
Abstract
Background:
The incidence of premature coronary artery disease (PCAD) is on rising trend in low- and middle-income countries. Considering the limited reports, the current study was conducted to evaluate the prevalence, various predisposing factors, and coronary angiographic findings of PCAD in North India.
Methods:
Study design—hospital-based analytical cross-sectional study.
Setting:
Outpatient and inpatient units of a tertiary cardiac center in North India. Two hundred sequential patients (170 males and 30 females) with acute coronary syndrome were evaluated for history of risk factors, measurement of anthropometric parameters, biochemical blood examination, electrocardiogram, complete dental examination, and angiographic assessment of coronary artery lesion. Patients with acute infection or chronic inflammatory disorders were excluded. Patients were divided into PCAD (age ≤45 years) and mature CAD.
Results:
The prevalence of PCAD was 15% (N = 30). PCAD had higher rates of family history of CAD (P < 0.001), tobacco consumption (P = 0.01), smoking (P = 0.004), and single-vessel disease (SVD) (P < 0.001). Premature CAD group had significantly lower mean fasting blood glucose (105 ± 41 mg/dL vs 127 ± 45 mg/dL) levels.
Conclusion:
Family history of CAD, smoking, and tobacco consumption are important risk factors of PCAD. SVD is more common in PCAD. Screening the susceptible population at risk and controlling the cardiovascular risk factors will help reduce the epidemic and consequences of PCAD.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of deaths around the world. Around 17.9 million people died from CVDs in 2019, accounting for 32% of global mortality. Around 85% of these deaths was attributed to heart attack and stroke. Over 75% of CVD associated deaths occur in low- and middle-income countries. 1 Nowadays, these diseases are epidemic in both urban and rural areas due to swift epidemiological changeover, improved life span, standard of living, food habits, stressful life and genetic susceptibility. 2 In India, the death rate was 24% in 2008 due to CVD and it is estimated that in 2030, the death rate may upsurge to 35.9%. 3 At the present time, moreover, it is often faced by young adults. Around 4% to 10% of individuals with CAD present at age less than 45 years.4, 5 Premature coronary artery disease (PCAD) has been defined in literature to commence at an age from 30 to 56 years.4-6 PCAD has been reported to present differently, with different risk factors and coronary angiographic findings in contrast to mature coronary artery disease (MCAD).6, 7 Clinical studies from India have reported the incidence in the young population as 12% to 16%.8, 9 About 52% of CAD-associated deaths and about 25% of acute myocardial infarction in India occur below the age of 50 years and 40 years, respectively.10, 11 Indians are affected with heart diseases 5 to 10 years earlier than other residents.12, 13 This new epidemic is a major concern for India. However, due to vast diversity of population, the results of the epidemiological studies cannot be generalized. Current study evaluated the prevalence, clinical manifestations, associated predisposing factors, and coronary angiographic findings in PCAD compared to MCAD from North Indian population.
Materials and Methods
This is an analytical cross-sectional study which was conducted in the inpatient and outpatient units of a tertiary cardiac facility in northern India. We collected the data of 200 consecutive patients with acute coronary syndrome (ACS), and patient information was anonymized.
Study Population
ACS included diagnosis of unstable angina, non-ST elevation myocardial infarction, and ST elevation myocardial infarction. Standard definition was used for the diagnosis. Patients with recent or ongoing fever/infection, chronic inflammatory disorders, and undiagnosed CAD were excluded. Patients were divided into groups of PCAD (age ≤45 years) and MCAD.
Methods
All patients were subjected to a protocol (as per proforma) which included a detailed clinical history and relevant examination. All patients were subjected to the following baseline investigations: complete blood count, erythrocyte sedimentation rate, fasting blood sugar, serum bilirubin, SGOT, SGPT, urea, creatinine, RA factor, VDRL, LE cell, ANA, HIV, X-ray chest PA view, ECG, and Troponin-T. Anthropometric measurements including weight, height, body mass index (BMI), and waist-hip ratio (WHR) were recorded. BMI >30 kg/m2 was considered as cut-off for obesity. Central obesity was defined as WHR >0.9 for males and >0.8 for females. Fasting blood glucose level ≥126 mg/dL or already undergoing treatment was considered as diabetes mellitus. Blood pressure recording on 2 occasions of 140 mm of Hg systolic or 90 mm of Hg diastolic or already undergoing treatment was considered as hypertensive. History of smoking or tobacco consumption within last 1 year was considered as risk factor. A positive family history of CAD was defined as the presence of CAD in a first-degree relative (male < 55 years and female < 65 years). Dyslipidemia was considered by presence of any 1 of the following: LDL >130 mg/dL, TG ≥150 mg/dL, or HDL <40 mg/dL in men and <50 mg/dL in women. Metabolic syndrome was defined as simultaneous presence of ≥3 of the risk factors: (blood pressure ≥130/85 mm Hg or intake of anti-hypertensive, waist circumference >102 cm in male or >88 cm in female, serum triglycerides ≥150 mg/dL, HDL-cholesterol <40 mg/dL for male or <50 mg/dL for female, and IFG ≥110 mg/dL). Complete dental evaluation was done by dental formula and tooth mobility. Missing and deciduous teeth were also recorded. Angiographic assessment of coronary lesions was done. Selective coronary angiography in multiple views was performed by standard technique to assess both the extent and severity of disease. Significant CAD was diagnosed by the angiographic evidence of luminal constriction of 50% in left main coronary artery (LMCA) or 70% reduction of lumen diameter of other major epicardial coronary arteries. The patients were classified into single-vessel disease (SVD), double-vessel disease (DVD), or triple-vessel disease (TVD) based on the number of involved coronary vessels. Significant CAD in LMCA was categorized as DVD.
Statistical Analysis
Software Statistical Package for Social Sciences (SPSS) Version 15.0 was used for analysis. Proportions and mean values were compared by chi-square test and independent “t” test, respectively. P value less than 0.05 was considered significant.
Results
A total of 200 patients (170 males and 30 females) were analyzed. The details of demographic characteristics and predisposing factors are shown in Table 1. Mean (standard deviation) age of patients with premature CAD was 38.2 (4.5) years. There was preponderance of male patient (male = 26 [86%]) similarly as in mature CAD group (male = 144 [84%]) (P value = 0.78).
Comparison of Parameters Between Premature CAD (Age ≤45 Years) and Mature CAD (Age >45 Years).
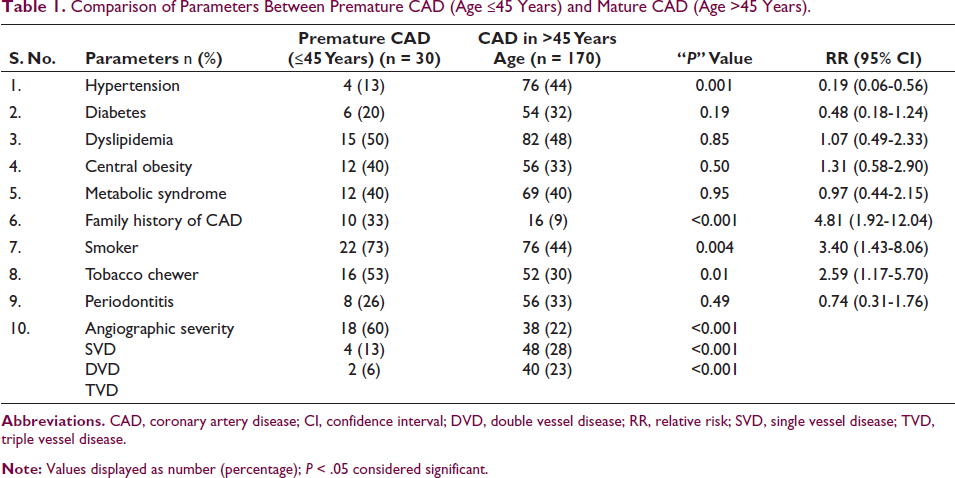
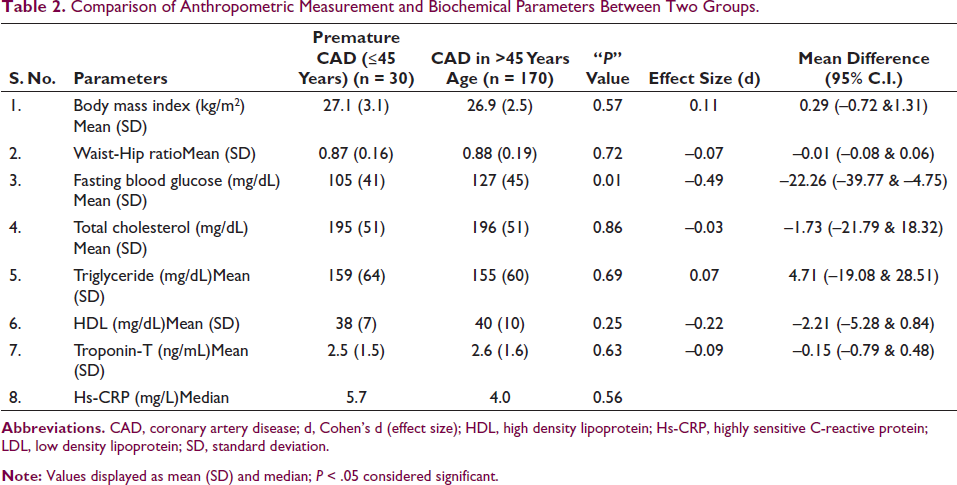
The mean age of females (62.8 ± 12.2) was significantly higher when compared with males (55.7 ± 10.6) (P < 0.001) in the overall cohort. Various cardiovascular risk factors are compared in Table 1. Family history of CAD (P < 0.001), tobacco consumption (P = 0.01), and smoking (P = 0.004) were significantly higher in PCAD while hypertension was significantly higher in mature CAD (P = 0.001). No association of premature CAD was seen with diabetes (P = 0.19) and dyslipidemia (P = 0.85). No association with central obesity, metabolic syndrome, and periodontitis was seen either. SVD was significantly higher in PCAD (P < 0.001) while DVD and TVD were significantly higher in mature CAD (P < 0.001). Fasting blood glucose level was significantly higher in mature CAD group (127 ± 45 mg/dL) as compared to premature CAD group (105 ± 41 mg/dL) (P = 0.01). However, anthropometric measurements and other biochemical parameters between young and old patients were similarly distributed (all P values > 0.05) (Table 2).
Comparison of Anthropometric Measurement and Biochemical Parameters Between Two Groups.
Discussion
Current study reported significant high prevalence of PCAD (15%). Although, this is lesser than the Malaysian study (55%) and study from Iraq (31%).14, 15 However, rate is similar to another study from India reporting 12% to 16% incidence in the young. 8 Hyperlipidemia was found to be prevalent in young Indians with CAD in these studies.16-24 However, the lipid profile has been found to be different between north and south Indian population with or without CAD. North Indians develop CAD at lower levels of total cholesterol.22, 24, 25 Current study did not find dyslipidemia as a significant risk factor for PCAD. Family history of CAD is another important independent predisposing factor for PCAD.16, 17, 24 The INTERHEART study reported population attributable risk of 14.8% in younger contrasted with 10.45% in elder patients. 26 Same study also reported smoking as a larger risk factor in younger men as compared to young women. 26 The risk of CAD increased incrementally with smoking. Various studies from India have reported smoking as a risk factor for CAD in young population.16, 17, 19, 24, 27 Higher prevalence of SVD was like earlier reports.28-30 Contrarily, it showed a significant higher rate of DVD/TVD among mature CAD group.
Study Limitations
Being a single-center hospital-based study, the prevalence cannot be generalized. Limited sample size can lead to referral bias. No data on follow-up was available. Comprehensive evaluation of risk factors and biochemical parameters and angiographic assessment of most of the enrolled patients are the strengths of the current study. Nevertheless, this study identified an unmet scientific need in this area, and it advocates for large studies to confirm these findings.
Conclusion
Family history of CAD, smoking, and tobacco consumption are important risk factors of PCAD. SVD is more common in PCAD. Screening the susceptible population at risk and controlling the cardiovascular risk factors will lead to reduce the epidemic and consequence of PCAD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.