
Abstract
Objectives
This study aimed to identify risk factors in patients diagnosed with angiographically significant coronary artery disease (CAD) after 65 years of age (elderly) with a subset analysis of more than 75 years, analyze their clinical, angiographic profile and assess their major acute cardiovascular and cerebrovascular events (MACCE).
Methods
This was an observational retrospective and prospective study conducted from January 2022 to June 2023 among consecutive elderly who underwent CAG for suspected or diagnosed CAD between 2010 and 2018 at a tertiary center in South India.
Results
A total of 1,511 patients satisfied eligibility criteria with mean age of 69.38 years and male preponderance (69%). Male gender, dyslipidemia and current tobacco use contributed to angiographically significant CAD by multiple logistic regression analysis but none of the risk factors contributed in the more than 75-year age group. Female patients had higher incidence of atypical presentation, less revascularizations and higher MACCE. Fourteen percent of patients with significant CAD developed MACCE over a median 3.5-year hospital follow-up. Survival analysis of 1,027 patients with significant CAD showed one, three, 5-year mortality rate of 4.3%, 6.9% and 10.8%, respectively, with left ventricular dysfunction and triple vessel disease being associated with worse survival. MACCE and 5-year survival was significantly better among those who underwent revascularization including those with significant left main or triple vessel disease.
Conclusion
This study showed a high prevalence of traditional risk factors in elderly patients among which male gender, dyslipidemia, current tobacco use were found to predict angiographically significant CAD. Triple vessel disease and left ventricular dysfunction were associated with worse survival. Mortality was significantly lower among elderly who underwent revascularization compared to medical management.
Introduction
Coronary artery disease (CAD) affects 1,655 per 100,000 individuals globally, and is expected to exceed 1,845 by the year 2030. 1 Krishnan et al. showed that definite CAD in Kerala increased nearly three times since 1993 in both urban and rural population. 2 with population aging being the most important contributing factor. CAD is the third leading cause of mortality worldwide 3 with more than 80% of deaths from cardiovascular disease estimated to occur in low and middle-income countries like India. 4
Elderly (more than 65 years age) account for more than half of cardiovascular hospitalizations and procedures as well as 80% of cardiovascular deaths. 5 Despite this, only few dedicated studies have evaluated CAD in them. In an analysis of recent late breaking clinical trials in Cardiology, 8 out of 22 trials did not include adults of age 60 to 80 and in the remaining, mean age was 54–66 years. 6 Recommendations have emphasized the need for more research for targeted prevention and management.
This study aimed to identify the risk factors in patients diagnosed with angiographically significant CAD after 65 years of age (elderly) with a subset analysis of patients more than 75 years and to analyze their clinical and angiographic profile, major acute cardiovascular and cerebrovascular events (MACCE) and survival.
Methods
This observational retrospective study was conducted between January 2022 to June 2023 in Department of Cardiology at a tertiary center in South India. Consecutive elderly patients who underwent coronary angiogram (CAG) for suspected or clinically diagnosed CAD after 65 years of age from 2010 to June 2018 were identified from the hospital database and assessed for eligibility. Patients who underwent CAG for other indications (hypertrophic cardiomyopathy, restrictive cardiomyopathy, chronic constrictive pericarditis, congenital heart disease, valvular heart disease, CAG prior to surgery) or were diagnosed with CAD before 65 years of age were excluded.
The presence of significant CAD was defined by the presence of 50 percent narrowing of intraluminal diameter of at least one of the major epicardial coronary arteries on CAG.
The baseline characteristics, risk factor profile, mode of presentation to hospital, clinical parameters and investigations at admission, coronary angiogram details, mode of management planned post CAG were extensively collected from the hospital database. Their follow-up data during outpatient visits till the end of study period and any hospitalization for occurrence of MACCE including acute coronary syndrome, stroke, re- interventions, heart failure hospitalization, mortality as well all treatment details were recorded in a detailed study proforma. Patients without follow-up visits to this hospital were contacted by telephone for details on outcomes after informed consent.
Statistical analysis was carried out using Stata 16.1 Stata Corp LLC. Categorical variables are presented as proportions and continuous variables as mean and standard deviation (SD) or median with inter quartile range (IQR) based on normality. Group comparisons were made using Student’s t tests, Chi-square tests, Fisher exact tests, and Mann–Whitney U tests as appropriate. Simple and Multiple Logistic regression was performed to identify risk factors associated with CAD. Kaplan-Meier survival models were performed and groups were compared using log-rank tests. Multivariate Proportional Hazard Model Cox regression analysis was employed for hazard ratio (HR) of all-cause mortality and MACCE. All confidence intervals were calculated to 95th percentile.
Results
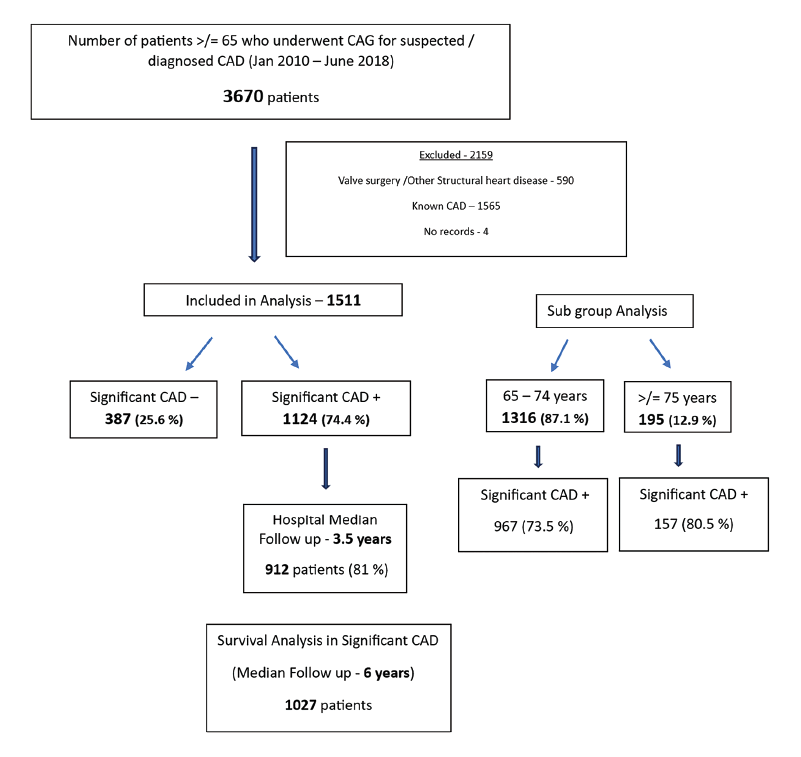
3670 consecutive elderly patients were screened and 1511 patients constituted the study group of which 12.9% were 75 years of age or more (Figure 1). 1124 (74.4%) patients had angiographically significant CAD of whom 912 patients had regular hospital follow-up and were analyzed for MACCE (median follow-up 3.5 years). Telephonic contact yielded survival data for 1027 patients (median follow-up 6 years).
Study Flow Chart.
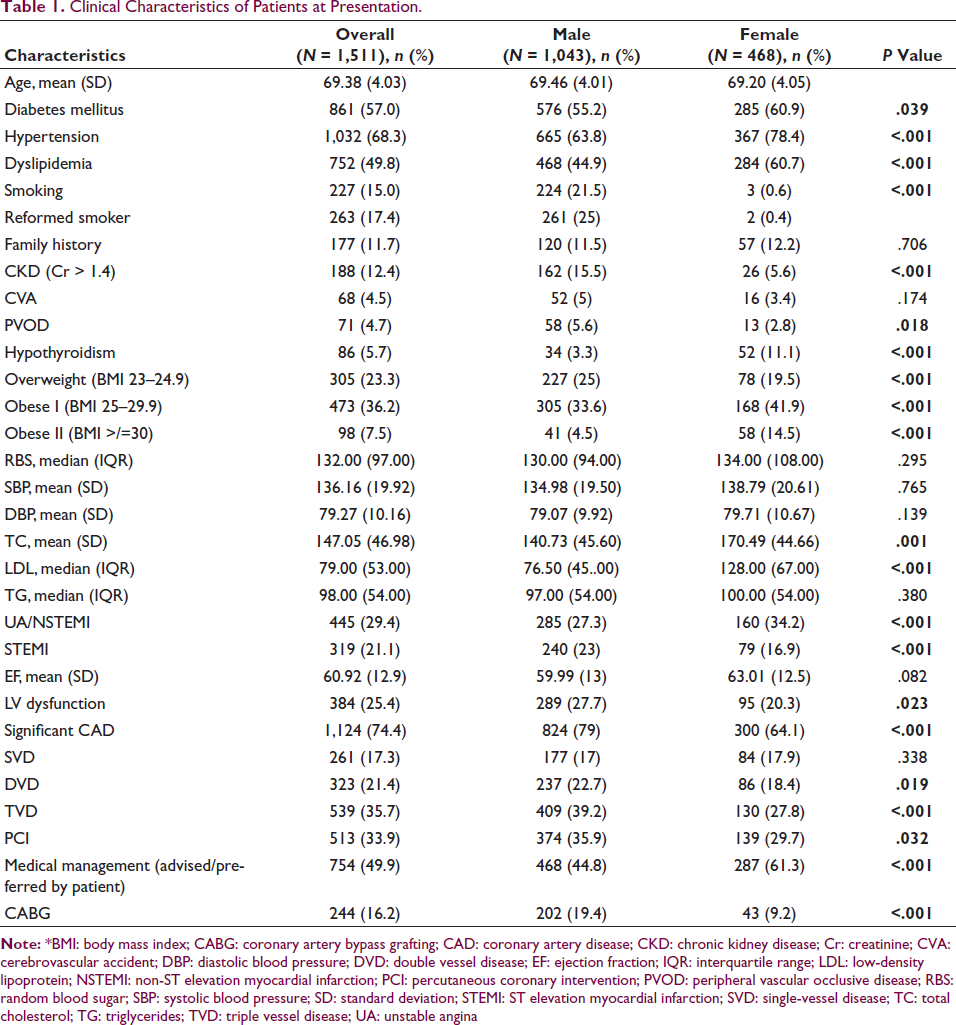
The mean age of total population was 69.38 (±4.03) years and had a male preponderance (69%). Prevalence of traditional risk factors and clinical characteristics of patients at presentation with gender wise distribution is shown in Table 1. Nearly all tobacco users were male (99%) with 15% current smokers at time of CAG. 43.7 % of patients were obese as per Asian standards. Only 1% of patients had none of the traditional risk factors.
Clinical Characteristics of Patients at Presentation.
Most patients presented with chronic stable angina (32%) followed by non-ST elevation acute coronary syndrome and ST Elevation myocardial infarction. 155 (10.3%) patients had clinical heart failure at presentation. IWMI (50% was most common type among STEMI but AWMI was more common in the more than 75 year subgroup (older subgroup). Approximately 42.6% STEMI patients underwent thrombolysis and was higher in the younger subset. Atypical chest pain, dyspnea on exertion and nonspecific ECG changes were significantly more common in women. Approximately 4% had severe LV dysfunction and 56.3% of patients had diastolic dysfunction at presentation.
Angiographically significant CAD was significantly higher in the older subgroup (P = .036) and in males (79% vs 64.1% in female patients; P < .001). Left main involvement (> 50% stenosis) in 5.7% and LAD involvement (>70% stenosis) in 51.5% of cases.
Angioplasty was significantly more among older subgroup (38% vs 33.5%; P = .014) whereas CABG was more in younger subgroup (17.5 vs 7.7%; P = .001).
Age, Male gender, Lower socioeconomic status, DM, Dyslipidemia, Current and reformed tobacco use, Obesity category II but not Hypertension, Family history were associated with angiographically significant CAD (Simple Logistic regression). None of the studied risk factors were found to contribute to CAD in older subgroup. Among those patients for whom laboratory parameters of major risk factors were available, many had uncontrolled risk factors (DM 58.4, HTN 35%, Dyslipidemia 41.3).
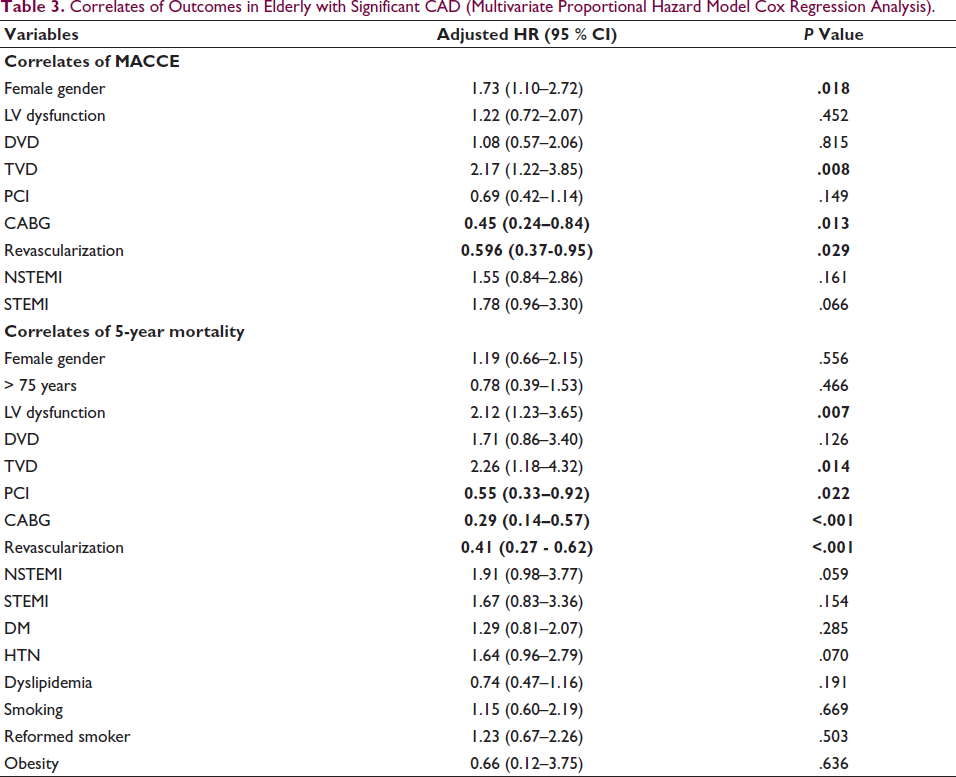
In-hospital follow-up in 912 patients with significant CAD over median follow-up of 3.5 years showed a MACCE rate of 14%. 6.7% had ACS on follow-up most common being NSTEMI. Revascularization was 3.8% and 3.4% patients needed HF hospitalization. A higher MACCE of 22.3% was recorded among those who completed 5 years follow-up in the hospital (439 patients). Factors associated with MACCE are shown in Table 3.
Association of Risk Factors with Angiographically Significant CAD (Multiple Logistic Regression Analysis).

Correlates of Outcomes in Elderly with Significant CAD (Multivariate Proportional Hazard Model Cox Regression Analysis).
In a subanalysis of patients having significant LM or TVD (N = 195 after excluding those lost to follow-up), 5-year MACCE was comparable for PCI versus medical management (26.7 % vs 45.2 %; P = .052), CABG and PCI (23.7 % vs 26.7 %; P =.674). CABG had lower MACCE versus medical management (23.7 % vs 45.2 %; P = .012).
Out of 1027 angiographically significant CAD patients, 79.3% and 33% completed 5-year and 10-year follow-up for mortality, respectively. Their survival analysis over a median follow-up of 6 years showed a 1, 3, 5, 10-year mortality of 44(4.3%), 71(6.9%), 111(10.8%), 187(18.2%), respectively. Kaplan–Meier analysis showed LV dysfunction and triple vessel disease were associated with greater mortality (Figure 2A and 2B, and Table 3) and worsening LV dysfunction showed a trend towards increased events. There was no significant variation among age subgroups, gender, various modes of presentation (Table 3).
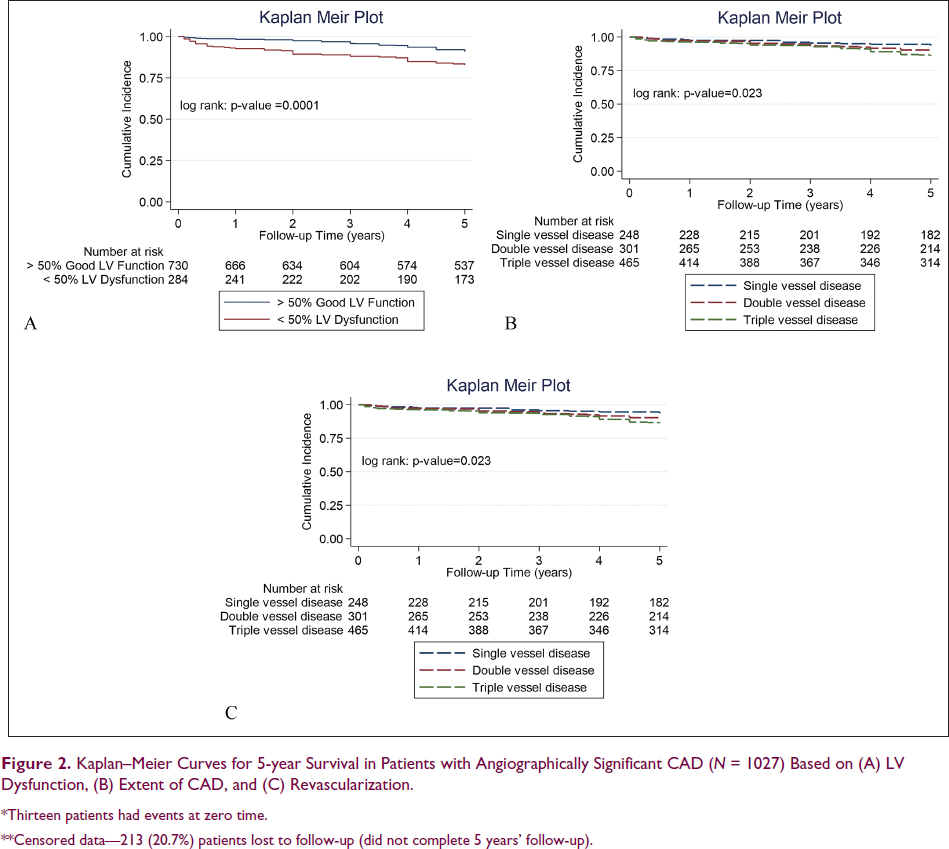
*Thirteen patients had events at zero time.
Those who underwent revascularization (CABG or PCI) had better survival compared to medical management (Figure 2C). Similar results were obtained on 10-year survival analyses also.
In significant LM or TVD (N = 389 after excluding those lost to follow-up), 5-year mortality rate was significantly lower among PCI versus medical management (12.5 % vs 27.1 %; P = .006) and also for CABG versus medical management (12.8% vs 27.1%; P = .002). CABG had no significant difference compared to PCI (12tab.8% vs 12.5%; P = .939).
Discussion
This study was conducted from January 2022 to June 2023 at a tertiary care center in South India among 1511 elderly patients (more than or equal to 65 years of age) admitted for CAG between January 2010 and June 2018 for either suspected CAD or a clinical diagnosis of CAD. Risk factor profile, clinical characteristics and MACCE in angiographically significant CAD were analyzed.
The major findings in this study are that there was a high prevalence of traditional risk factors in this cohort compared to other similar studies. Male gender, dyslipidemia and current tobacco use were significantly found to be contributing to angiographically significant CAD in elderly (Table 2) whereas none of the risk factors were found to be significant in the 75 years or more age group. Fourteen percent of patients with significant CAD developed MACCE over a median 3.5-year hospital follow-up. Female patients had significantly less revascularization and higher MACCE on follow-up. Triple vessel disease and LV dysfunction were found to significantly predict 5-year mortality rate in elderly. MACCE and survival were significantly better among those who underwent revascularization compared to medical management.
The mean age of this cohort is comparable to similar Indian studies7, 8, 9 but with a higher numbers (12.9%) in the older subgroup (having mean age 77.1 ± 2.55 years). 10 Equal risk for CAD in post-menopausal women was not reflected in elderly studies and male predominance persisted even among the older subgroup. This could be due to decreased access to health care especially in developing countries.
The prevalence of DM, HTN, Dyslipidemia, Obesity in this cohort was higher than population-based surveys such as ICMR INDIAB 13 as well as CAD studies in India. 7, 9, 10, 11 Only 1% had none of the traditional risk factors. We also found that despite women having higher prevalence of most major risk factors, female gender was not significantly associated with angiographically significant CAD. This supports the theory that women are more prone to nonobstructive CAD spectrum. Smoking history in 33% among which 15% were current smokers was contrary to what was shown earlier that prevalence decreases with age. This impresses upon the need to aggressively bring down modifiable risk factors even in elderly patients.
There was a significantly higher prevalence of CAD in older subgroup (80.5% vs 73.5%; P = .036) similar to AHA reports. 14 Few studies have looked into whether the same traditional risk factors contribute to CVD in elderly and they all show conflicting results7, 8, 9. Our findings are similar to Mukherji et al. 8 despite being conducted nearly three decades apart. Some studies done in very elderly showed that only hypertension15, 16 or none of the major risk factors 17 contributed to CAD which our analyses among 75 year and older also suggests.
The lack of significant contribution by DM, HTN, family history of CAD, and Obesity may suggest that they contribute less to the development of atherosclerosis in elderly. Another important explanation could be that significant proportion of patients with these risk factors have expired and we may have inadvertently selected a healthier population. In view of conflicting results in various studies, we can only suggest that traditional risk factors do not predict the presence of CAD with the same degree as in younger individuals but they continue to play a role. More than one-third of patients with available data had uncontrolled DM, HTN, dyslipidemia on follow-up despite being in a tertiary set up. Elderly need equal or rather more attention with respect to modifying risk factors, clinical management and formulating guidelines.
NSTE-ACS was the most common presentation9, 16, 18, 19 similar to previous ACS studies. IWMI was most common7, 9 while in NORIN STEMI study with a younger cohort, AWMI was the most common. Thrombolysis was performed in only 42.6% of patients and was significantly less in the older subgroup (30.4%) which could be explained by higher contraindications or higher rates of Primary PCI in our setup. Multivessel disease was more common as shown in previous elderly registries indicating more extensive atherosclerosis.
Age related factors such as frailty, comorbidities, and unwillingness to undergo intervention could be the reasons for half the patients being kept on medical follow-up. PCI was significantly more in older elderly probably due to higher surgical risk.
Women were significantly less likely to undergo revascularization and had significantly higher MACCE highlighting the gender differences which however did not translate to worse survival. Higher bleeding events, vascular complications, decreased compliance to follow-up and medication could be factors. The higher MACCE (22.3%) among those who completed 5-year hospital follow-up could be more reflective of actual rates.
CAD in elderly has poor prognosis with 3-year STEMI mortality rate as high as 52% and 1-year mortality exceeding 25% in NSTE-ACS depending on the median age, study setting, and type and frequency of interventions. 20 NORIN STEMI Study where 66% underwent PCI showed 11% 1-year mortality which was significantly contributed by female patients (12% vs 5% in males). Sharma et al. 9 and Bhatia et al. 7 showed significantly higher in-hospital mortality in acute MI compared to nonelderly (20.6% and 28.04%, respectively). However, survival rates in this study reflected good outcomes with 1-year mortality rate of 4.3%, 3-year mortality rate of 6.9% and 5-year mortality rate 10.8% with no gender difference. This being a tertiary center in a state with higher socioeconomic indices could have resulted in better compliance to management and follow-up leading to better outcomes.
Studies have shown that revascularization has better prognosis for STEMI while taking age-related factors into account, but this is not clear for SIHD, NSTE-ACS. TIME study which recruited only elderly patients (75 years or more) with SIHD showed that QOL, MACCE was better at 6 months but there no difference on 4-year follow-up. While GRACE, CRUSADE, TACTICS TIMI showed that invasive management is better, 20 Savonitto et al. 21 showed that there was no difference versus conservative management in NSTE-ACS. In this study, MACCE over 3.5-year follow-up and survival was significantly better with revascularization which could be the result of better outcomes among ACS patients which constituted 50 % of cases.
In large studies such as ISCHEMIA trial, medical management was noninferior to revascularization in SIHD. This study supports revascularization among significant LM (>50% lesion) or TVD in whom 5-year mortality rate was significantly better. While there was no significant difference between and CABG and PCI, CABG had lower MACCE. Suboptimal medical management in elderly due to various issues such as decreased compliance, polypharmacy, drug interactions and side effects could be an important factor. Hence, further dedicated research in elderly is needed to decide on the optimal mode of management.
Limitations
This was a single center retrospective observational study. The risk factors contributing to CAD in elderly were not compared with a younger age group. Patients with borderline lesions on CAG which do not exactly reflect insignificant CAD were also included for comparison. Patients who were lost to follow-up were contacted over telephone for outcomes which may be unreliable data and hence these patients were included only in survival analysis.
Conclusion
This retrospective observational study showed a high prevalence of traditional risk factors in elderly patients among which male gender, dyslipidemia, current tobacco use predicted angiographically significant CAD. MACCE and survival rates were better when compared to previous studies in this cohort and were predicted by the presence of triple vessel disease and left ventricular dysfunction. Mortality was significantly lower among elderly who underwent revascularization in this study.
Abbreviations
AHA: American Heart Association; DM: Diabetes mellitus; FHS: Framingham Heart Study; GBD: Global burden of disease; HTN: Hypertension; LM:Left main; LV:Left ventricle; NSTE-ACS: Non ST elevation-Acute coronary syndrome; QOL: Quality of life; SIHD: Stable ischemic heart disease; TVD: Triple vessel disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Statement
This study was approved by Institutional Ethics Committee of SCTIMST (IEC/1877).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.