
Abstract
This case report delineates the complex management of a 65-year-old female with established diabetes, hypertension, and ischemic heart disease, who presented with refractory angina despite comprehensive medical management. Coronary angiography identified significant pathology in the right coronary artery alongside a previously placed, functioning stent in the left anterior descending artery. The intervention was complicated by the occurrence of a type B coronary artery dissection and a type III coronary perforation during an attempt to extract a stent. Immediate remedial measures, including balloon inflation and the placement of drug-eluting stents, were undertaken. The patient underwent a transient episode of collapse, from which she was successfully resuscitated. The concluding angiographic assessment confirmed the effective dilation of the lesion with no remaining dissection or perforation. This case accentuates the infrequent yet critical complications that can arise during percutaneous coronary intervention.
Keywords
Introduction
+++Coronary heart disease (CHD) is a prevalent and impactful condition, particularly among the elderly. In 2020, cardiovascular diseases were the leading cause of death in the United States, accounting for 928,741 fatalities. 1 Notably, a significant portion of these deaths occurred in individuals over the age of 35, primarily in developed countries. 2 The introduction of percutaneous coronary intervention (PCI) with stenting has been a revolutionary advancement in the treatment of CHD, leading to marked reductions in morbidity and mortality. 3
Stents, which are expandable wire mesh coils, are inserted into newly opened arteries to maintain patency and prevent restenosis. Vascular tissue eventually covers the stent, forming a protective layer. 4 This process typically completes within 3–12 months, depending on whether the stent is drug-coated. 5 Drug-Eluting Stents release medication to slow down tissue growth and prevent the re-narrowing of blood vessels, whereas Bare Metal Stents do not have this drug coating. 6
This case report details the management of CHD in a 65-year-old female patient with a history of diabetes, hypertension (HTN), and ischemic heart disease, who underwent PCI with stenting for symptomatic angina. The case underscores the challenges encountered, including coronary artery dissection (CICAD) and perforation, and the interventional strategies employed to address these complications.
Case presentation
A 65-year-old female patient with a medical history of diabetes mellitus, HTN, and ischemic heart disease presented with persistent class III angina despite maximal medical therapy. She had previously undergone PCI in the left anterior descending (LAD) artery 8 years prior. Over 3 days, she experienced resting chest discomfort with accompanying ST-T wave changes on the electrocardiogram (ECG) (Figure 1). Troponin assays were negative. An echocardiogram showed an ejection fraction of 40% and hypokinesis of the inferior wall, septum, and apex. Given her high-risk profile and ongoing symptomatic angina at rest, coronary angiography was indicated and performed via the right femoral artery approach.

Electrocardiogram (ECG) of the patient showing ST-T changes. The figure illustrates the ECG of the patient, revealing significant ST-T changes. These changes are indicative of myocardial ischemia and provide important diagnostic information regarding the patient’s cardiac condition.
The angiogram revealed a patent LAD stent and a normal circumflex artery. However, significant disease was noted in the proximal to mid segments of the right coronary artery (RCA) (Figure 2). Interventional treatment was initiated to address the RCA lesion. A Judkins right guide catheter was used to engage the coronary system, and a run-through wire successfully crossed the lesion. Predilation was performed with a 2.0 × 15 mm semi-compliant balloon. Subsequently, a 3.0 × 40 mm intracoronary drug-eluting stent (iDES) was advanced but could not traverse the lesion. The stent was retracted, and further predilation was attempted with 2.0 mm semi-compliant balloons to facilitate stent delivery.

Coronary angiogram of the right coronary artery (RCA). This figure showcases the coronary angiogram of the patient’s RCA. The angiogram reveals a severely diseased segment of the RCA, highlighting the need for intervention. The figure provides a visual representation of the anatomical features and extent of the disease in the RCA, aiding in the decision-making process for further treatment strategies.
During stent retraction, deformation of the proximal stent segment occurred, preventing its retrieval into the guide catheter. The entire assembly, including the stent, guidewire, and guide catheter, was carefully withdrawn into the descending aorta and common femoral artery. The stent disengaged from the balloon during this process, leaving the stent within the vessel while the balloon exited the sheath. The proximal stent struts remained outside the sheath, allowing for successful retrieval.
A covered stent was not utilized for the coronary perforation due to the potential risk of side-branch occlusion in this particular anatomical setting. The decision was made to use a standard iDES, which provided adequate sealing of the perforation without compromising the vessel’s integrity.
The guide catheter was repositioned, and the lesion was crossed again with the same coronary wire. Additional predilation was performed, but subsequent contrast injection revealed a type B CICAD (Figure 3) and a type III coronary perforation (Figure 4). Immediate measures included balloon inflation at the perforation site for 3 min. Echocardiographic assessment showed a mild pericardial effusion without evidence of tamponade. Despite these interventions, the patient experienced a sudden collapse.

Type B coronary artery dissection (CICAD). This figure presents a visual recording of a type B CICAD during the percutaneous intervention. The figure clearly depicts the presence of parallel tracts or multiple lumens separated by a radiolucent area following contrast injection. This type of dissection indicates a significant tear or break in the coronary artery wall, posing a serious risk to the patient’s cardiovascular health.
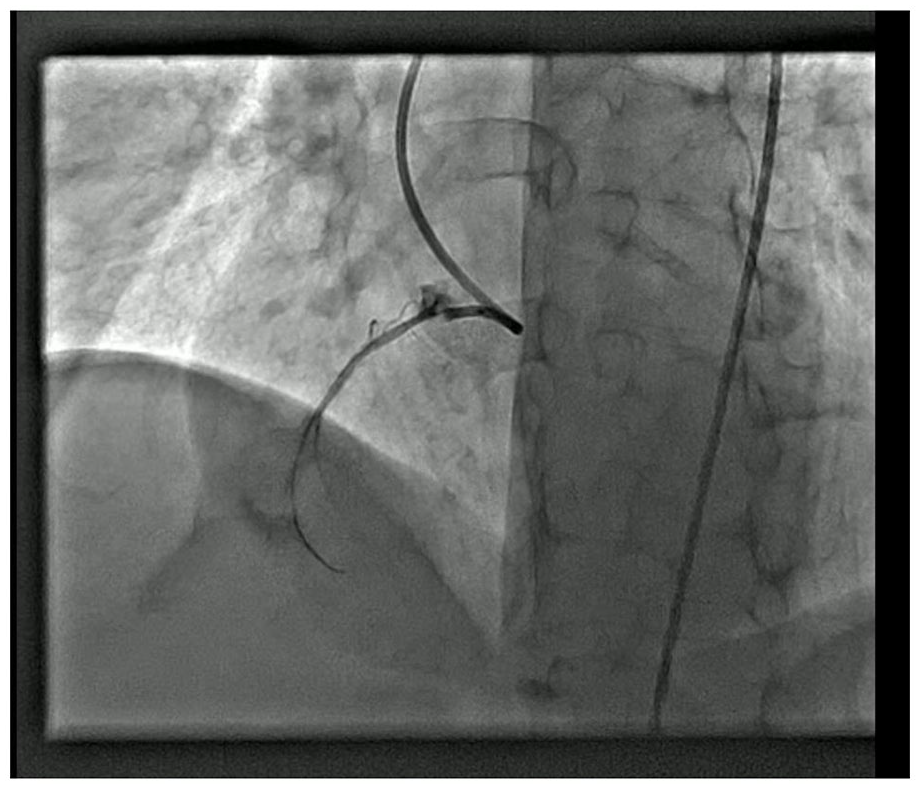
Type III coronary artery perforation (CAP). This figure captures the occurrence of a type III CAP during the percutaneous intervention. The figure provides a clear visualization of the extravasation of contrast medium into the surrounding spaces, such as the coronary sinus or the heart chamber, indicating a severe and potentially life-threatening complication. The figure highlights the urgent nature of addressing the perforation to prevent further complications, such as cardiac tamponade or myocardial infarction.
Cardiopulmonary resuscitation was initiated, and spontaneous circulation returned after one minute. A 3.0 × 24 mm iDES was successfully deployed at the perforation site, sealing the perforation. However, the proximal dissection remained. A second 3.0 × 18 mm iDES was placed proximally, overlapping slightly with the first stent, effectively sealing the dissection. Final angiography confirmed optimal dilation with no residual dissection or perforation (Figure 5). The patient was discharged 2 days later in stable condition.

Successful resolution of coronary complications. This figure showcases the successful resolution of the coronary complications encountered during the percutaneous intervention. After the management of coronary artery dissection and perforation, the figure demonstrates the final angiographic results, revealing good lesion dilation and the absence of residual dissection or perforation. The figure provides a visual confirmation of the successful outcome achieved through prompt and effective interventions. This footage serves a valuable educational resource, demonstrating the importance of timely recognition and appropriate management in overcoming complex coronary complications during percutaneous interventions.
The patient was scheduled for regular follow-up visits to monitor her recovery. During these visits, clinical assessments, ECGs, and echocardiograms were performed to ensure the absence of ischemic symptoms and the stability of cardiac function.
Discussion
This case presentation highlights the challenging course of a patient experiencing uncommon but severe complications during PCI: coronary artery perforation (CAP) and CICAD. These complications can significantly impact patient outcomes, and their prompt recognition and management are crucial for successful intervention.
Coronary artery perforation
CAP is a rare but serious adverse effect of PCI, with an incidence ranging from 0.19% to 1.46% in standard procedures and reaching up to 4.8% in chronic total occlusion cases.1,2 It can lead to life-threatening complications like cardiac tamponade, cardiogenic shock, and myocardial infarction. Studies suggest a fivefold increase in in-hospital mortality associated with CAP, with rates as high as 10%–15%. 2
Ellis classification is a widely used system for categorizing CAP severity based on the location and extent of contrast extravasation. 3 Type I perforations involve minimal leakage, while type II perforations show pericardial or myocardial staining. Type III, as seen in this case, represents extravasation into the coronary sinus or cardiac chambers. 3
A case series from Pakistan reported a 0.12% incidence of CAP among patients undergoing PCI procedures. 4 The LAD was the most frequently affected artery, followed by the circumflex and RCA. Interestingly, guidewires were identified as the cause of perforation in 25% of these cases. 4 The reported complications included fatalities, emergency surgery, and myocardial infarction, highlighting the potential severity of CAP. 4
Management of CAP
Early recognition and prompt intervention are essential for managing CAP. Balloon tamponade at the perforation site is often the first-line therapy to achieve immediate hemostasis, as demonstrated in this case. 5 Stent deployment, covered stents in specific scenarios, and surgical intervention are additional options depending on the severity and location of the perforation. 5
Coronary artery dissection
CICAD is another potential complication of PCI, with an estimated incidence of less than 0.1%. 6 It occurs when a tear or separation forms within the arterial wall, potentially leading to luminal narrowing or blockage. Although most CICAD cases have a favorable prognosis, they can cause reduced blood flow and require stent placement for stabilization. 7
Studies suggest a higher prevalence of CICAD in the RCA compared to the left main artery during coronary angiography. 6 Risk factors for CICAD include catheter manipulation, complex procedures, and patient characteristics like advanced age, diabetes, and pre-existing coronary artery disease, similar to those observed in this case.6,8
CICAD can be categorized into four types based on the angiographic appearance:
Type A: Radiolucent areas within the lumen with minimal contrast staining.
Type B: Parallel channels or multiple lumens separated by a radiolucent area.
Type C: Contrast staining outside the lumen (extraluminal cap).
Type D: Spiral luminal filling defect with prominent contrast staining. 8
The presented case demonstrates a Type B CICAD based on the classification system and described angiographic findings.
Management of CICAD
Balloon angioplasty or stent implantation are the usual approaches to managing CICAD, with success rates exceeding 90% in most cases. 9 However, factors like the severity of dissection and presence of adequate antegrade flow can influence treatment decisions. In rare instances, when percutaneous interventions fail, surgical bypass grafting might be necessary. 9
Conclusion
This case underscores the importance of recognizing and effectively managing complications like CAP and CICAD during PCI. Prompt intervention with balloon tamponade, stent placement, or other techniques plays a vital role in achieving successful outcomes and minimizing patient mortality.
Footnotes
Acknowledgements
The authors are very appreciative to the patient for the opportunity to learn as well as thankful to the hospital for providing support for completing this report.
Author contributions
G.A.S., A.B.B., S.Y., S.R., N.U., M.K. K., S.J.S., N.U.H.Z., and M.N.L. contributed to various aspects of the manuscript. G.A.S., A.B.B., and N.U. were involved in the conception and design of the manuscript. G.A.S., S.Y., S.R., M.K.K., S.J.S., N.U.H.Z., and M.N.L. contributed to data collection and processing. A.B.B., S.Y., and N.U. participated in the interpretation and analysis of the project. S.R., M.K.K., and S.J.S. conducted the literature review and were involved in the writing of the manuscript. G.A.S., S.Y., S.R., N.U., M.K.K., S.J.S., N.U.H.Z., M.N.L. and H.H.S. critically revised the manuscript to ensure its accuracy and quality.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the legally authorized representative of the patient for the publication of this case report.