of webs, bands, and stenosis in the area previously affected with acute PE leads to redistribution of blood flow to the unaffected area, which amounts to increase in shear stress and pressure in the vessels. 15 The two pathophysiological changes described above have led to CTEPH often being referred to as a two-compartment disease comprising mechanical intraluminal obstructions and a sizable degree of arteriopathy in nonobstructed areas that is not different from pulmonary arterial hypertension (PAH).6, 7 The index case presented with typical symptoms and signs of right ventricular heart failure, which is the major complication and cause of mortality in patients with CTEPH. 7 Ventilation/perfusion (V/Q) scan is the investigation of choice for diagnosing CTEPH; however, recent study showed that V/Q scan and computed tomography pulmonary angiography (CTPA) are accurate methods of diagnosing CTEPH with excellent accuracy. 1 The location of the emboli, which could be proximal, distal, or both, has a significant implication in the mode of treatment. PEA is the only approved surgical treatment for operable CTEPH in which case the proximal part of the pulmonary vasculature is occluded; in patients with distal occlusion, it may not be amenable to surgical intervention, hence the use of various medications with proportions of success recorded.6, 8, 14, 16, 17 PEA is a complex procedure; only expert centers with large volume of patients with good outcomes have been advocated to carry out the procedure. Such dedicated centers are not available in our environment as we are informed. 10 In addition, the CTPA (Figure 3a and 3b) of the index case showed that the occlusions were mainly in the distal segment of the pulmonary vessel alongside a very high mPAP, hence the option of medical therapy.
Conclusion
Chronic thromboembolic PH is a disease with high morbidity and mortality. Early commencement of medical therapy in the peripheral form of CTEPH, where the required surgical skills are not readily available or are lacking, will improve patient outcomes.
Footnotes
Acknowledgment
The authors acknowledge Dr. T. A. Okedere (MBChB, FWACS) of the Department of Radiology, Royal Brompton & Harefield Hospitals, UK, who reviewed and interpreted the images.
Authors’ Contributions
Olaoye O. B.: Concept and design of the manuscript. Contributed to literature search, data acquisition, data analysis, intellectual input, manuscript editing, and final manuscript review. Babatunde E. O., Eminowa O., and Sanmi-Alao O. O.: Contributed to literature search, data acquisition, data analysis, and manuscript preparation. Awopeju O. and Ojo O. E.: Gave intellectual input, manuscript editing, and final manuscript review. All authors gave final approval of the version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has provided informed consent for the submission of the article to the journal.