
Abstract
Premature coronary artery disease (CAD) is defined by the early onset of significant atherosclerotic narrowing of the coronary arteries, generally occurring before age 55 in men and 60 in women. This condition is an increasing concern in cardiovascular medicine due to its impact on younger populations, resulting in greater morbidity, diminished quality of life, and a substantial economic burden. Common risk factors include dyslipidemia, hypertension, diabetes, smoking, obesity, and genetic predispositions such as familial hyperlipidemia. This case report describes a 19-year-old male with no known cardiovascular risk factors who presented with an ST-segment elevation myocardial infarction and ventricular tachycardia caused by left main coronary artery disease including the left anterior descending artery and the left circumflex artery. Despite lacking common risk factors, he underwent successful coronary artery bypass grafting with two grafts.
Keywords
Introduction
Coronary artery disease (CAD) is a leading global cause of morbidity and mortality, characterized by atherosclerotic plaque buildup that restricts coronary blood flow. This condition encompasses a range of clinical presentations, including angina, myocardial infarction, and sudden cardiac death. While advances in diagnostic imaging and interventional treatments have improved patient outcomes, the multifaceted nature of CAD poses ongoing challenges for clinicians, necessitating tailored approaches to management and care. 1 CAD is typically seen as a condition that primarily affects older adults, with its prevalence rising significantly with age. 2
Premature coronary artery disease (PCAD) is defined by the development of significant coronary atherosclerosis before the age of 55 in men and 60 in women. It has become a growing concern in cardiovascular medicine due to its early onset and increased risk of serious events, such as myocardial infarction. PCAD is influenced by a mix of modifiable risk factors, including smoking, hypertension, diabetes, and hyperlipidemia, alongside nonmodifiable factors such as genetics, age, and family history. A deeper understanding of the mechanisms driving PCAD and its progression is crucial for enhancing early detection and improving treatment outcomes. 3
Left main coronary artery disease (LMCAD) carries a higher prognostic risk due to the extensive myocardial territory it supplies, which can range from 75% to 100% of the heart muscle, depending on the dominance of the left coronary circulation. 4 The choice of treatment for LMCAD depends on the complexity and location of the disease. Simple lesions in the left main artery can be effectively treated with either PCI or coronary artery bypass grafting (CABG). However, more complex cases, such as distal bifurcation lesions or involvement of multiple vessels, often favor surgical revascularization for better outcomes. 5
Myocardial infarction in adolescents represents a unique diagnostic challenge, raising the risk of misdiagnosis, as this population typically does not exhibit the traditional risk factors for cardiovascular disease seen in older patients. 6 While risk factors for MI in these young individuals may include substance use such as cocaine, trauma, infections, inflammatory conditions, and genetic disorders like familial hyperlipidemia. 7
We report a case of a 19-year-old male who presented with an ST-segment elevation myocardial infarction (STEMI) and triple vessel occlusion, despite having no known risk factors or identifiable cause. The patient successfully underwent CABG with two grafts.
Case presentation
A 19-year-old male was presented to the emergency department after experiencing sudden intense chest pain lasting a few minutes, followed by collapse and reduced consciousness. The patient had no familial risk factors, and there was no history of smoking, alcohol intake, illicit drug use, unhealthy dietary habits, or sedentary lifestyle. His medical history was entirely unremarkable. He maintained a BMI of 23.7 kg/m² (weight: 75 kg, height: 178 cm).
At the emergency department, he underwent an ECG, which revealed ventricular tachycardia (VT). He received a DC shock and lidocaine, after which another ECG showed anterolateral ST elevation. He was then transferred to the hospital for management of VT and acute coronary syndrome. Upon admission to the cardiology department, his vital signs were stable, though he reported chest pain.
Initial workup was conducted including a chest radiograph that appeared normal. Cardiac enzymes were notably elevated, with troponin I at 527.7 ng/mL (normal < 30 ng/L), CK-MB at 331 ng/mL (normal 25–190 ng/L), LDH at 634 (normal 207-414), lactic acid at 62.1 mg/dL (normal 5.7–22 mg/dL), and D-dimer at 1470 ng/mL (normal 0–120 ng/dL). His white blood cell count was elevated at 25.96 × 103 with a neutrophil percentage of 91.7. Cholesterol levels were as follows: total cholesterol 180 mg/dL, triglycerides 94 mg/dL, HDL 28 mg/dL, and LDL 122 mg/dL. Platelet count, serum fibrinogen, and urine toxicology screens were normal. Blood glucose levels remained within normal limits.
A repeat ECG confirmed anterolateral ST elevation (Figure 1). Bedside echocardiography showed normal left ventricular systolic function with an ejection fraction (EF) of 60% and no valvular abnormalities, thrombi, or pericardial effusion. The patient was treated with a loading dose of aspirin and clopidogrel, therapeutic anticoagulation, and an amiodarone infusion. Cardiac catheterization was performed, revealing 70% occlusion of the distal left main artery, 99% occlusion of the origin of the left anterior descending artery, and 90% occlusion of the proximal left circumflex artery (Figure 2).
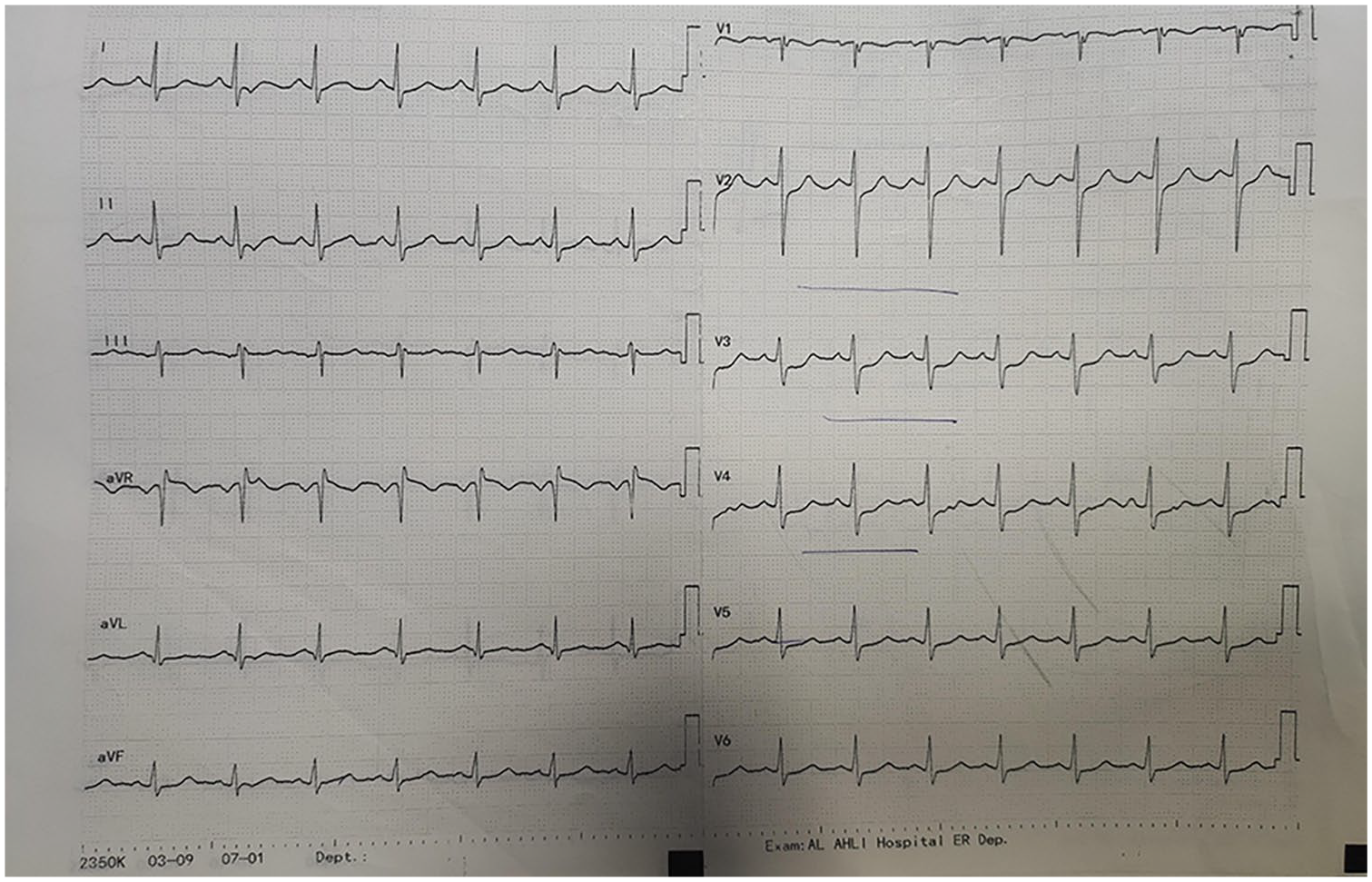
ECG showing ST elevation in the anterior and lateral leads.

Multiple views of coronary catheterization demonstrating severe stenoses: 70% at the distal left main (LM) (yellow arrow), 99% at the origin of the left anterior descending artery (LAD) (red arrow), and 90% at the origin/proximal segment of the left circumflex artery (Cx) (blue arrow).
The patient subsequently underwent myocardial revascularization with CABG. A median sternotomy was performed, and the left internal mammary artery (LIMA) and right internal mammary artery (RIMA) were prepared using a skeletonized technique. Cardiopulmonary bypass was initiated, and grafting was completed with the obtuse marginal artery grafted to the RIMA and the left anterior descending artery grafted to the LIMA. Postoperatively, sinus rhythm was restored, and the patient was successfully weaned off bypass. No intraoperative complications occurred.
Postsurgery, the patient was transferred to the coronary care unit, where he was closely monitored. He received IV fluids, two units of packed red blood cells due to a drop in hemoglobin levels, IV and oral antibiotics, and pain management. Echocardiography on the fifth postoperative day showed good left ventricular function with an EF of 55%, with anterior and septal hypokinesia but posterior and lateral hyperkinesia.
The patient was discharged 1 week later in stable condition, with normal lab results, stable vital signs, and clean, infection-free wounds. Following over 4 months of follow-up, the patient has remained in good health, symptom-free, and continues to show excellent recovery.
Discussion
Published studies have highlighted rising trends in PCAD and a notably higher prevalence of traditional cardiovascular (CV) risk factors, such as hypertension and diabetes mellitus, among young adults. 8 However, no reported cases of PCAD without identified significant risk factors have been documented, as seen in our case. In recent years, the incidence of PCAD has been decreasing. 9
The pathophysiology of MI in teenagers and young adults is diverse and is typically not caused by atherosclerotic plaque rupture, except in cases of genetic predisposition or familial hyperlipidemias. Various nonatherosclerotic causes of premature coronary artery disease include coronary spasm, coronary embolization, coronary dissection, anomalous coronary origin, coronary aneurysm, antiphospholipid syndrome, myocardial bridges, and, in rare cases, hypercoagulable states.10,11
Globally, PCAD poses a significant public health challenge, leading to years of productive life lost and placing additional strain on healthcare systems. Over 80% of individuals with PCAD have at least one modifiable risk factor.12,13
Epidemiological and clinical studies, particularly in developed countries, have identified more coronary risk factors for PCAD. These include various forms of hyperlipidemia like elevated LDL cholesterol, triglycerides, non-HDL cholesterol, and lipoprotein (a), dietary factors such as high intake of saturated and trans fats and refined sugars, as well as genetic influences, alongside broader social determinants.14,15
A systematic review and large-scale survey conducted in Iran identified distinct patterns of risk factors in patients with PCAD compared to healthy individuals with normal coronary arteries. The study revealed that dyslipidemia (52%), cigarette smoking (66%), and a strong family history of coronary artery disease (90%) each significantly increased the risk of developing PCAD compared to controls. 16 Given that PCAD is a multifactorial condition with genetic predisposition playing a key role in its development among younger adults, it is crucial to further investigate and compare risk factors between the patients with PCAD and those without the disease. 17 However, our patient had no identifiable risk factors, a clear past medical and family history, and no prior cardiovascular complaints.
Prevention guidelines from the USA and Europe emphasize the importance of lipid factors in managing and PCAD. 18 However, our patient exhibited mild dyslipidemia, with an LDL level of 122 mg/dL and an HDL level of 28 mg/dL. To the best of our knowledge, this lipid profile alone does not sufficiently explain the severity of his condition.
A thorough differential diagnosis was conducted to explore the underlying causes of the patient’s PCAD. Given the rarity of such cases, the patient and their family were counseled regarding the unique nature of this condition. Upon the patient and his family request for further investigation to determine the cause, whole-exome sequencing was performed to explore the possibility of rare metabolic disorders or atypical presentations of lipid disorders, such as familial hyperlipidemia or combined hyperlipidemia. Autoimmune vasculitides, including systemic lupus erythematosus and Kawasaki disease, were ruled out based on serological markers and clinical history. Hypercoagulable states, such as antiphospholipid syndrome or deficiencies in protein C or S, were excluded using coagulation studies. Toxic exposures, including smoking, recreational drug use, or chronic infections like HIV, were ruled out through patient history, laboratory testing, and toxicology screening. Congenital anomalies of the coronary arteries were also excluded using advanced imaging techniques, such as coronary angiography and CT angiography. This systematic approach to excluding known causes highlights the uniqueness of the case and underscores the need for further investigation into potential unknown or atypical mechanisms behind PCAD.
Hill et al. present a case similar to ours, involving a 16-year-old male who experienced chest pain, ST-segment elevation, and elevated troponin levels, ultimately diagnosed with STEMI despite the absence of traditional cardiac risk factors. Coronary angiography revealed a complete blockage in the left anterior descending artery, which was treated with angioplasty, thrombectomy, and stenting. The patient made a full recovery. The study underscores the need for a broad differential diagnosis when evaluating chest pain in young adults and emphasizes the importance of following adult STEMI management protocols, considering the potential for premature death and long-term disability. 6
For patients with LMCAD, the treatment options include CABG, percutaneous coronary intervention (PCI), and optimal medical therapy. CABG is often preferred, especially for complex cases involving distal bifurcation lesions or multivessel involvement, as it tends to offer better long-term outcomes. Surgical revascularization has been shown to significantly reduce the risk of complications such as myocardial infarction and stroke when compared to PCI. Regardless of the revascularization method chosen, medical therapy remains essential for managing symptoms and controlling risk factors.5,19
Conclusion
This case highlights the importance of considering PCAD in young patients, even in the absence of traditional risk factors. The occurrence of triple vessel disease in a 19-year-old male underscores the complex and multifactorial nature of PCAD, emphasizing the need for a comprehensive diagnostic approach to rule out rare or atypical causes. Early detection and prompt intervention, such as CABG, can result in successful outcomes even in severe cases. This report underscores the necessity of ongoing research into the pathophysiology, risk factors, and optimal management strategies for PCAD in young populations to improve prevention, diagnosis, and treatment.
Footnotes
Acknowledgements
The authors are grateful to the patient and their family for their significant contribution.
Author contributions
WA, HA, BA Writing original draft. MJ review original draft. MS contributed to data collection, data entry, and data interpretation. AA, TI Provide supervision. All authors have read and approved the final manuscript. Each author has participated sufficiently in the work to take public responsibility for the content.
Data Availability
The article contains all the data that support the study’s findings and are readily accessible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.