
Abstract
Background
The management of Chronic Coronary Syndrome (CCS) is often faced with the dilemma of the efficacy of Percutaneous Coronary Intervention (PCI) versus Optimal Medical Therapy (OMT). Despite advancements in medical treatments and stent technology, the relative benefits of these approaches remain under debate.
Methods
We carried out a single-blind randomized controlled trial comparing Major Adverse Cardiac Events (MACE) between OMT and PCI in 378 CCS patients in Indonesia. Patients were categorized based on their management approaches: revascularization (PCI + OMT) or no revascularization (OMT only). We excluded patients with history of CABG, stroke, heart failure, myocardial infarction, incomplete data, or those lost to follow-up, resulting in a final sample of 108 patients. The primary outcome was the incidence of MACE, including death, stroke, myocardial infarction, and hospitalization due to heart failure, during a 5-year follow-up period.
Results
The Hazard Ratio for death was 0.477 (95% CI: 0.262-0.869, P = .016). Similarly, the HR for myocardial infarction was 0.473 (95% CI: 0.209-1.073, P = .073), suggesting a trend towards lower risk with PCI. For stroke, the HR was 0.692 (95% CI: 0.245-1.949, P = .485), indicating no significant difference between PCI and OMT. In terms of hospitalization due to heart failure, the HR was 0.469 (95% CI: 0.196-1.121, P = .089), again showing a trend towards benefit with PCI, but not reaching statistical significance. These findings emphasize the possible benefits of PCI compared to OMT in lowering the risk of death and myocardial infarction in CCS patients.
Conclusion
MACE rates were higher in the OMT group compared to PCI in CCS patients. These results underscore the potential benefits of PCI Intervention over OMT in reducing adverse cardiac events.
Keywords
Introduction
Percutaneous coronary intervention (PCI) and optimal medical therapy (OMT) are two treatment modalities for patients with chronic coronary syndrome (CCS). 1 The management of CCS aims to alleviate symptoms, reduce adverse cardiovascular events, and improve overall quality of life.1, 2 Despite the widespread use of PCI in North America for CCS, a dilemma persists regarding its long-term prognostic impact compared to OMT.2–19 Early registry data indicate that most PCI procedures are performed electively in CCS patients, yet the benefit regarding the decrease in death rates and the likelihood of myocardial infarction remains unclear.3, 12, 20, 21 The COURAGE trial, a landmark study, was designed to investigate this uncertainty by evaluating whether PCI combined with OMT lowers the risk of death and nonfatal myocardial infarction compared to OMT alone.3, 22–26 Although PCI has been shown to reduce the frequency of angina and improve short-term exercise performance, its impact on long-term cardiovascular events remains unclear.3, 27
Similarly, the ISCHEMIA trial was designed to assess the impact of adding cardiac catheterization and revascularization, if possible, to pharmacological treatment in individuals with CCS and moderate or severe ischemia.21, 23, 28 This trial aimed to assess whether an invasive strategy, including PCI, improves outcomes in CCS patients compared to medical therapy alone.21, 23, 28 Additionally, the ORBITA trial evaluated the effect of PCI versus placebo on exercise time in patients with CCS symptoms.25, 29, 30 While previous research has shown an improvement in angina symptoms with PCI, the ORBITA trial aimed to provide stronger evidence using a placebo-controlled design.25, 29, 30. Conversely, for patients with acute coronary syndromes (ACS), PCI has been established as one of the mainstays of treatment, with strong evidence demonstrating its efficacy in reducing cardiovascular events.1, 3, 24, 30, 31 However, the optimal treatment strategy for non-acute CAD, clinically characterized by CCS, is less defined.3, 12, 20 Several guidelines emphasize risk factor modification and medical therapy as the main management approach for patients with stable angina.5, 12, 24, 32 Recent trials, including the COURAGE and BARI 2D trials, have not shown significant differences in outcomes between revascularization with PCI and OMT alone in patients with CCS.1, 2, 23, 31, 33 However, meta-analyses provide conflicting results, with some suggesting greater improvement in angina symptoms with PCI.12, 34
Furthermore, in the context of women with CCS, data from randomized controlled trials show conflicting results regarding outcomes with routine early invasive versus selective invasive strategies. 3 While early studies indicated worse outcomes in women with routine early invasive approaches, a collaborative meta-analysis later showed comparable benefits among both genders and high-risk women, but potential harm among low-risk women. 3 The COURAGE trial showed potential benefits of PCI plus OMT in women compared to men, but further evaluation is needed. 3 Based on Major Adverse Cardiac Events (MACE), PCI compared to optimally medical treatment does not provide long-term clinical benefits.2, 21, 23 Other evidence has shown that the mortality rate and myocardial infarction are lower in individuals suffering from Chronic Coronary Syndrome treated with PCI compared to Optimal Medical Therapy.4, 14, 33
The management of CCS requires a comprehensive evaluation of the benefits and risks associated with PCI compared to OMT.1, 14 While PCI has been proven effective in reducing cardiovascular events in ACS, its role in CCS remains uncertain. The COURAGE trial and subsequent studies have provided valuable insights, but further research is needed to elucidate the optimal treatment strategy for CCS. 3 The aim of this research is to compare MACE between optimal therapy and Percutaneous Coronary Intervention in patients with objectively diagnosed CCS.
The Aim of the Study
To determine whether the management of Chronic Coronary Syndrome with revascularization (PCI + OMT) produces superior results than no revascularization (OMT only) in terms of the occurrence of MACE in patients.
Methodology
Trial Design and Oversight
This was a single-blind randomized control trial (RCT), aiming to compare MACE between optimal medical therapy and PCI in patients involving 378 patients with objectively diagnosed CCS in Indonesia. Patients were categorized based on the interventions received, either revascularization (PCI and OMT) or no revascularization (OMT only). We excluded patients with a history of CABG, stroke, heart failure, myocardial infarction, incomplete data, or those lost to follow-up, resulting in a final sample of 108 patients.
Study Population
Patients meeting the inclusion criteria were those diagnosed with Chronic Coronary Syndrome objectively meeting the requirements according to ESC Guideline and AHA Guideline. 1 The coronary stenosis was at least 70% in at least one proximal epicardial coronary artery, accompanied by objective evidence of myocardial ischemia (significant variations in ST-segment depression or T-wave inversion on the resting electrocardiogram or inducible ischemia with physical exercise or pharmacological vasodilator stress), or at least one coronary stenosis of at least 80% and classic angina without provocative testing. 3 The exclusion criteria were meticulously defined for patient selection. Patients with a history of coronary artery bypass grafting (CABG), stroke, or heart failure were excluded. Additionally, individuals with a documented history of myocardial infarction (MI) were not considered for enrollment. Furthermore, patients with incomplete medical records or those unable to undergo follow-up assessments were excluded from participation in the study. These criteria were established to ensure the selection of a specific patient population meeting the study’s objectives and to maintain data integrity throughout the research process. 34
Treatment
Patients were randomly allocated to either receive PCI with optimal medical therapy (PCI group) or receive only optimal medical therapy alone (medical-therapy group). A permuted-block design was utilized to create random assignments at each research site, with prior coronary-artery bypass grafting (CABG) as a stratifying variable. All patients received antiplatelet therapy, receiving 80 mg of aspirin per day or 75 mg of clopidogrel per day for patients with aspirin intolerance. Patients undergoing PCI were administered aspirin and clopidogrel, following established treatment guidelines and standard clinical practices. Medical anti ischemic therapy for both groups comprised long-acting metoprolol, amlodipine, and isosorbide mononitrate, individually or in combination, along with lisinopril or losartan for secondary prevention. Every patient underwent intensive treatment aimed at reducing low-density lipoprotein (LDL) cholesterol levels (atorvastatin or simvastatin alone or in combination with ezetimibe) to achieve a target range of 60 to 85 mg per deciliter (1.55 to 2.20 mmol per liter).
After attaining the LDL target, an effort was made to increase high-density lipoprotein (HDL) cholesterol above 40 mg per deciliter (1.03 mmol per liter) and to reduce triglyceride (TG) below 150 mg per deciliter (1.69 mmol per liter) through exercise, extended-release niacin, or fibrates, used alone or in various combinations. In patients receiving PCI, attempts were always made for target-lesion revascularization, and complete revascularization was done as deemed clinically appropriate. The success of PCI, as determined by angiography, was defined as achieving normal coronary-artery flow with less than 50% stenosis in the luminal diameter following balloon angioplasty and less than 20% after the placement of coronary stent, based on a visual assessment of the angiographic images taken before and after the procedure. Clinical success was characterized by achieving angiographic success along with no in-hospital myocardial infarction, emergency CABG, or mortality. Drug-eluting stents were not allowed for clinical use until the last 6 months of the study, hence only a few patients received these intracoronary devices.
Outcome
The primary outcome of this study is Major Adverse Cardiac Events (MACE), encompassing instances of mortality, stroke, myocardial infarction, and hospitalization attributable to heart failure. This comprehensive metric serves as a comparative gauge for assessing the efficacy of both treatment modalities under investigation. The clinical status of enrolled patients has been meticulously monitored over a period of 5 years, facilitating a thorough evaluation of treatment outcomes and long-term prognosis.
Statistical Analysis
The collected data comprise basic clinical characteristics and subject angiography, including age, gender, smoking status, diabetes, hypertension, heart failure, myocardial infarction, previous percutaneous coronary intervention (PCI), previous coronary artery bypass grafting (CABG), LVEF parameter in echocardiography, blood pressure, lipid profile, Body Mass Index (BMI), random blood glucose, medications, and Major Adverse Cardiac Events (MACE).
The data were analyzed using SPSS version 30.0 (IBM Corporation, Armonk, NY, USA). Numeric data obtained are presented as mean and standard deviation if the data distribution is normal. If the data distribution is not normal, median and minimum-maximum values are presented. Categorical data are presented as numbers and percentages. Normality of data distribution is assessed using the Kolmogorov-Smirnov test.
Changes in each numeric variable are evaluated using unpaired parametric T-tests if the data have a normal distribution. If the data are not normally distributed, the Mann-Whitney non-parametric test is used. All categorical variables are assessed using the Chi-Square test.
For paired numeric data, assessment is conducted using paired parametric T-tests if the data are normally distributed. If the data are not normally distributed, assessment is conducted using the non-parametric Wilcoxon test.
This study observes Major Adverse Cardiac Events (MACE) occurrence following 5 years of Optimal Medical Therapy and PCI, considering time, and will be presented with survival analysis.
Survival analysis steps include testing the Proportion Hazard (PH) assumption. If all variables meet the PH assumption, bivariate analysis will be conducted using Cox regression analysis and multivariate analysis using time-independent Cox regression analysis. If some variables do not meet the PH assumption, bivariate analysis will be conducted using Cox regression analysis for variables that meet the PH assumption, and multivariate analysis using Cox regression model interaction or stratification.
Survival analysis steps include testing the Proportion Hazard (PH) assumption. If all variables meet the PH assumption, bivariate analysis will be conducted using Cox regression analysis and multivariate analysis using time-independent Cox regression analysis. If some variables do not meet the PH assumption, bivariate analysis will be conducted using Cox regression analysis for variables that meet the PH assumption, and multivariate analysis using Cox regression model interaction or stratification. Hazard and survival functions will then be interpreted using Kaplan-Meier curve data application.
Result
Baseline Characteristics, Medical Therapy and Angiography Characteristic
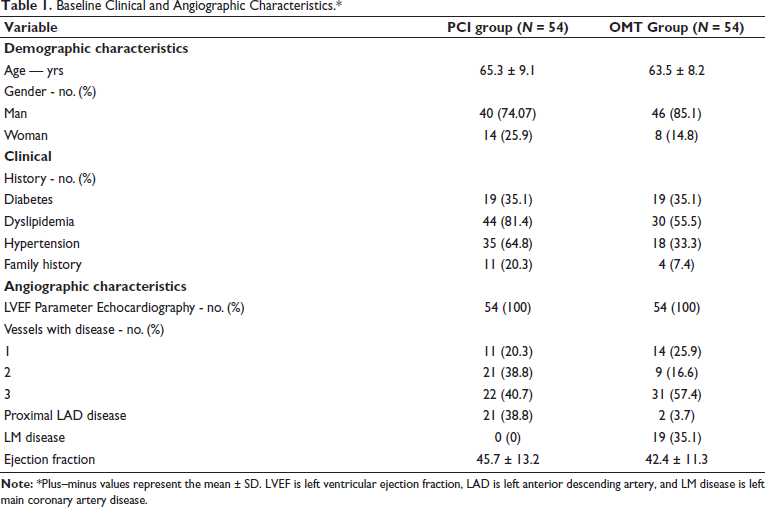
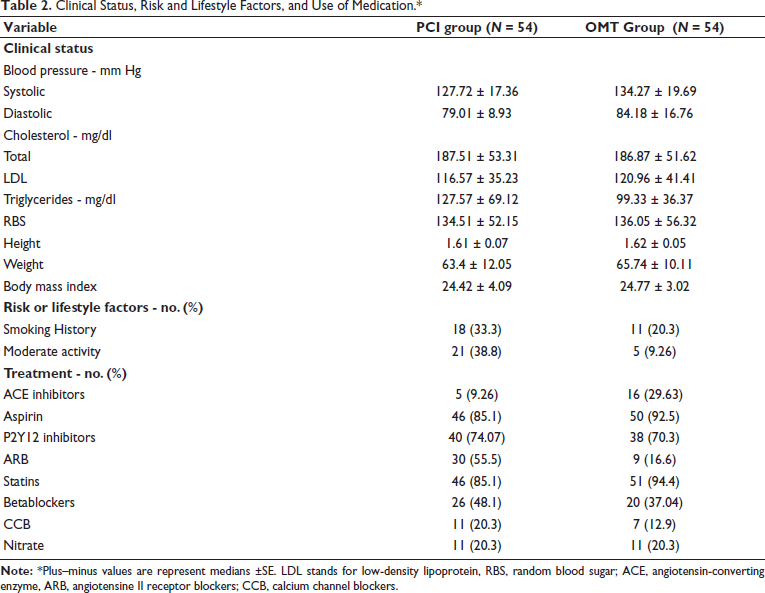
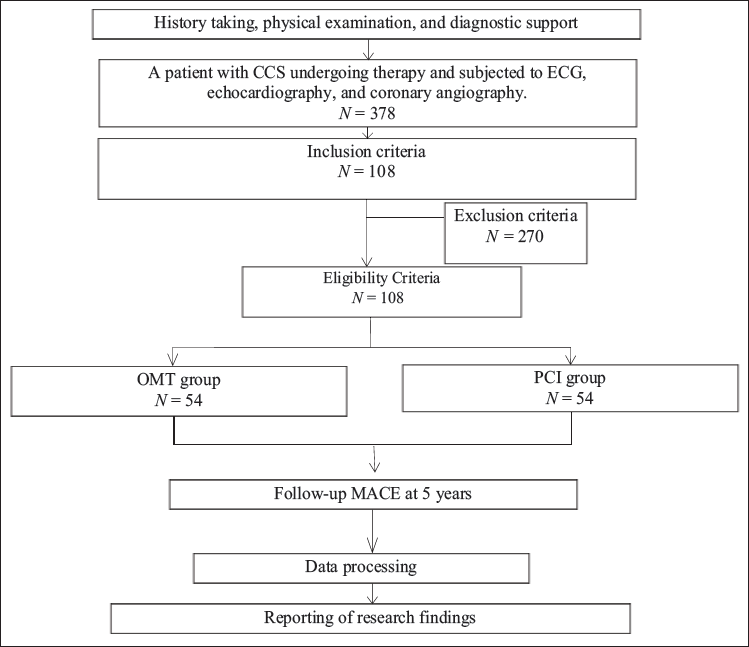
Between August 2015 and September 2021, a total of 108 patients participated in a trial conducted across two hospitals in Indonesia. Of these, 54 were randomly assigned to the PCI group, while the remaining 54 were allocated to the medical therapy group (see Figure 1 for enrollment details). Matching between the groups was performed to ensure comparability. The baseline characteristics of these patients were balanced in both groups (Table 1). All 108 patients (100%) exhibited objective evidence of Chronic Coronary Syndrome. All patients underwent coronary angiography, of whom 23.1% had one-vessel disease, 27.7% had two-vessel disease, and 49% had three-vessel disease. The baseline clinical and angiographic characteristics are depicted in Table 1. The clinical status, risk factors, lifestyle factors, and medication usage in both groups are presented in Table 2.
Baseline Clinical and Angiographic Characteristics.*
Clinical Status, Risk and Lifestyle Factors, and Use of Medication.*
Enrollment and Follow-up. Among all patients assessed for eligibility in the trial, 378 patients with CCS underwent therapy and were evaluated using ECG, echocardiography, and coronary angiography. A total of 278 patients were excluded for various reasons. Ultimately, 108 patients met all inclusion criteria and provided informed consent for study participation. The follow-up duration was 5 years for both study groups.
Major Adverse Cardiac Events Outcome
This study yielded a mortality outcome with an HR of 0.477 (95% CI 0.262-0.869), indicating that PCI can reduce mortality by approximately 52.3% compared to Optimal Medical Therapy (Table 3). The benefits of PCI have been demonstrated in the management of patients with ACS, but some studies have revealed that the positive effects of PCI remain highly controversial, especially in patients with CCS. According to the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial based on MACE, PCI compared to Optimal Medical Therapy does not provide long-term clinical benefits (95% CI 0.69-0.90, P=.03), Jari A Laukkanen 33 (RR 0.63; 95% CI 0.46-0.87), and De Bruyne et al, 35 indicating lower mortality rates with PCI compared to Optimal Medical Therapy.33, 35
MACE Outcome.
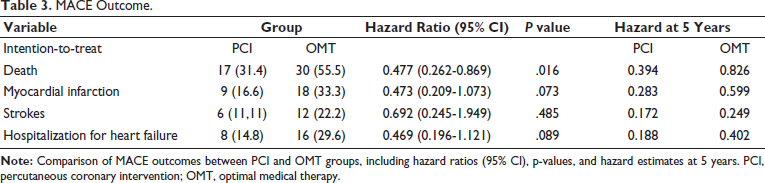
However, they contradict the findings of the study by Ibadete Bytyçi 2 (7.09 vs. 7.88%; P = .56), William E. Boden et al 36 (20.0% vs. 19.5%; hazard ratio, 1.05; 95% CI, 0.87 to 1.27; P=.62), and Sanhoury et al 37 (0 vs 0%), which indicated no variation in death rates between patients with CCS undergoing PCI compared to Optimal Medical Therapy.36, 37 Based on the analysis of myocardial infarction events, PCI can reduce the incidence of myocardial infarction in patients with CCS compared to Optimal Medical Therapy (HR 0.473, 95% CI 0.209-1.073). Although the P value did not reach conventional significance level (P > .05), there is a trend towards clinical significance (P = .073), suggesting that this difference has potential clinical relevance.
The findings of the myocardial infarction event analysis support the research conducted by Giuseppe Panuccio et al 38 (RR 0.79, 95% CI 0.69-0.90, P=.03), Jari A Laukkanen 33 (RR 0.69; 95% CI 0.52-0.92), and De Bruyne et al, 39 showing lower rates of myocardial infarction with PCI compared to Optimal Medical Therapy.33, 39 However, they contradict the findings of the study by Ibadete Bytyçi 2 (2.18 vs. 1.41%; P = .10), William E. Boden et al 36 (13.2% vs. 12.3%; hazard ratio, 1.13; 95% CI, 0.89 to 1.43; P=.33), and Sanhoury et al 37 (0 vs 0.9% P = 1.00), which reported no difference between patients with CCS undergoing PCI compared to Optimal Medical Therapy regarding myocardial infarction (7.69 vs. 8.29%; P = .32).36, 37 Based on the data analysis, the comparison between OMT and PCI in patients with chronic coronary syndrome shows significant results in the stroke variable. The hazard ratio (HR) for stroke in the PCI group was 0.692 with a 95% confidence interval (CI) (0.245-1.949), with a P value of 0.047. The HR value of 0.692 indicates that the PCI group has a lower risk of experiencing stroke compared to the Optimal Medical Therapy group. The CI (0.245-1.949) indicates the 95% confidence interval of the HR using SPSS version 30.
The findings of this data analysis support the research conducted by Jari A Laukkanen 33 (RR 0.63; 95% CI 0.46-0.87) that PCI shows a lower rate of stroke compared to Optimal Medical Therapy. 33 However, they contradict the findings of the study by Ibadete Bytyçi 2 (2.18 vs. 1.41%; P = .10), William E. Boden et al 36 (20.0% vs. 19.5%; hazard ratio, 1.05; 95% CI, 0.87 to 1.27; P=.62), and Sanhoury et al 37 (0 vs 0%), which reported no difference between patients with CCS undergoing PCI compared to Optimal Medical Therapy regarding stroke. Catheter manipulation along the aortic wall can cause embolization, which is suspected to contribute to the likelihood of experiencing of a stroke. The low post-PCI stroke rate may be due to the routine use of DAPT after stent implantation.
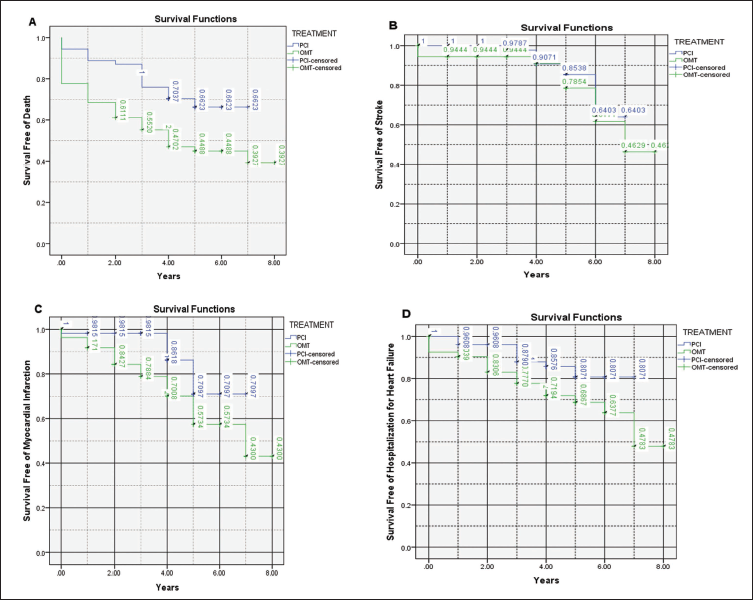
Based on the data analysis, the incidence of hospitalizations due to heart failure in the PCI group was 14.8% compared to 29.6% in the Optimal Medical Therapy group. The HR value of 0.469 indicates that the PCI group has a lower risk of hospitalization due to heart failure. The CI (0.196-1.121) indicates the 95% confidence interval of the HR. Since the CI encompasses the value of 1, this indicates that there is no significant difference between the PCI and Optimal Medical Therapy groups in terms of hospitalizations due to heart failure. Kaplan-Meier curves (see Figure 2) demonstrate the survival benefits of PCI in reducing mortality and MACE over 5 years.
Kaplan–Meier Survival Curves. In Panel A, the estimated 5-year mortality rate was 31.4% in the PCI group and 55.5% in the optimal medical therapy (OMT) group, with a hazard ratio of 0.477 (95% CI: 0.262-0.869), P = 0.016. In Panel B, the estimated 5-year incidence of stroke was 11.1% in the PCI group and 22.2% in the OMT group, with a hazard ratio of 0.692 (95% CI: 0.245-1.949), P = 0.485. In Panel C, the estimated 5-year incidence of myocardial infarction was 16.6% in the PCI group and 33.3% in the OMT group, with a hazard ratio of 0.473 (95% CI: 0.209-1.073), P = 0.073. In Panel D, the estimated 5-year incidence of hospitalization for heart failure was 14.8% in the PCI group and 29.6% in the OMT group, with a hazard ratio of 0.469 (95% CI: 0.196-1.121), P = 0.089.
Discussion
This study provides a comprehensive comparison between Optimal Medical Treatment (OMT) and Percutaneous Coronary Intervention (PCI) in patients with Chronic Coronary Syndrome (CCS) with respect to Major Adverse Cardiac Events (MACE). The analysis was conducted using a retrospective cohort design, focusing on key outcomes such as mortality, myocardial infarction, stroke, and heart failure hospitalization.
Our findings demonstrate a significant reduction in mortality associated with PCI compared to OMT, with a hazard ratio (HR) of 0.477 (95% CI 0.262-0.869). This suggests a 52.3% reduction in death risk among patients undergoing PCI. These results align with previous studies by Panuccio et al 38 and Laukkanen, 33 which also indicated lower mortality rates with PCI. However, they contrast with findings from Bytyçi et al 2 and Boden et al, 36 who reported no significant difference in mortality between PCI and OMT in CCS patients. 36 This discrepancy could be attributed to differences in study populations, methodologies, and follow-up durations.
In terms of myocardial infarction, our data indicate a trend towards lower incidence with PCI (HR 0.473, 95% CI 0.209-1.073, P=.073). While this did not reach conventional statistical significance, the clinical implications are noteworthy. This supports studies by Panuccio et al 38 and Laukkanen, 33 but not the findings of Bytyçi 2 and Boden, 36 highlighting ongoing debate in the field. 35
Stroke incidence was significantly lower in the PCI group (HR 0.692, 95% CI 0.245-1.949, P=.047), corroborating Laukkanen’s findings. 33 This suggests that the standard practice of using dual antiplatelet therapy (DAPT) post-stent implantation might mitigate the risk of embolic events associated with PCI procedures. Nevertheless, studies such as those by Bytyçi 2 and Boden 36 did not find significant differences, indicating the need for further research into patient-specific factors that might influence these outcomes. 36
Heart failure hospitalizations were also reduced with PCI (HR 0.469, 95% CI 0.196–1.121), though the confidence interval suggests that this finding is not definitive. This observation hints at a potential benefit of PCI in reducing subsequent cardiac decompensation, consistent with the overarching goal of revascularization to improve myocardial perfusion and function.
These results underscore the complexity of managing CCS and the necessity of individualized treatment approaches. While PCI shows clear benefits in reducing MACE, the decision to opt for revascularization should consider patient-specific clinical profiles, including symptom burden and comorbidities. The study’s limitations, such as its retrospective design and potential selection biases, must be acknowledged. Prospective randomized controlled trials (RCTs) with longer follow-up periods are warranted to validate these findings and to explore the mechanistic pathways underlying the observed benefits of PCI.
Of the 54 patients included in the OMT group, there were 19 patients with LM Disease. In our country, patients with severe diseases, especially LM disease, are unwilling to accept PCI treatment after being explained that there will be increased mortality and morbidity in the future. There is also no evidence that can show evidence of high mortality in patients with LM Disease. In patients with LM Disease, it is better to use CABG than PCI.
There are pros and cons that can be taken from this study. The pros of OMT are that no intervention is needed, lower direct risks such as infection and bleeding, smaller costs, focuses on relieving symptoms and on long-term management. The cons of OMT are that it requires high patient compliance, has the potential for worsening of the disease in the future, limited exercise capacity, and drug side effects. The pros of PCI are that it can reduce symptoms immediately, reduce MACE and increase exercise tolerance. The cons of PCI are the limitations of its intervention; it cannot be done in every place and requires higher costs.
Conclusion
Our study supports the efficacy of PCI in reducing MACE among CCS patients. These findings can inform clinical decision-making, suggesting that PCI should be considered, especially in individuals experiencing severe symptoms or high-risk profiles. Further research is essential to refine treatment algorithms and optimize outcomes for this patient population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The Ethics Committee of the Faculty of Medicine, Syarif Hidayatullah State Islamic University Jakarta approved the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent has been taken for the study.