
Abstract
Background
When the endothelium of the coronary artery is damaged, it exposes the underlying structure to a series of events that can cause complete blockage and a myocardial infarction with ST-segment elevation (STEMI). One of the key factors in this process is a protein called von Willebrand factor (vWF) that helps platelets adhere to the damaged area. Our objective was to investigate the importance of measuring vWF levels in patients with STEMI to determine the severity of their coronary artery disease (CAD) on angiography.
Methods
The study included 30 patients who experienced their first STEMI. Patients with a history of CAD, cardiomyopathies, valvular heart disease, atrial fibrillation, anticoagulants, coagulation disorders, and pregnancy were not included in the study. After informed consent, all patients were subjected to routine blood investigations, electrocardiography, echocardiography, and coronary angiography. Blood samples were collected for vWF Ag within 24 hours of the patients’ arrival at the hospital. After the angiography, the coronary arteries were evaluated for stenosis and quantified using the modified Gensini score (mGS). The score was then correlated with vWF Ag levels using the Spearman rank correlation. Additionally, the receiver operating characteristic (ROC) curve was plotted for the value of vWF Ag levels to detect significant CAD.
Results
The average age of the group was (49.77 ± 10.79) years. The average levels of vWF Ag were (204.17% ± 51.99%). Patients with an mGS score of over 150 had higher levels of vWF Ag than those with a score of under 100 (P < .001). There was a positive correlation (r2: 0.67) between the parameters. On the ROC curve, vWF Ag levels higher than 186% predicted the presence of CAD, with an area under curve indicating sensitivity and specificity.
Conclusion:
In patients with STEMI, higher levels of vWF Ag were found to be associated with a greater severity of CAD.
Introduction
The development of atherosclerotic plaque in the coronary artery wall is the primary cause of coronary artery disease (CAD). This plaque can lead to thrombus formation by rupture or erosion, which in turn can result in acute myocardial infarction (AMI).1, 2 Depending on the extent of the thrombus blocking the artery lumen, AMI can be categorized as NSTEMI or STEMI. The latter is the leading cause of morbidity and mortality worldwide. The primary focus of STEMI management is to restore blood flow in the coronary artery either through drugs or percutaneous intervention. 3 The goal is to achieve coronary artery patency as early as possible to save the myocardium. Thrombosis is a significant factor in atherosclerotic CAD. 4 Several factors, including atheroma, can predispose thrombus formation in the coronary artery. Recently, the von Willebrand factor (vWF) has been of interest. This multimeric glycoprotein is found in endothelial cells, alpha granules of platelets, and plasma. 5
While plasma vWF Ag levels have been assessed in CAD patients, the results have been diverse. However, there are no studies on STEMI.6–9 Therefore, a study was conducted to evaluate the correlation between the angiography severity of CAD quantified by the mGS and vWF Ag levels.
Materials and Methods
A prospective observational study was conducted on 30 patients who were over 18 years and under 80 years of age and had experienced their first episode of STEMI. The study was done only after obtaining consent from the Institutional Ethics Committee, and all patients included in the trial provided written informed consent. Patients with unstable angina, liver, and renal failure, tachyarrhythmias, myocarditis, valvular heart disease, and pacemaker implantation were excluded from the study.
The data of each patient regarding medical history, age, sex, hypertension, diabetes mellitus, and smoking were collected. Within 24 hours of admission, all patients underwent echocardiography and angiogram, and a blood sample was taken for the assessment of the vWF Ag level. The plasma levels of vWF Ag were detected using an enzyme-linked immunosorbent assay.
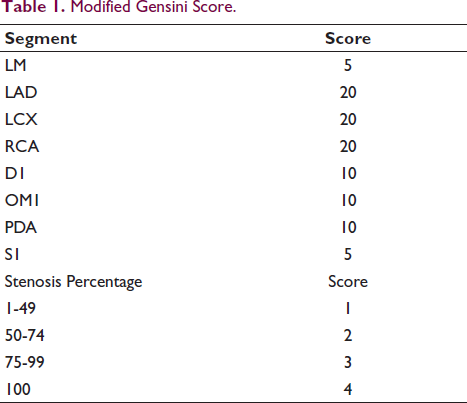
The severity of CAD was assessed using mGS, which involves dividing the coronary arterial system into eight segments and evaluating the diameter of the stenosis in each segment to get an overall score. 10 The most severe diameter stenosis is taken for grading (1: [11%-49%], 2: [50%-74%], 3: [75%-99%], 4: [100%] occlusion), resulting in a score range of 0 to 32. The extent of myocardium being affected by the stenosis in each segment was determined by multiplying a number by the grade of stenosis in the segment. The number is 5 for the left main; 20 each for the left anterior descending, left circumflex, and right coronary arteries; 10 each for the main diagonal, obtuse marginal, and posterior descending branch; and 5 for the first septal. If the obtuse marginal branch is large, the factor would be (20) (Table 1).11, 12
Modified Gensini Score.
Statistical Analysis
The data collected for this study were analyzed using statistical software called SPSS, version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive and inferential statistical analysis was conducted. Continuous and categorical variables were presented as mean + SD (range: minimum to maximum) and percentage, respectively. The chi-square test was used to determine the significance of categorical variables among the groups. A two-tailed independent student t-test was used to determine the statistical significance of research parameters on a continuous scale between 2 groups. This analysis focused on metric parameters in an intergroup comparison. The correlation between the vWF and mGS was assessed using the Spearman rank correlation. To predict the presence of significant CAD, we used the receiver operating characteristic (ROC) curve to find the average value of the vWF Ag levels.
Results
Baseline Characteristics
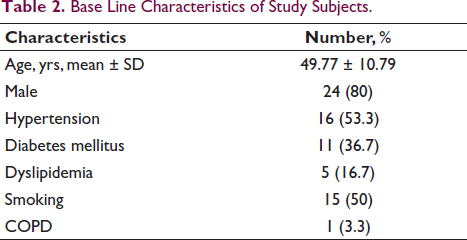
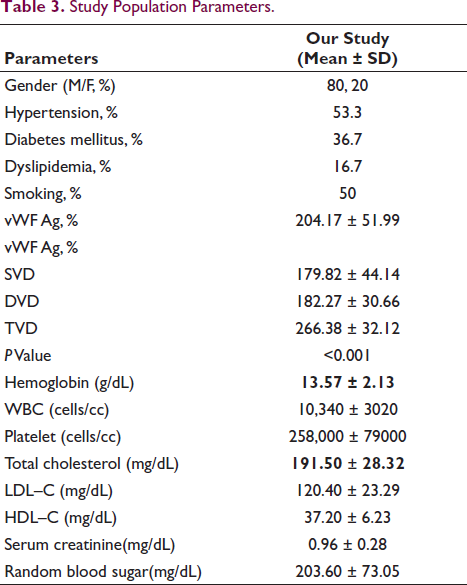
The demographic characteristics of the patients are presented in Table 2. Out of the 30 patients, 24 were male, and the average age of the group was 49.77 ± 10.79 years. Among the risk factors, 16 patients (53.33%) had hypertension, 11 patients (36.67%) had diabetes, 15 patients (50%) smoked, and 5 patients (16.67%) had dyslipidemia. All patients presented with chest pain, and two-thirds of them experienced sweating (Table 3). Anterior wall STEMI was observed in 60% of patients, and inferior wall STEMI was observed in 40% of patients. All patients were treated with Tenecteplase within the treatment window.
Base Line Characteristics of Study Subjects.
Study Population Parameters.
vWF Ag Levels in the Study Population
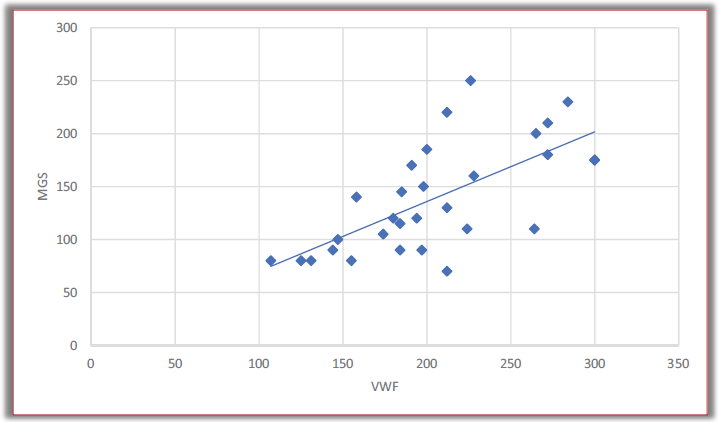
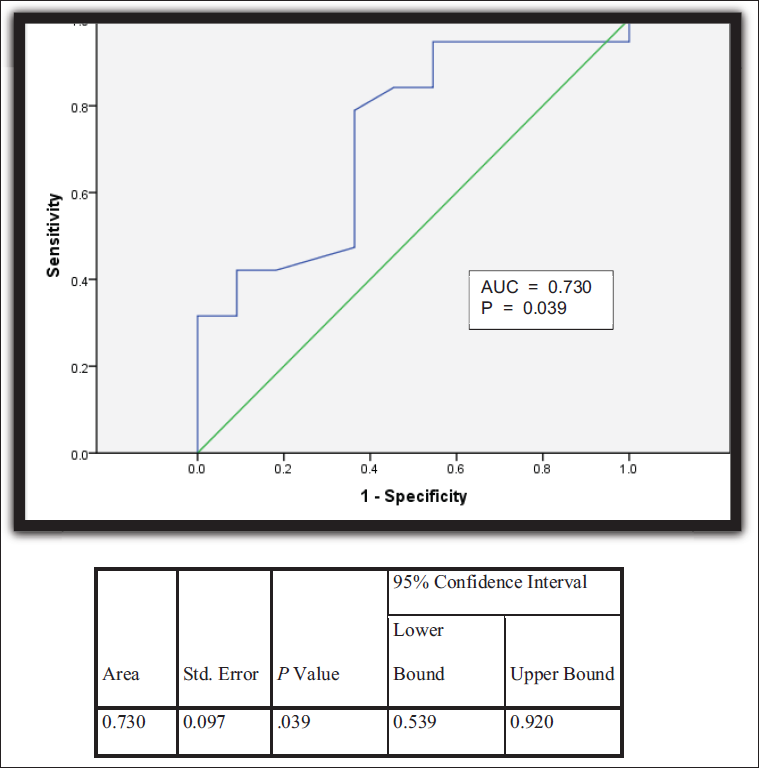
The mean vWF Ag levels were higher in patients with mGS scores ≥ 151 than those with mGS scores ≤ 100 (250% ± 39.79% vs. 155.78% ± 35.02%; P < .001). Patients with triple-vessel disease had higher vWF Ag levels than those with single-vessel disease (266.38% vs. 179.82%; P < .001). A correlation coefficient value of 0.670 was noted between vWF Ag levels and mGS (P < .001), indicating a strong correlation between the 2 (Figure 1). The ROC curve was plotted between vWF Ag levels and coronary angiogram report to predict more than 1 vessel’s involvement in CAG. The area under curve value was 0.739 with the 95% confidence interval (0.54-0.92), suggesting that higher vWF Ag levels predicted more than 1 vessel’s involvement (Figure 2).
Receiver Operating Characteristic Curve (ROC) Showing Relation Between vWF Ag Levels in Predicting More than One Vessel Involved.
Discussion
This particular study, involving 30 patients with STEMI, indicated that as the severity of CAD worsened, the levels of vWF Ag increased. vWF is a glycoprotein that plays an important role in primary hemostasis by adhering platelets to the subendothelial collagen and stabilizing factor VIII of the intrinsic coagulation cascade. It is present in plasma, the subendothelial matrix, the endothelial cells, and platelet granules. 13 The severity of inflammation determines the balance of vWF and ADAMTS13 activity. In hypercoagulable states (sepsis, COVID-19), vWF is excessively released, surpassing the counterbalancing activity of ADAMTS13. 14
High concentrations of vWF in the blood are linked to well-known cardiovascular risk factors, such as advanced age, smoking, high cholesterol levels, diabetes mellitus, and hypertension. Moreover, elevated levels of vWF can predict the occurrence of stroke and vascular events in individuals with atrial fibrillation. 15 vWF has also been linked to insulin resistance and type 2 diabetes mellitus. Insulin resistance is linked to impaired endothelial function. These data indicate that vWF may pose a danger for cardiovascular disease (CVD), specifically in people with type 2 diabetes mellitus or insulin resistance. 16
The link between higher vWF and an increased risk of CVD was shown to be mitigated by insulin resistance and diabetes mellitus, suggesting that these conditions are possible mediators. Higher levels of vWF have been linked to an increased chance of developing type 2 diabetes mellitus. Moreover, vWF has been linked to insulin resistance in individuals both with and without diabetes mellitus. Consequently, those with increased levels of vWF have a higher likelihood of having insulin resistance and acquiring diabetes mellitus, which could increase their risk of developing CVD. 17
In a study by Hiroyuki Sakai and colleagues, the plasma concentration of vWF was elevated in individuals with AMI, possibly due to the hemodynamic alterations caused by the onset of myocardial infarction. 6
Another study conducted by Kato et al 18 showed that elevated levels of vWF were correlated with an increased amount of coronary plaque in patients with CAD who were undergoing statin medication. This indicates that a high vWF level may serve as an indicator of the remaining cardiovascular risk even after statin therapy.
A comprehensive study and meta-analysis conducted by Mengge Fan and colleagues 19 found that plasma vWF levels in patients with CAD assessed 24 and 48 hours after admission might potentially serve as a standalone predictive indicator for major adverse cardiovascular events. In our study, we found that individuals with higher MGS and those with more arteries implicated in CAG had considerably higher plasma vWF Ag levels.
The mean vWF Ag levels were 204.17% + 51.99%, and the mean MGS was 138.67 + 51.02. Our study’s mean age of presentation, sex distribution, risk factor profile, and mean vWF Ag levels were comparable with those of Bin Yan et al. 20
In our study, there was no statistically significant association between vWF Ag levels among different age groups. However, Bin Yan et al’s study 20 showed that the vWF Ag is highest among older people, which is statistically significant (P = .001). In our study, patients with hypertension, diabetes mellitus, dyslipidemia, and vWF Ag levels were higher but not statistically significant. In Bin Yan et al, 20 patients with hypertension had low levels of vWF Ag in comparison to non-hypertensive patients. The high shear stress and change in blood flow in hypertension can make vWF more vulnerable to sites being cleaved by ADAMTS.(13, 21-22)
There is a scope for research on the possible role of vWF Ag in developing acute MI. To the best of our knowledge, this is the first study to investigate the correlation between vWF Ag levels and the extent of coronary artery involvement in Indian patients with ACS.
Limitations
The study was limited by a small sample size owing to financial constraints, which meant that trends in vWF Ag levels could not be fully measured.
Conclusion
This study has shown that higher levels of vWF Ag in people with STEMI are directly linked with a greater extent of CAD. However, more extensive population studies are needed to confirm whether it is an effective predictor of severe CAD.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study has been approved by Institutional Ethical Committee.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent has been taken from all the participants enrolled.