
Abstract
Complete heart block is an uncommon condition that can be fatal if unidentified, as it affects the conduction system of the heart. The phenomenon may be caused by a drug or underlying medical condition requiring a temporary or permanent pacemaker to stabilize the condition. We report a case of complete heart block precipitated by ticagrelor which was reversed with the cessation of ticagrelor therapy.
Introduction
Ticagrelor, an oral antiplatelet agent, is a potent and direct P2Y12 antagonist causing rapid onset of action and intense platelet inhibition. 1 It is recommended as a first-line antithrombotic agent in patients with acute coronary syndrome, also prevents postsurgery myocardial infarction and stroke. 2 As per the American College of Cardiology guidelines, dual antiplatelet therapy (ie, aspirin and P2Y12 antagonist) is the cornerstone of treatment for patients with acute coronary syndrome and following cardiac catheterization for stable coronary disease. 3
The drug is usually well tolerated, but some patients experience serious adverse effects such as major bleeding, gastrointestinal disturbances, dyspnea, and ventricular pauses > 3 seconds. 1 The commonly observed side effects are headache, backache, altered blood pressure, and bradycardia.
In our case report, we present a case of ticagrelor-induced high-degree atrioventricular (AV) block manifesting as syncope.
Case Report
81-year-old man with known medical history of hypertension, hypothyroidism, dyslipidemia, obstructive sleep apnea, chronic obstructive pulmonary disease, benign prostatic hyperplasia, and coronary artery disease underwent coronary angiography which showed double-vessel coronary artery disease. This was followed by percutaneous coronary intervention/drug-eluting stenting (PCI/DES) to left anterior descending artery and plain old balloon angioplasty to left circumflex artery-obtuse marginal branch 3. He was discharged on aspirin, ticagrelor, rosuvastatin, thyroxine, acebrophylline, and tamsulosin.
After continued medications for 5 days, later in the evening, he presented to emergency department of the hospital with complaints of loss of consciousness, uprolling of eyes, and urinary incontinence preceded with 1 episode of vomiting. A total of 4 episodes of syncope each lasting for 5 to 10 seconds of duration were reported with spontaneous recovery within seconds.
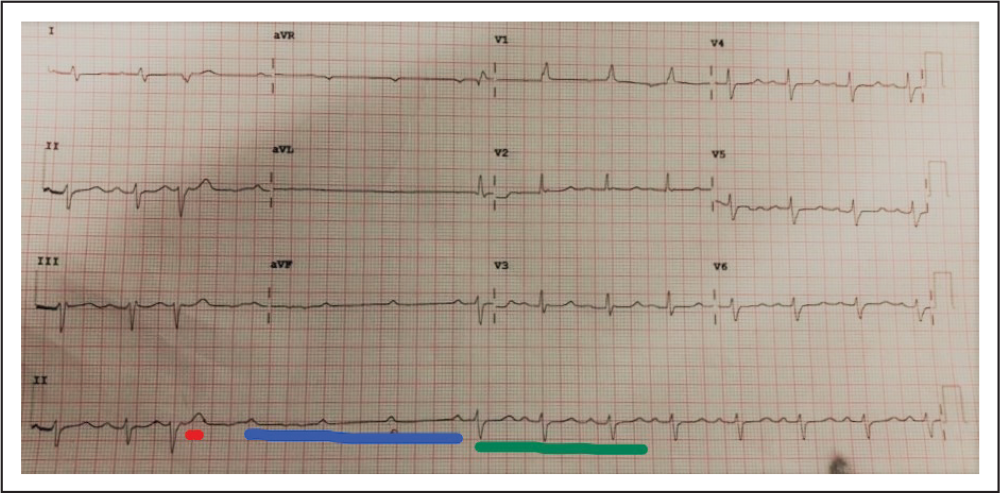
On evaluation, electrocardiography (ECG) showed right bundle branch block with intermittent episodes of high-grade AV block degenerating to complete heart block often precipitated by an ectopic beat and its associated pause. Two-dimensional echocardiography showed normal left ventricular function with regional wall motion abnormalities in right coronary artery territory and hypokinetic inferoposterior wall as before the PCI.
In the above electrocardiogram shown in Figure 1, ectopic beat (VPC) is marked by red color, AV discontinuation by blue color, and return to sinus rhythm is shown in green color.
Presentation ECG
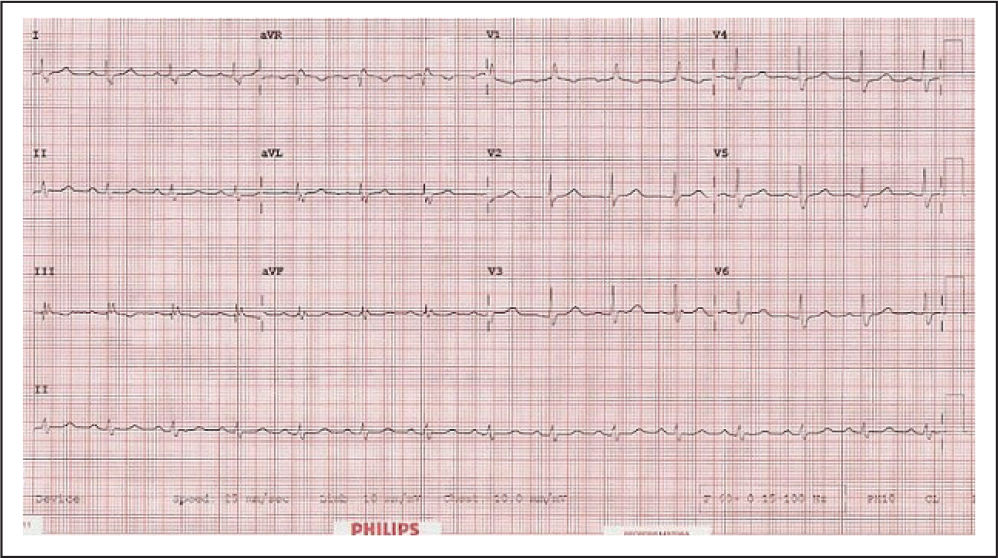
Electrocardiogram at 1-Year Follow-Up.
As the patient was recently prescribed ticagrelor (post PCI/drug-eluting stenting and plain old balloon angioplasty) and in view of case reports suggesting ticagrelor association with ventricular premature complexes and AV dissociation, ticagrelor was potentially thought to be the etiology for AV conduction block. Therefore, ticagrelor was stopped and switched over to clopidogrel.
Close monitoring and observation of the patient in the hospital for the subsequent 2 days showed no sign of AV block. On day 3, 24-hour Holter monitoring was done which showed minimum heart rate of 65 beats/min, maximum heart rate of 126 beats/min, and premature ventricular beats of 2.6% with no evidence of prolonged AV node conduction. The paroxysmal episodes of high-grade and third-degree AV block have been resolved and normal PR interval on ECG has been attained by cessation of ticagrelor therapy.
Thus, ticagrelor was replaced with clopidogrel in the drug regimen. Permanent pacemaker insertion was planned in case of recurrence of syncope episode during further follow-up visits. At 1-year follow-up, ECG showed sinus rhythm with right bundle branch block (same as pre-PCI procedure).
Discussion
Bradycardia related to ticagrelor was first described in a phase IIb dose-ranging study, where a post hoc analysis of cardiac arrhythmias revealed an unexpectedly increased incidence of predominantly asymptomatic ventricular pauses. 7 Case reports of clinically significant ticagrelor-related arrhythmias requiring temporary pacemaker or permanent pacemaker implantation and drug discontinuation have been published. Hence, to corroborate these findings prospective Platelet Inhibition and Patient Outcomes trial was performed. 8 According to this trial, ticagrelor is associated with ventricular pauses in the first week of treatment; however, these episodes were felt to be asymptomatic and nonfatal to the patient. 5
Paroxysmal AV block is a poorly defined clinical entity characterized by abrupt and unexpected changes from 1:1 atrioventricular conduction to complete heart block, leading to fatigue, dyspnea, dizziness, syncope, and potentially fatal sudden cardiac death. 4
The rhythm can be reversed, if the cause is correctly identified, diagnosed, and managed precisely. The first and most important step in the medical treatment for heart block is the withdrawal of any potential aggravating or causative medication. However, early identification of signs and symptoms of AV block, its diagnosis, and appropriate emergency escape mechanisms can prevent further occurrence of any cardiac complications and may help in reversibility of the situation.
Although paroxysmal AV block is a life-threatening condition because of unreliable escape mechanisms, its proper diagnosis is often missed and overlooked because of its unfamiliarity, unpredictability, and, in some cases, no clear evidence of AV conduction disease during normal 1:1 conduction. 4
Other P2Y12 platelet receptor antagonists, such as clopidogrel or prasugrel, are suitable alternatives if the patient is at risk for the development of a potentially life-threatening heart block. To prevent further recurrence of the event and support heart function, a permanent pacemaker insertion may be performed.
In the above case report, the patient did not require either a temporary or a permanent pacemaker. The AV block was resolved solitary termination of ticagrelor.
Conclusion
From the current case report, it can be inferred that ticagrelor can cause complete heart block—a rare, serious, and life threatening adverse event which could be reversed by early diagnosis and management. On termination of ticagrelor therapy, the patient showed significant improvement in symptoms. Insertion of neither temporary nor permanent pacemaker was required.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.