
Abstract
Von Willebrand disease (VWD) is often diagnosed as a consequence of symptoms experienced with hemostatic stressors, such as menstruation and childbirth. Thus, patients seeking medical care for VWD are generally younger. As a result, the natural course of VWD in older adults has not been well described. A retrospective electronic health record review was performed to provide a descriptive analysis of older VWD patients with at least one clinic visit at the Hemophilia Center of Western Pennsylvania (HCWP) between June 1, 2015, and May 31, 2021, and age 45 or older at the time of the visit. Data collected included VWD-related information, multimorbidity, and medications. Age-related change in von Willebrand factor (VWF) levels and the influence of multimorbidity on VWF levels were assessed. Seventy patients had 131 HCWP clinic visits. Hypertension, 34.3%, and osteoarthritis, 32.3%, were the most common multimorbidity-associated conditions. More than 33% of patients were receiving at least one antihemostatic medication. The most common bleeding symptom was ecchymosis, 22.9%. VWF antigen levels, 0.76 IU/mL, and the proportion of patients with normal VWF levels, 54.5%, increased with age to 0.99 IU/mL, p < 0.001, and 78.8%, p < 0.001, respectively. Multimorbidity did not predict change in VWF levels, p = 0.84. Of 62 invasive procedures performed, bleeding occurred in one of nine where VWD-specific therapy was omitted. These findings underscore the importance of describing the natural course of VWD in older adults, especially the critical nature of determining bleeding risk to guide clinical decision-making with the use of antihemostatic drugs and periprocedural VWD-specific therapy.
Background
Von Willebrand disease (VWD) is a heterogeneous disorder caused by a deficiency or defect in von Willebrand factor (VWF). 1 A disorder of primary hemostasis, VWD primarily manifests as mucocutaneous bleeding, such as ecchymosis, epistaxis, and menorrhagia, as well as bleeding following hemostatic stressors, such as surgery, childbirth, and trauma. 2 VWD is the most common inherited bleeding disorder with 1% of the population affected and 0.1% symptomatic. 3 VWD is more commonly diagnosed in women, likely due to symptoms experienced with gender-specific hemostatic stressors, such as menstruation and childbirth. 4 As a consequence, patients seeking medical care for VWD are generally younger. A survey conducted of nine hemophilia treatment centers in the United States found that over a 3-year period between 2013 and 2015 almost two-thirds of clinic visits in adult patients with VWD occurred in individuals less than 45 years of age. 5 The reasons older adults less commonly pursue medical care for VWD are unclear. Certainly, the cessation of menstruation and childbirth with menopause may be one reason; however, an increased need for age-related invasive procedures, such as screening colonoscopy and arthroplasty, and concomitant periprocedural VWD-specific therapy to prevent bleeding, should still demand VWD-related care. Another reason may be an amelioration of bleeding symptoms with aging. It is well established that VWF levels increase with age among healthy adults.6–8 Recently, there is emerging research demonstrating this occurs in patients with VWD, in particular mild type 1, too.9–11 It is unclear if rising VWF levels alter bleeding phenotype, but if so, this may explain why older patients less commonly seek VWD-related care.12–15
Because most patients seeking medical care for VWD are younger, the natural course of VWD in older adults has not been well-described. 16 This is critical for many reasons. As previously mentioned, VWF levels increase with age in VWD, yet it is uncertain if this results in lessened bleeding. If so, VWD-specific therapy, routinely administered in conjunction with invasive procedures, may increase thrombosis risk, especially among those with cardiovascular disease (CVD) and related risk factors. Patients with VWD may be afforded some protection against CVD events, such as myocardial infarction (MI) and stroke, but not atherosclerotic CVD.17, 18 CVD, and related disorders, such as atrial fibrillation, often necessitate antiplatelet therapy or systemic anticoagulation; however, the best practice for these agents, and associated treatments, such as percutaneous coronary intervention, is not known. 19 Whether or not VWD affects the prevalence of other common diseases with age, such as hypertension and chronic kidney disease, and how these comorbidities affect VWF levels and overall bleeding risk is unclear, too. Because of this, a descriptive analysis of the older VWD patient cohort at the Hemophilia Center of Western Pennsylvania (HCWP) was performed.
Methods
A retrospective electronic health record (EHR) review of VWD patients with at least one clinic visit at HCWP between June 1, 2015, and May 31, 2021, and 45 years of age or older at the time of the visit was performed. VWD diagnosis was made by an HCWP affiliated physician with expertise in disorders of hemostasis and based on clinical symptoms consistent with a bleeding disorder and a previous von Willebrand factor antigen level (VWF:Ag) and/or von Willebrand factor ristocetin cofactor activity (VWF:RCo) less than 0.50 IU/mL, according to EHR documentation. Patients with a concomitant hereditary bleeding disorder were excluded. Data collected consisted of the following: demographics; number of clinic visits; VWD type; VWF levels; bleeding symptoms; invasive procedures performed, including periprocedural VWD-specific therapy administered and hemostatic complications; medical conditions; and medications.
Demographics consisted of age at the time of clinic visit, sex, race, and ethnicity. For patients with more than one clinic visit, age was determined as the average age of all clinic visits. VWD type was based on EHR documentation. VWF levels consisted of VWF:Ag level, VWF:RCo activity, and factor VIII activity (FVIII). VWF levels recorded consisted of the baseline (oldest) and current (latest) values documented in the EHR. Normal VWF levels were defined as VWF:Ag level and VWF:RCo activity greater than or equal to 0.50 IU/mL. Age-related to VWF levels was defined as the age when VWF levels were checked. Only patients with type 1 VWD and VWF levels checked on more than one occasion and at least one year apart had VWF levels recorded. VWF levels were checked during office visits. Bleeding symptoms were recorded as documented in the office note for each clinic visit. Invasive procedures were defined as those performed at age 45 or older and included periprocedural VWD-specific therapy administration, DDAVP, VWF concentrates, or antifibrinolytics, and hemostatic complications, bleeding or thrombosis. Bleeding was defined as any bleeding deemed abnormal at the time of the procedure or during the first week following the procedure, per EHR documentation. Thrombosis was defined any as any thrombotic event during the first 3 months following the procedure, per EHR documentation. Medical conditions consisted of multimorbidity-associated conditions, deep vein thrombosis, and iron deficiency anemia. Multimorbidity was defined as two or more of the core set of 20 chronic conditions listed as selected by the United States Department of Health and Human Services because they meet the definition of chronicity, are prevalent, and are amenable to intervention. 20 Medications consisted of antihemostatic drugs – aspirin, systemic anticoagulants, fish oil, non-steroidal antiinflammatory drugs (NSAIDs), and selective serotonin reuptake inhibitors/serotonin and norepinephrine reuptake inhibitors (SSRIs/SNRIs). Other drugs collected included iron and estrogen.
Means and standard deviations for continuous variables and frequencies for categorical variables were used to summarize the data. A paired t-test was performed to compare changes in VWF levels, and McNemar's test was used to compare changes in the proportion of patients with normal VWF levels. Multiple linear regression was performed to assess the influence of multimorbidity on change in VWF levels adjusted for VWD type.
The study was approved by the Institutional Review Board at the University of Pittsburgh.
Results
Seventy patients had 131 clinic visits at HCWP with an average of 1.9 (SD 1.3, range 1−9) visits per person. The most common clinic visit type was a return clinic visit, 80.2%. Patient characteristics are presented in Table 1. The average age at each visit was 58.4 years (SD 9.7, range 45−84.5). Most patients were female, 81.4%. Type 1 VWD, 88.6%, was the most common VWD type.
Patient Characteristics.

COPD, chronic obstructive pulmonary disease; DOAC, direct oral anticoagulant; NSAIDs, nonsteroidal antiinflammatory drugs; SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin norepinephrine reuptake inhibitor.
For patients with more than one visit, age was determined as the average age of all clinic visits.
Defined as 2 or more of a core set of 20 chronic conditions as selected by the United States Department of Health and Human Services because they meet the definition of chronicity, are prevalent, and are amenable to intervention.
Multimorbidity was present in 58.6% of patients (Table 1). Hypertension, osteoarthritis, and depression were the most common multimorbidity-associated conditions affecting 34.3%, 32.3%, and 25.7% of patients, respectively. Coronary artery disease was present in six patients, including four with a history of MI, and three patients had a history of ischemic stroke. Two patients had a history of deep vein thrombosis. Multimorbidity did not predict change in VWF levels, β = 0.009 (SE 0.046), p = 0.84. The most common antihemostatic drugs taken by patients were SSRIs/SNRIs, 27.1%, and NSAIDs, 22.9% (Table 1). Four patients were receiving aspirin and one patient was receiving systemic anticoagulation. Thirteen percent of patients were receiving multiple antihemostatic drugs.
The most commonly documented bleeding symptom during office visits was ecchymosis, 22.9% (Table 2). Other commonly reported bleeding symptoms were gastrointestinal bleeding (GIB), 14.5%; epistaxis, 12.2%; and heavy menstrual bleeding, 10.7%. One patient with type 2 VWD receiving VWF concentrate prophylactically to prevent GIB had nine office visits, accounting for 47.3% of reported GIB.
Bleeding Symptoms.

Bleeding symptoms were recorded as documented in the office note for each clinic visit.
One patient with type 2 VWD receiving VWF concentrates prophylactically to prevent gastrointestinal bleeding had nine office visits, accounting for 47.3% of reported gastrointestinal bleeding.
VWF levels were checked on more than one occasion and at least one year apart in 40 patients with type 1 VWD (Table 3). Mean VWF:Ag level, VWF:RCo activity, and FVIII activity increased from 0.76 (SD 0.3) to 0.99 (SD 0.32), p < 0.001; 0.59 (SD 0.30) to 0.73 (SD 0.37), p = 0.02; and 0.84 (SD 0.33) to 1.09 (SD 0.37), p < 0.001, IU/mL, respectively, between the baseline (oldest) and current (latest) values. The proportion of patients with normal VWF levels increased from 54.5% to 78.8%, p < 0.001. The average age was 52.3 (SD 10.7) years at the time of the baseline (oldest) values and 59.2 (SD 9.6) years at the time of the current (latest) values, p < 0.001.
Change in von Willebrand Factor Levels.

VWF:Ag, von Willebrand factor antigen; VWF:RCo, von Willebrand factor ristocetin cofactor activity. FVIII, factor VIII.
VWF levels recorded consisted of the baseline (oldest) and current (latest) values documented in the electronic health record. Only patients with type 1 VWD and VWF levels checked on more than one occasion and at least 1 year apart were included.
Normal VWF levels were defined as VWF:Ag level and VWF:RCo activity greater than or equal to 0.50 IU/mL.
Age related to VWF levels was defined as the age when VWF levels were checked.
Thirty-six patients had 62 invasive procedures performed (Table 4). The most common invasive procedures were dental extraction, 11; colonoscopy, 10; and arthroplasty, 7. VWD-specific therapy was not given with nine procedures. The decision to omit VWD-specific therapy at HCWP is at the discretion of the HCWP physician and is based on the presence of normal VWF levels, bleeding phenotype, and the type of invasive procedure being performed (Table 5). DDAVP and VWF concentrates were administered with 22 and 31 procedures, respectively. No antifibrinolytics were given. Two procedures were complicated by bleeding, a colonoscopy requiring removal of two 10 mm polyps with GIB despite periprocedural DDAVP, and a spine surgery with wound bleeding in the absence of any VWD-specific therapy.
Invasive Procedures.

EGD, esophagogastroduodenoscopy.
Invasive procedures listed include only those performed more than once.
Invasive procedure details, such as the need for biopsy or polypectomy, were not available in the electronic health record.
Invasive Procedures Without von Willebrand Disease Specific Therapy.
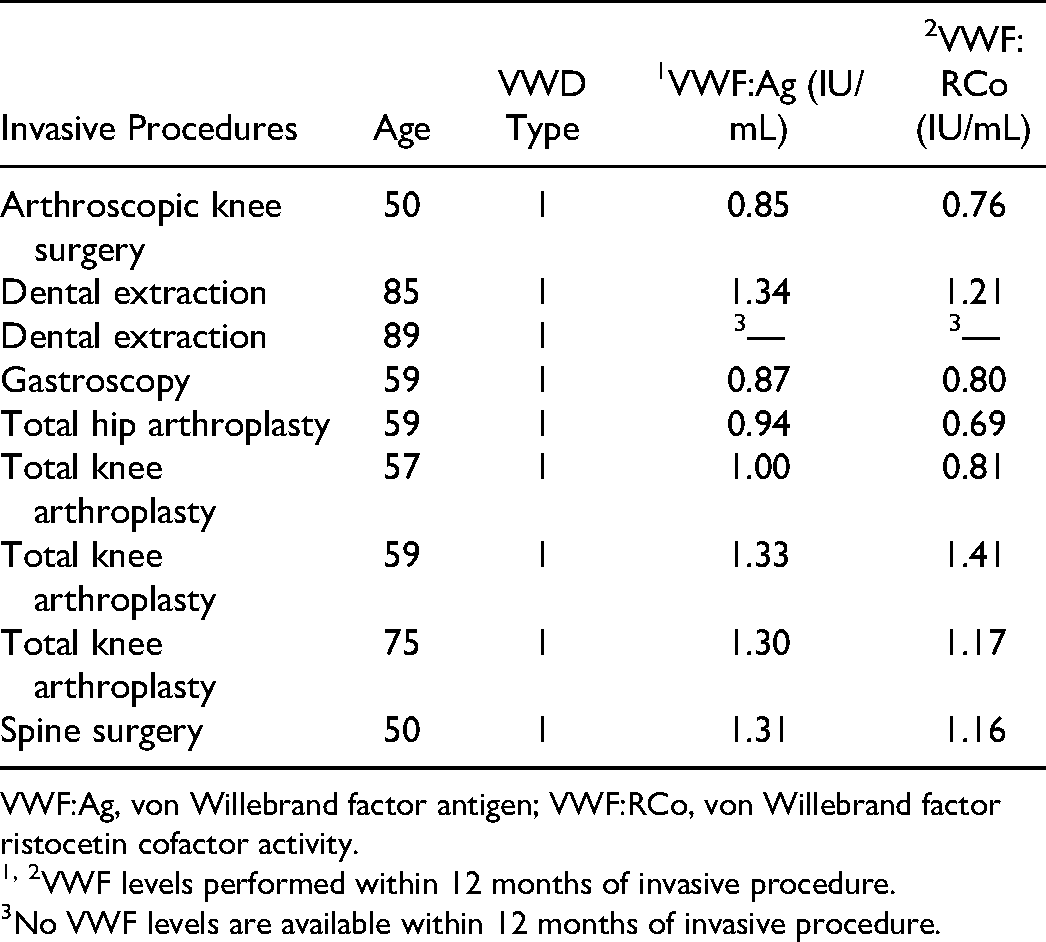
VWF:Ag, von Willebrand factor antigen; VWF:RCo, von Willebrand factor ristocetin cofactor activity.
1, 2VWF levels performed within 12 months of invasive procedure.
No VWF levels are available within 12 months of invasive procedure.
Discussion
This retrospective EHR review describes the clinical characteristics of older patients with VWD. Between June 1, 2015, and May 31, 2021, 70 patients 45 years of age or older had 131 clinic visits at HCWP. Four patients had a history of MI, and three patients had a history of stroke. Likely as a result of this, and other multimorbid-associated conditions, such as osteoarthritis, affecting 33% of patients, more than a third of patients were receiving at least one antihemostatic medication.
In patients with type 1 VWD, mean VWF:Ag levels increased with age from 0.76 IU/mL at baseline (oldest), average age 52.3 years, to 0.99 IU/mL at current (latest), average age 59.2 years, p < 0.001, and VWF levels at current (latest) were normal in 78.8% of patients. These data are consistent with previously published findings, which have demonstrated an age-related increase in VWF levels in patients with VWD, in particular mild type 1 VWD. A retrospective cohort study among 31 patients with type 1 VWD (historically lowest VWF:Ag level or VWF:RCo activity <0.50 IU/mL) reported VWF:Ag levels and VWF:RCo activity increased 0.30 and 0.20 IU/mL, respectively, per decade. 9 Further, 58% of patients experienced normalization (greater than 0.50 IU/mL) of VWF:Ag levels and VWF:RCo activity. At last follow up, the mean VWF:Ag level and VWF:RCo activity were 0.71 and 0.56 IU/mL compared with baseline values of 0.44 and 0.34 IU/mL (p < 0.001 and p < 0.001, respectively). Others have reported similar findings.10, 11
The reasons underlying an increase in VWF levels with age in VWD is not entirely clear. Atiq et al found an association between comorbidities and VWF:Ag levels and hypothesized comorbid illnesses, such as hypertension, diabetes mellitus, and malignancy, may explain the age-related increase in VWF levels. 21 He found VWF:Ag levels increased from 0.36 IU/mL (95% CI, 0.23 to 0.49) in patients without comorbidities to 0.44 IU/mL (95% CI, 0.29 to 0.62) in patients with one comorbidity to 0.67 IU/mL (95% CI, 0.39 to 0.90) in patients with two comorbidities. In contrast, multimorbidity did not predict change in VWF levels, β = 0.009 (SE 0.046), p = 0.84, in this study. The disparate findings may be related to differences in the comorbidities assessed by Atiq et al., and the multimorbidity related illnesses assessed herein. Additionally, the limited sample size in this study may have precluded the ability to detect such a change. More than half of the patients, 58.6%, met the definition of multimorbidity. Osteoarthritis, 32.3%, and depression, 25.7%, were more common than seen in the general population. The high prevalence of osteoarthritis may be due to undetected hemarthrosis in VWD when younger; whereas, it is not clear why the prevalence of depression was so high. A protective effect of VWD and VWF deficiency against CVD events despite atherosclerosis using the Nation Inpatient Sample and Atherosclerosis Risk in Communities databases, respectively, has been previously reported; yet, 10% of patients in this cohort had a history of MI or stroke, which may indicate this protective effect disappears with normalization of VWF levels.17, 18
Whether or not an age-related increase in VWF levels results in amelioration of bleeding phenotype is uncertain. In this cohort, bleeding symptoms were recorded as documented in the office note for each clinic visit; however, the retrospective nature of the study and review of the office note to determine bleeding symptoms precludes the ability to determine an accurate bleeding score and systematically conclude if bleeding phenotype changes with age. Prospective studies with longitudinal bleeding assessments, recently investigated by Lavin et al, are necessary to answer this important question, especially as it relates to the need for VWD-specific therapy with invasive procedures or concomitant antihemostatic therapy.22 If VWF levels normalize with age and bleeding risk is mitigated, particularly in older patients with CVD related risk factors, VWD-specific therapy could potentiate thrombotic risk. Alternatively, the use of antihemostatic agents, such as aspirin, may pose no significant bleeding risk. Further, VWF concentrates are expensive. Unnecessary use is a waste of healthcare dollars.
This study has a few limitations that warrant consideration. This is a retrospective EHR review; thus, it is subject to the inherent limitations of such studies, in particular selection bias. Study participants are limited to patients with at least one clinic visit. Further, analyses of change in VWF levels over time are restricted to patients with multiple clinic visits. These patient populations may not be an accurate reflection of the entire VWD population and may represent a healthier cohort (ie, more likely to seek healthcare due to health consciousness), or alternatively, a less healthy cohort (ie, more likely to see healthcare due to worse health). Another limitation of this study lies with the potential for fluctuation in VWF levels, which are subject to influence by many external factors, such as infection, surgery, and estrogen, that may cause a transient increase; however, VWF levels were checked during office visits, which is a setting more likely to provide an accurate reflection. Only three patients were receiving exogenous estrogen therapy. Further, it is important to note that baseline VWF levels are the oldest VWF levels documented in the EHR. Baseline VWF levels are not the historically lowest VWF levels, many of which were checked more than 20 years ago or elsewhere and are not readily available in the EHR.
In conclusion, these findings underscore the importance of describing the natural course of VWD in older adults, especially the critical nature of determining current bleeding risk in this population, so as to guide clinical decision-making when such patients require antihemostatic drugs or invasive procedures that necessitate VWD-specific therapy.
Footnotes
Authors’ Contributions
CDS designed and performed the research, completed the statistical analysis, formulated the conclusions, and wrote the paper.
Declaration of Interests
CDS has acted as a paid consultant for Genentech, Hema Biologics, Novo Nordisk, and Takeda Pharmaceuticals.
Data Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute, (grant number 5K23HL148762).