
Abstract
Percutaneous coronary intervention (PCI) is one of the most commonly performed cardiovascular interventions to treat significant coronary artery stenosis. Although a safe procedure, it carries the risk of complications like coronary artery perforation (CAP), bleeding, stroke, and acute kidney injury rarely resulting in death. The incidence of CAP is 0.84% of all PCI procedures and the incidence is increasing as cardiologists are accepting more and more challenging cases. CAP is caused by a guidewire (GW) or a vessel tear from balloon angioplasty, stenting, or rotational atherectomy. Though the majority of CAPs do not result in cardiac tamponade, some do lead to tamponade and death. The majority of distal wire perforations respond to prolonged balloon inflation, coils, glue, or fat embolization. Herein, we report a case of distal CAP in a 63-year-old woman occurring following left circumflex artery PCI caused by the exiting of coronary GW. The CAP was successfully sealed by the liquid embolization technique using ONYX. First described in 1990, Onyx is an elastic polymer composed of ethylene vinyl alcohol copolymer dissolved in dimethyl sulfoxide and mixed with micronized tantalum powder (Onyx). The Onyx is predominantly used by interventional radiologists while performing neurovascular and peripheral vascular interventions. There were only a few case reports of plugging of CAPs using Onyx. Our case highlights the safety and feasibility of closing distal CAPs using Onyx.
Keywords
Introduction
Percutaneous coronary intervention (PCI) is one of the most commonly performed cardiovascular interventions to treat significant coronary artery stenosis. Although a safe procedure, it carries the risk of complications like coronary artery perforation (CAP), bleeding, stroke, and acute kidney injury rarely resulting in mortality. CAP is one of the dreaded complications encountered during PCI. Incidence of CAP is around 0.84% which may result in cardiac tamponade and death in some if not identified and managed promptly.1–4 Distal coronary perforations are routinely managed by prolonged balloon inflation proximal to perforation, collagen, glue, and coils. There are only a few case reports of managing distal coronary perforations with liquid embolic agents, especially Onyx. First described in 1990, Onyx is an elastic polymer composed of ethylene vinyl alcohol copolymer dissolved in dimethyl sulfoxide (DMSO) and mixed with micronized tantalum powder (Onyx). The Onyx is more often used by interventional radiologists during neurovascular and peripheral interventions. There were only a few case reports of the closure of CAPs using Onyx. The same technique was adopted to rescue our patient from this catastrophic complication. We present a case of left circumflex artery (LCX) perforation during PCI resulting in cardiac tamponade managed by the liquid embolic agent, Onyx. This case highlights not only the safety and feasibility of Onyx but also the importance of having an interventional radiologist in the team especially while managing complex situations arising out of cardiac interventions.
Case Report
A 63-year-old woman with no known co-morbidities presented with recurrent angina pectoris of three-month duration to a peripheral cardiac center. Coronary angiography demonstrated significant stenosis involving the left anterior descending artery (LAD) and LCX. The patient was advised to undergo PCI to LAD and LCX. During PCI, a 6F guiding catheter (EBU 3.0, Medtronic Inc., USA) and a 0.014-inch guidewire (GW) (Run-through guidewire, TERUMO) were used. A 3.0 mm × 36 mm ABLUMINUS stent (Concept Medical, USA) was deployed in the LCX. The LAD vessel was similarly stented with a 3.0–16 ABLUMINUS stent. Following the intervention, the patient developed sudden hypotension and dyspnea on the same day. Two-dimensional echocardiography was done on the same day which revealed evidence of pericardial effusion and signs of cardiac tamponade. Pericardiocentesis was initiated immediately with the help of a pig-tail catheter. Pericardiocentesis was done for consecutive four days. Check coronary angiogram on the fourth post-procedural day also failed to demonstrate the exact site of perforation. The patient developed acute kidney injury and dialysis was done on the same day. The patient was then intubated and put on mechanical ventilation. Inotropes were started.
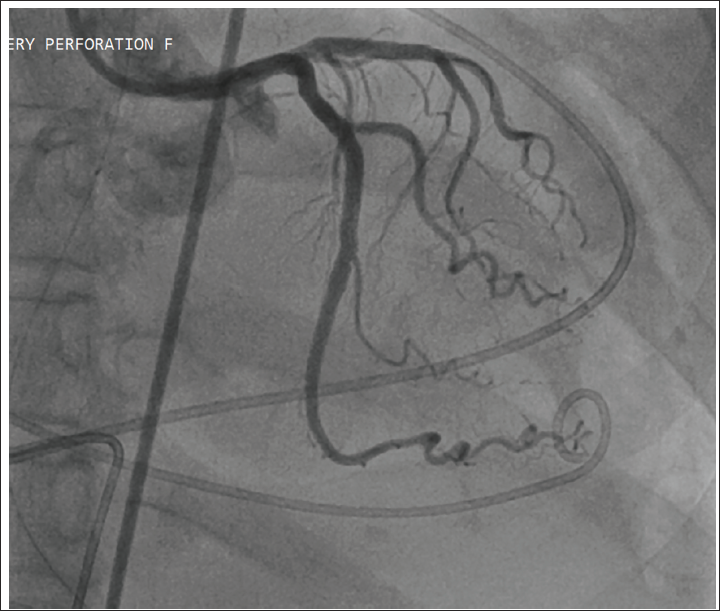
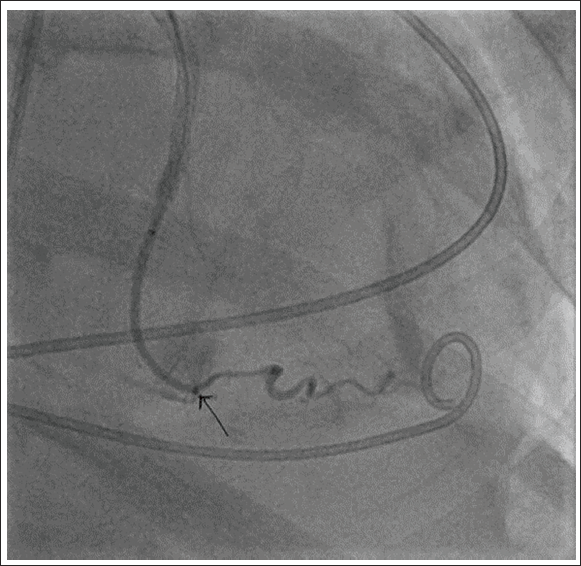
The patient was referred to our center for further management, four days after the stent placement, as she developed sepsis and multiorgan dysfunction. Three days after stabilization, coronary angiography was repeated in view of persistent pericardial effusion and cardiac tamponade, which again failed to demonstrate the site of coronary perforation (Figure 1). However, selective contrast injection into the obtuse marginal branch using a microcatheter demonstrated contrast extravasation (Figure 2). Considering the diameter and area of supply of the vessel, we thought coil embolization was not an ideal choice. Though N-butyl cyanoacrylate glue was a choice, however, given its adhesive properties with an associated risk of catheter retention, it was not considered. Thus, the liquid embolic agent, Onyx, was favored after consulting an interventional radiologist, for its precision and lack of adhesive nature.
The Initial Images with Standard-sized Wire Did Not Reveal Perforation Site During Coronary Angiography.
Coronary Angiography Using Microcatheter Revealed the Leakage Site in the Distal LCX–Obtuse Marginal Vessel (Arrow Showing the Leakage Site).
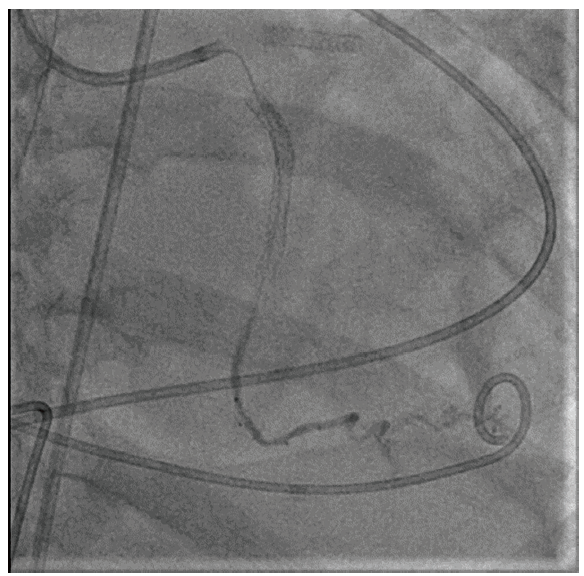
Microcatheter (1.7F Echelon-10 [Medtronic, USA]) was placed at the point of perforation using 0.14″ GW (Traxcess guidewire [Microvention. Inc]). Once the microcatheter tip was in the desired position, the injection of Onyx 18 was carried out as follows: (a) 0.25 mL of DMSO was injected into the microcatheter to fill the dead space; (b) Onyx was aspirated into a 1-mL syringe, and 0.25 mL of this amount was injected slowly for 40 seconds to fill the microcatheter and replace the DMSO in the dead space under fluoroscopy. About 0.6 mL of Onyx 18 was injected intermittently under subtracted fluoroscopy. A repeat coronary angiogram revealed a patent Obtuse marginal artery with cessation of contrast extravasation (Figure 3). The perforation site was closed and the patency of the vessel was maintained. On the second post-procedural day, a pigtail catheter was collected from the pericardial sac and echocardiography showed a small effusion. After recovery from multiorgan failure, the patient was discharged and on subsequent follow-up, she was in good physical condition. Subsequent recovery was uneventful.
Angiogram after Closure of Coronary Artery Perforation Using ONYX- No Leakage at Perforation Site.
Discussion
Perforation or frank rupture of the coronary artery due to coronary GWs especially with hydrophilic wires, atherectomy devices, or high-pressure balloons, occurs in 0.84% of patients undergoing PCIs.1–4 The frequency of CAP is increasing because interventional cardiologists are accepting more and more challenging cases including chronic total occlusions (CTOs) and severely calcified lesions. Though CAP is considered a cath lab nightmare yet majority of distal perforations do not lead to cardiac tamponade. However, CAP warrants prompt diagnosis and management as it can lead to death. The degree of perforation varies from barely perceptible to severe and a classification scheme based upon the angiographic appearance of the perforation has been proposed—Elli’s modified classification 4 :
Class I—Extra-luminal crater without extravasation
Class II—Pericardial or myocardial blushing (staining)
Class III—Perforation ≥1 mm in diameter with contrast streaming into the pericardium
Class IV—Perforation into a chamber like the left ventricle or coronary sinus or any other chamber except the pericardium
Though the majority of operators follow Elli’s classification for grading of perforation, however, this classification does not take into account perforations of collaterals during CTO interventions. Coronary perforations are ideally classified according to location, as location has important implications regarding management. There are three main perforation locations: (a) main vessel, (b) distal coronary wire perforations, and (c) collateral vessel, either septal or epicardial. Our case represents Class II perforation. The management of CAP depends on its severity as per Elli’s classification. Type I and some type II perforations usually require close observation with no active treatment as they are usually well tolerated. However, some of the type II perforations can lead to cardiac tamponade due to persistent leaks from the perforation site as in our case. Prolonged balloon inflation proximal to the site of perforation or occlusion by the deployment of coils, glue, or fat embolization is successful in occluding the perforation in the majority of cases.5–7 However, we felt our patient needed a different approach as it is a distal GW perforation of a small diameter branch vessel. We were successful in sealing the perforation by using Onyx. When the Onyx comes in contact with blood, the DMSO diffuses away, leaving polymer precipitating within the vessel lumen, without adherence to the vessel wall. The non-adhesive nature of Onyx provides more precise targeted embolization without an added risk of catheter retention.7, 8 Usage of the microcatheter over microwire helped in the distal navigation across the tortuous cardiac vessel and stent in our case. Contrast injection through a neurovascular microcatheter helped us in locating the exact site of perforation.
Conclusion
CAP during PCI is an infrequent complication. Morbidity and mortality depend on the type and site of perforation. Identification and prompt treatment can tide over the crisis in the majority of cases. There are many ways by which perforations can be managed. However, some cases need out-of-the-box thinking as well as the hardware used by other interventional specialists like interventional radiologists. By adopting such a philosophy we could successfully seal a distal perforation site by using Onyx. Therefore, the liquid embolization technique is a safe and feasible option in some cases of distal coronary artery wire perforations.
Learning Points
Management of complications associated with PCIs sometimes needs out-of-the-box thinking. Taking help from an interventional radiologist sometimes saves the day.
Sealing of distal CAP can be done safely with the use of Onyx.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval was obtained from the Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The written informed consent was taken from the patient’s relative.