
Abstract
Introduction
The onset and progression of chronic kidney disease (CKD) are strongly linked to a decrease in Klotho, which was once thought to have an anti-aging effect. The specific mechanism of this enzyme’s connection with CKD and its related co-morbidities has to be investigated further. Present study aimed to test Klotho levels in various phases of CKD and to study their correlation with cardiac morbidity.
Methods
Present study was single-center, observational, cross-sectional study conducted in all genders with age ≥18 years who presented with CKD stages G1-G5 ND. All cases underwent battery of investigations including estimation of serum Klotho & FGF 23 levels along with 2D echocardiography.
Results
Most study participants were found to be in CKD stage G2 (24%) followed by stages G4 and G5 (18% each). On cardiac evaluation, low LVEF was detected in 38% cases, diastolic dysfunction in 44% & LV hypertrophy in 48% cases. There was a negative correlation between serum Klotho levels and LVH (P = .009), LVEF (P = .015) or LV diastolic dysfunction (P = .005). Likewise, there was positive correlation between serum FGF 23 levels and LVH (P = .0001), LVEF (P = .0001) or LV diastolic dysfunction (P = .0001).
Conclusions
With our study, we want to emphasize the prognostic value of Klotho and FGF 23 in routine evaluation of CKD patients. Low serum Klotho & high FGF 23 levels were associated with low left ventricular ejection fraction (LVEF), left ventricular hypertrophy (LVH) and left ventricular dysfunction among CKD patients.
Keywords
Introduction
Chronic kidney disease (CKD) is a systemic disease that affects the function and structure of the kidneys in an irreversible manner over months or years. Its frequency has been estimated to be as high as 13% globally 1 and 17.2% in India. Diabetes and hypertension account for more than two-thirds of CKD cases in Western countries. 2 Diabetes and hypertension account for 40%-60% of CKD cases in India nowadays. 3 According to data from the Indian Council of Medical Research, the prevalence of diabetes in the Indian adult population has risen to 7.1% (ranging from 5.8% in Jharkhand to 13.5% in Chandigarh), with a prevalence of 28% in the urban population (over the age of 40 years).4, 5 More evidence has been revealed that the onset and progression of CKD are strongly linked to a decrease in Klotho, an enzyme encoded by Klotho gene, once thought to be an anti-aging gene. There are three subfamilies of Klotho: α-Klotho, β-Klotho, and γ-Klotho. α-Klotho activates FGF23, and β-Klotho activates FGF19 and FGF21. The Klotho gene is mostly expressed on the cell surface membrane of the proximal and distal renal tubules. 6 In addition, new evidence suggests that Klotho is not only an early indicator of CKD, but also a potential therapeutic target for the disease. 7
The majority of Klotho research has focused on its role as a renal cofactor for FGF23 binding. The phosphaturic effect of FGF23 is elicited by the presence of Klotho in the kidneys, as is the inhibition of the production of the active form of vitamin D. 8 The discovery of a soluble form of Klotho and, more critically, its expression in vascular tissue and blood has allowed this molecule to be considered a new factor with substantial effects in various organs, including the cardiovascular (CV) system. 9
The Kidney Disease-Improving Global Outcomes (KDIGO) workgroup recommends a broader term, CKD–mineral and bone disorder (CKD-MBD) for the systemic disorder of mineral and bone metabolism due to CKD. 10 The term renal osteodystrophy is exclusively used to describe the bone morphology disorders in CKD. The clinical diagnosis of CKD-MBD broadly encompasses serum levels of calcium, phosphate, intact parthormone (iPTH) and 25(OH) vitamin D. FGF23 and Klotho levels can supplement these tests in management of CKD-MBD and KDIGO recommends new studies in this field. 10
The specific mechanism of this marker’s connection with CKD and its related co-morbidities has to be investigated further. Present study aimed to determine Klotho levels in various phases of CKD and to find out its correlation with cardiac morbidity.
Materials and Methods
Present study was a single-center, observational, cross-sectional study conducted at a tertiary care center in New Delhi, India. Study duration was of two years (July 2018 to June 2021). Study was approved by an institutional ethical committee.
Inclusion criteria
All genders, with age ≥ 18 years, with CKD stages G1-G5 ND.
Outdoor patients visit outpatient department as well as indoor (admitted) patients regardless of reason for admission.
Exclusion criteria
Patients with sepsis.
Patients with malignancy.
Patients with CAD.
Patients with Hepatitis-B, Hepatitis-C.
Patients with HIV.
A written informed consent was taken from the patients. The complete demographic, personal and clinical & treatment history was taken. A history of co-morbidities such as hypertension, diabetes etc. was determined and the duration of CKD was obtained. The severity of CKD was assessed based on the KDIGO guidelines which used GFR. 11
Each case was subjected to battery of investigations which included kidney function tests (urea, creatinine, sodium, potassium, calcium, and phosphate), Klotho levels, FGF-23 levels, HBsAg, Anti-HCV, & Anti-HIV serology, hemogram and thyroid function test. A commercial enzyme-linked immunosorbent assay (ELISA) was performed to measure serum Klotho levels according to manufacturer’s protocol (Human soluble α-Klotho Assay Kit JP27998, Immuno-Biological Laboratories Co., Ltd., Gunma, Japan). The quantification was performed spectrophotometrically using a FLUOstar OPTIMA Microplate Reader (ThermoFisher Scientific, Waltham, MA) and Optima Control software version 2.20 (BMG LABTECH GmbH, Offenburg, Germany). Serum intact FGF23 levels were analyzed by commercially available second-generation quantitative ELISA kit (Immutopics, Inc. San Clement, CA) according to manufacturer’s instructions. Intact FGF23 assay detects exclusively biologically active FGF23.
An echocardiography was conducted in the Department of Cardiology to observe cardiac parameters. Outcome measures were cardiac abnormalities: left ventricular hypertrophy (LVH), left ventricular ejection fraction (LVEF), and diastolic dysfunction as per stages of CKD. LVEF of <50% was considered as low LVEF. Diastolic dysfunction was assessed by integrating pulsed wave Doppler examination of mitral inflow before and during Valsalva maneuver and of pulmonary venous flow and Doppler tissue imaging of the mitral annulus. The four recommended variables for identifying diastolic dysfunction and their abnormal cutoff values are annular e’ velocity. Septal e’ < 7 cm/sec, lateral e’ < 10 cm/sec, average E/e’ ratio > 14, LA volume index > 34 ml/m², and peak TR velocity > 2.8 m/sec. LV diastolic function is normal if more than half of the available variables do not meet the cutoff values for identifying abnormal function. LV diastolic dysfunction is present if more than half of the available parameters meet these cutoff values. The study is inconclusive if half of the parameters do not meet the cutoff values. LV hypertrophy was defined as LVMI greater than 118 g/m2 (men) or 108 g/m2 (women).
Data was collected and compiled using Microsoft Excel, analyzed using SPSS 23.0 version. Frequency, percentage, means and standard deviations (SD) were calculated for the continuous variables, while ratios and proportions were calculated for the categorical variables. Differences of proportions between qualitative variables were tested using chi-square test or Fisher exact test as applicable. ANOVA/ Kruskal Wallis test was used to associate quantitative variables with stage. Univariate or multivariate logistic regression was implied to find out risk factors for cardiac abnormalities. P value <.05 was considered statistically significant.
Results
Fifty cases were included in the study. Demographic characteristics of the cases included in the study have been depicted in Table 1. Most of the cases were middle-aged. Majority of cases were male (58%) and females were 42% of all cases. Most of the cases were overweight or obese, and 40% cases were diabetic while nearly half of the cases were hypertensive. Among study participants, most common presenting complaint was shortness of breath (68%), followed by pedal edema (56%), and anorexia (38%).
Demographic Characteristics of Cases Included in the Study.
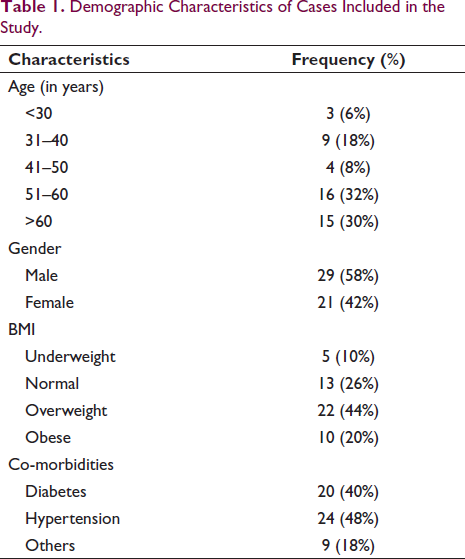
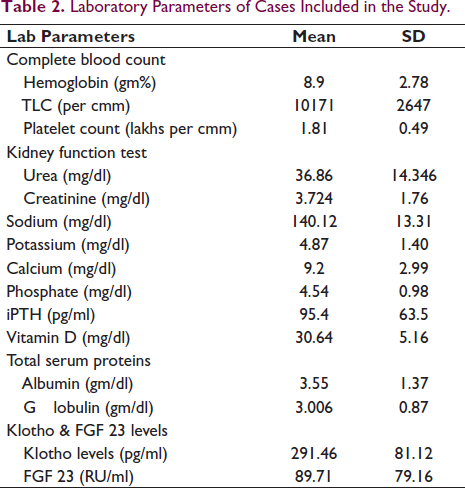
Table 2 depicts the laboratory parameters of cases included in the study. Among study participants, mean serum Klotho level was 291.46 ± 89.71 pg/ml, while mean FGF 23 was 89.71 ± 79.16 RU/ml.
Laboratory Parameters of Cases Included in the Study.
Distribution of study participants according to stage of CKD and corresponding mean Klotho and FGF 23 level has been depicted in Table 3. Mean serum Klotho level was lowest in CKD stage G4 and highest in stage G1. However, serum FGF 23 level was highest in CKD stage G5 ND and lowest in stage G1. Also, it was found that the difference between serum Klotho and FGF 23 levels across different CKD stages was statistically significant (P < .0001)
Distribution of Study Participants According to Stage of CKD.
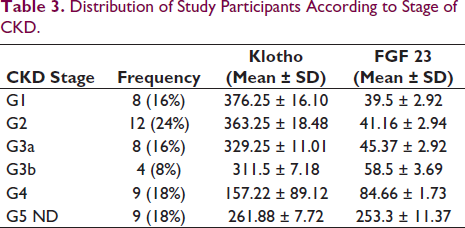
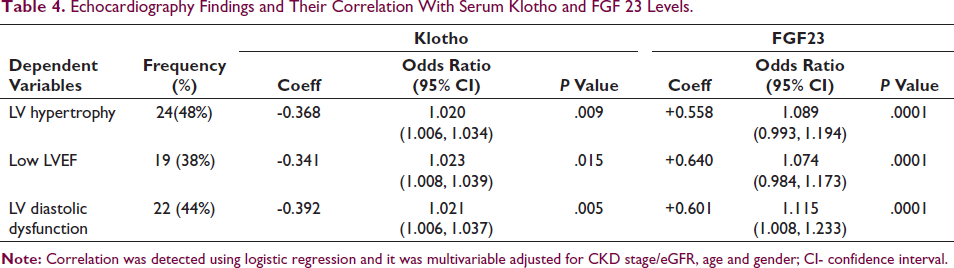
Table 4 depicts the echocardiography findings and their correlation with serum Klotho and FGF 23 levels along with the odds ratio and 95% confidence interval. Correlation was detected using logistic regression and it was multivariable adjusted for CKD stage/eGFR, age and gender. Among study participants, most common echocardiographic abnormality was LV hypertrophy (48%) followed by diastolic dysfunction (44%). A negative correlation has been found between Klotho levels and echocardiographic abnormalities. Also, a positive correlation was found between FGF 23 levels and echocardiographic abnormalities. The negative correlation with serum Klotho was strongest for LV diastolic dysfunction followed by LV hypertrophy. The positive correlation with FGF 23 was strongest for low LVEF followed by LV diastolic dysfunction. Fourteen cases (28%) were found to have heart failure with preserved ejection fraction and similar to those with reduced ejection fraction, a negative correlation with serum Klotho and a positive correlation with serum FGF 23 levels was found.
Echocardiography Findings and Their Correlation With Serum Klotho and FGF 23 Levels.
Discussion/Conclusion
It is well known that the advancement of CKD has consequences over other organs, causing many unfavorable systemic effects including CV illnesses and increased mortality. 2
CKDs seem to be present among middle age group individuals. The findings of our study were consistent with the studies done by Abdallah et al., 12 (58.6 ± 19.3 years), Tanaka et al., 13 (63.3 ± 13.2 years), Kim et al., 13 (53.6 ± 12.2 years), and Khodeir et al., 15 (57 ± 12.5 years). In our study, we found male preponderance which was consistent with studies done by Abdallah et al., 12 Kim et al., 14 and Khodeir et al. 15
In our study, diabetes was present among 40% cases and hypertension among 48% cases. In study done by Abdallah et al., 12 diabetes was detected in 37.5% cases while hypertension was detected in 30.7% cases. Similarly in study done by Kim et al., 14 diabetes was present in 33.9% and hypertension in 96.1% cases. In a study done by Sarah Seiler et al., 16 diabetes mellitus was reported in 38% cases and CV disease prevalence was 30%. In a study done by Yuvaraj et al., 17 diabetes was present among 61.8% and hypertension among 88.1% cases.
In our study, we found a mean Klotho level of 291.46 ± 89.71 pg/ml and mean FGF 23 level of 89.71 ± 79.16 RU/ml. In study done by Abdallah et al., 12 , mean Klotho level was 477.9 ± 76.2 and mean FGF 23 level was 60.5 ± 17.6. Similarly, in a study done by Kim et al., 14 median Klotho levels were 536 pg/ml with a range of 420 and 667 pg/ml. In study done by Khodeir et al., 15 mean Klotho level was 5.36 ± 3.57 ng/ml and mean FGF 23 level was 1182.26 ± 427.5 pg/ml. Anbarasan et al. 18 documented a mean FGF 23 level of 730.7 ± 492.7 pg/ml. In our study, lower mean Klotho level has been documented compared to data from other international studies pointing toward the geographical variability of its expression which needs to be further studied in larger studies. Also, in our study, Klotho levels were highest in stage G1 and decreased in each stage, lowest values being in G4 but we found a slight rise in level in G5. However, the level was lower than G3. There was a sharper decline from G3 to G4 which creates relative perception of higher Klotho level in G5. Small sample size could be one of the reasons for such disparity.
In our study, we determined a negative correlation between Klotho levels and LVH, LVEF, & LV diastolic dysfunction. Also, there was positive correlation between FGF 23 levels and LVH, Low LVEF or LV diastolic dysfunction. Similar finding was found in study done by Tanaka et al. 13 After adjusting for age, gender, eGFR, calcium, and inorganic phosphate, the association between the highest FGF23 tertile and poor LVEF was shown to be significant. Patients with low Klotho levels were significantly associated with LVH and low LVEF. However, our study findings were contradicted by the study done by Sarah Seiler et al., 16 which depicted that serum Klotho levels were not significantly associated with CV parameters. However, our study findings were coherent in regards with serum FGF 23 levels which were significantly associated with CV parameters. In study done by Anand et al., 17 investigations comparing FGF23 levels with biochemical parameters and CV state revealed that greater FGF23 levels were directly linked to increased cardiac mortality. On 2D-Echo, patients with a poor ejection fraction, a thicker IVS, and a larger left ventricular mass index had a higher FGF23. In a study done by Silva et al., 19 a multinomial regression analysis revealed that lower Klotho levels and higher FGF-23 levels were associated with an increased risk of concentric hypertrophy. Klotho, FGF-23, and heart geometry groups were statistically significant as independent factors of CV hospitalization in the generalized linear model (GLM) (P = .007). these findings were consistent with our studies.
Our study had a few limitations. This study was cross-sectional observational study. It was done at a single-center and does not represent entire India. A larger multicenter study will be required to better understand the geographical diversity of this enzyme in the Indian subcontinent and also to validate its correlation with different CV parameters. Also, the study was limited by small sample size and we could not account for influence of comorbodities like diabetes, hypertension and anemia.
With our article, we want to emphasize the prognostic value of Klotho and FGF 23 in routine evaluation of CKD patients. Their level can predict cardiac morbidity and early detection could be life-saving. A better knowledge of the cellular and molecular processes behind Klotho and FGF23’s effects on CKD progression and CVD development will aid in the development and implementation of innovative treatment options. Collaborative and translational research is essential for improving bench-to-bedside transfer.
Conclusions
With our study, we want to emphasize the prognostic value of Klotho and FGF 23 in routine evaluation of CKD patients. With CKD progression, serum Klotho levels decrease and FGF 23 levels increase. Low serum Klotho levels and high FGF 23 Levels were associated with low LVEF, LVH, and diastolic dysfunction.
Author Contributions
The authors, Dr Manoj Kumar, Dr Vinod Chaitanya, Dr Himanshu Verma, Dr Charu Madan, Dr Anwar H Ansari and Dr Sourabh Sharma have contributed equally in conception and design of manuscript, analysis and interpretation of data and final approval of the manuscript.
Data Availability Statement
Data is available with corresponding and first author.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Subjects have given their written informed consent. The study protocol was approved by the institutional ethical committee of VMMC & Safdarjung Hospital.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.