
Abstract
A young adult in their 20s with recurrent presyncope, a diagnosed case of complete heart block, underwent a dual-chamber pacemaker implantation with left bundle branch area pacing (LBBAP). An immediate post-procedure electrocardiogram (ECG) showed atrial and ventricular paced complexes. However, an ECG two hours later showed no pacing pulses with an extremely prolonged PR interval of 400 ms. What is the probable mechanism?
Case Report
Case
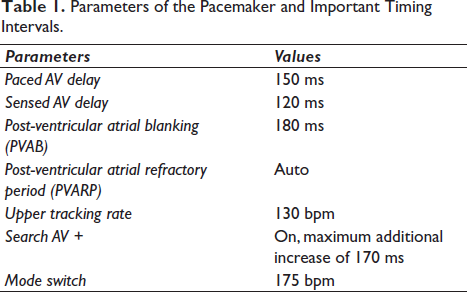
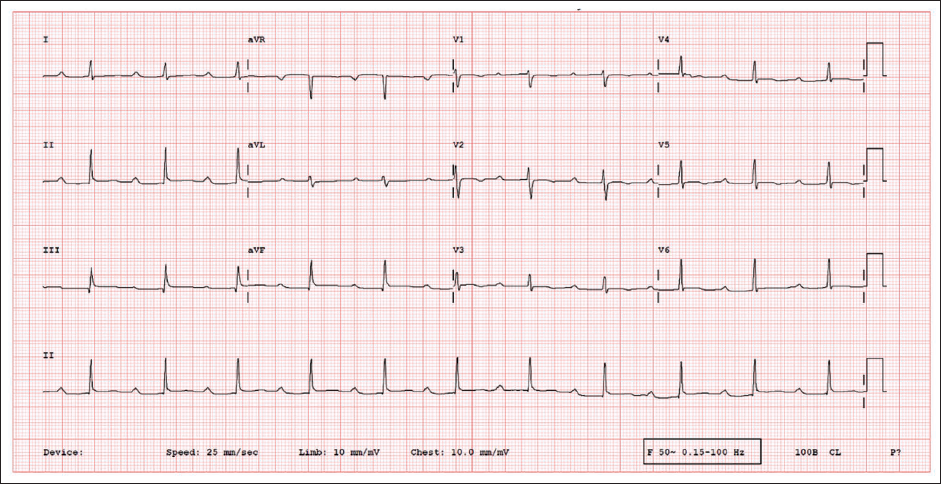
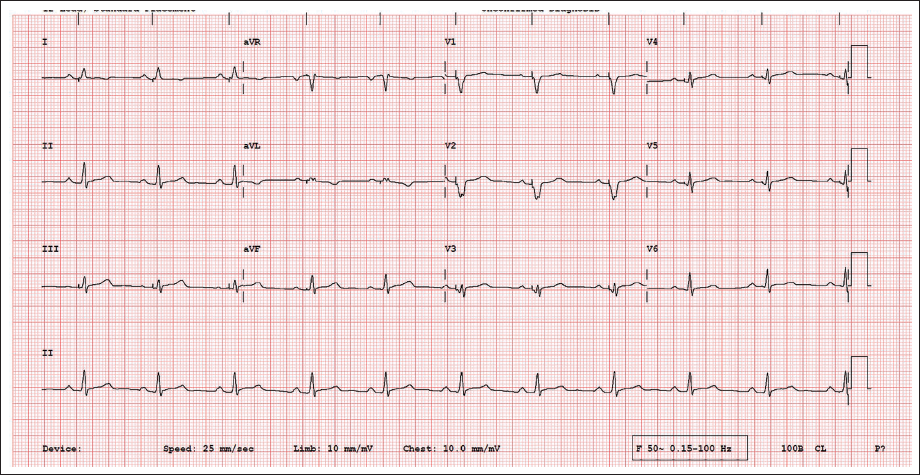
A young adult in their 20s with recurrent presyncope was diagnosed with an intermittent congenital complete heart block (CHB). She underwent dual-chamber pacemaker implantation with left bundle branch area pacing (LBBAP) (Medtronic DDDR) (Table 1, Supplementary Figures 1,2). An immediate post-procedure ECG showed atrial and ventricular paced complexes. However, an electrocardiogram (ECG) two hours later showed no pacing pulses with an extremely prolonged PR interval of 400ms (Figure 1). Magnet ECG showed ApVp rhythm at a paced atrioventricular (AV) delay of 150 ms. What is the probable mechanism?
Parameters of the Pacemaker and Important Timing Intervals.
12-lead Electrocardiogram of the Index Patient.
Discussion
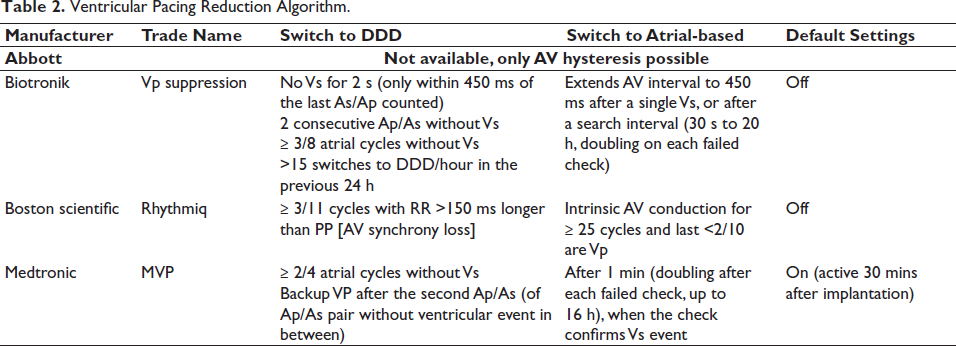
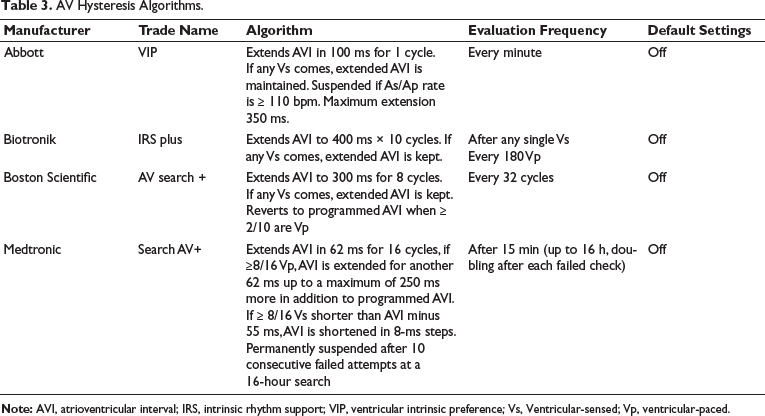
Lead malfunction and pacemaker device failure were ruled out as magnet ECG showed normal atrial and ventricular pacing. The sensed and paced AV delay was 120 ms and 150 ms, respectively, and did not explain the extreme AV delay. The search AV+ was ruled out as the highest PR interval (maximum sensed AV delay) possible with the programmed parameters was 290 ms (120 + 170 ms). In AV hysteresis mode, if eight or more Vs events in the previous 16 ventricular events are within 15 ms of the scheduled Vp event (or if ≥8/16 Vp), the sensed and paced AV delay is extended by 62 ms to promote intrinsic rhythm up to a maximum value of 600 ms (Tables 2 and 3).
Ventricular Pacing Reduction Algorithm.
AV Hysteresis Algorithms.
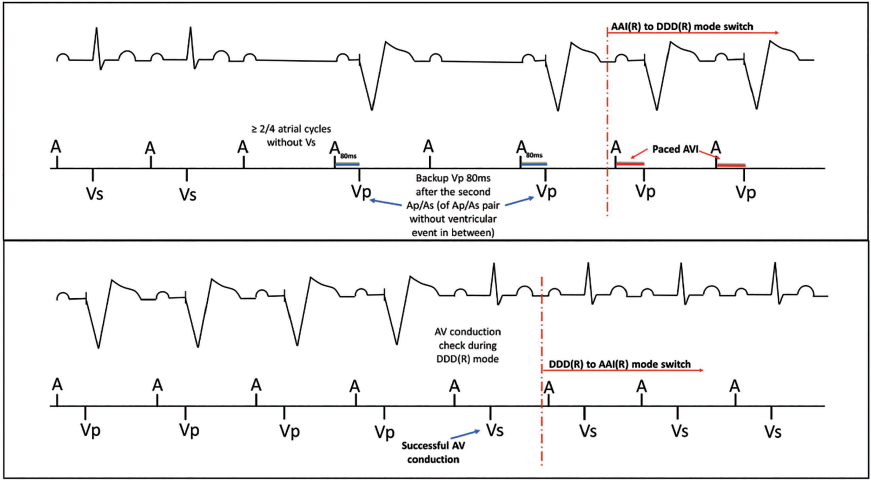
Managed ventricular pacing (MVP) mode is an algorithm to operate the pacemaker in AAI mode while having ventricular pacing as a backup with an immediate switch to DDDR mode once the AV conduction is absent (Table 1, Figure 2).1, 2 In MVP mode, the first check for AV conduction occurs after one minute. Subsequent checks occur at progressively longer intervals (2, 4, 8 … min) up to 16 hours and occur every 16 hours after that and the pacing mode is changed to AAI(R) from DDD(R) if AV conduction is detected (or vice versa when AV conduction is not detected). This mode is marked as AAI< = > DDD [AAIR < = > DDDR] in the device programmer, and when it is functioning in AAI(R) mode with backup ventricular pacing, an AAIR+ sign is mentioned in the top left corner of the programmer (Supplementary Figures 3, 4). 3 A look back at our case revealed a transition from DDD(R) mode [AsVp] mode to AAI(R) with a prolonged PR interval (Figure 3). This was probably due to intermittent congenital CHB with occasional presence of AV nodal conduction. In AAI(R) mode, when two out of four recent A-A intervals contain no intrinsic QRS, the pacemaker switches back to DDD(R) mode (Figure 4). If the conduction check fails and no intrinsic QRS is detected, backup ventricular pacing is given at 80 ms after the atrial sensed or paced events. In our patient, the likely mechanism for the extreme AV delay is that the conduction check detected intrinsic QRS complexes leading to a mode switch to AAI(R).
Upper Panel. Mode Switch from AAI(R) to Temporary DDD(R). Two Out of Four Most Recent A-A Intervals with No Conducted Vs Event (Pacemaker Supplies a Ventricular Backup Pulse at 80 ms); Lower Panel. The Pacemaker Performs an AV Conduction Check, If Successful, It Changes from DDD(R) to AAI(R) Mode. If Unsuccessful, It Remains in DDD(R) Mode (Pacemaker Supplies a Ventricular Backup Pulse at 80 ms).
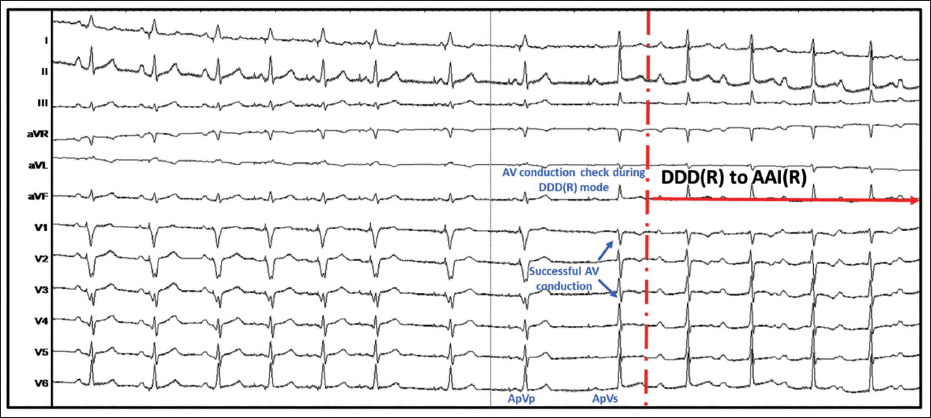
An Electrocardiogram During the Procedure Shows That the Pacemaker Performs an AV Conduction Check, and It Changes from DDD(R) to AAI(R) Mode.
Pacemaker in DDD(R) Mode with AsVp Rhythm When No Intrinsic Atrioventricular Conduction Exists.
The second iteration of MVP™ (MVP™ 2.0) incorporates a dynamic, adaptive A-A interval and a configurable maximum AV interval threshold, avoiding an erroneous detection of escape beat (in the presence of AV block) as AV conduction after a predefined AV interval. 2 This case highlights the importance of knowledge of advance pacemaker algorithms to avoid unnecessary investigations.
Footnotes
Authors’ Contribution
SSK, SM, JV, ASP, and NN were involved in conceptualization, formal analysis, writing—original draft, and review and editing.
Clinical Trial Registration
Not applicable.
Data Availability Statement
All data are incorporated into the article and its online supplementary material.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as it is an anonymous case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained.
Permission to Reproduce Material from Other Sources
Not applicable.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.