
Abstract
Background:
Myocardial injury is a common manifestation in patients with coronavirus disease (COVID-19), and the correlation with adverse outcomes has been demonstrated; therefore, adequate monitoring of myocardial injury markers is very important.
Case Summary:
A patient with COVID-19 was hospitalized in our hospital with an initial classification of intermediate risk for myocardial injury, after serial measurements of myocardial injury markers, risk was readjusted to high, as shown later by electrocardiographic abnormalities. The patient underwent emergency diagnostic coronary angiography and successful angioplasty. The patient was discharged to home.
Discussion:
Myocardial injury risk-stratification is essential in patients with COVID-19, since it is essential in the recognition of patients who are susceptible to cardiovascular complications.
Introduction
The degree of myocardial injury is reflected by troponin elevation; it is common in patients with coronavirus disease (COVID-19) and the correlation with adverse outcomes has been demonstrated. 1 The initial mechanism for severe acute respiratory syndrome coronavirus-2 (SARS-CoV2) infection is the binding of the virus to the membrane-bound form of ACE2 which is a membrane-bound peptidase that is expressed in the lungs, heart, vessels, kidney, brain, and gut 2 ; all these organs are potential targets of the virus.
The increase of troponin levels in patients with COVID-19 occurs by different mechanisms: severe respiratory infection accompanied by hypoxemia, cardiac adrenergic stimulation during cytokine storm syndrome, sepsis, systemic inflammation, pulmonary thrombosis and embolism, myocarditis, and type I myocardial infarction. 3
Case Report
A 66-year-old man presented to emergency department with respiratory distress, fever, and 1 week of weakness. His past medical history included diabetes mellitus and hypertension. The patient was evaluated and on examination found to have fever (39°C), tachycardia (105 beats/min), tachypnea with 24 breaths/min, blood pressure of 117/65 mm Hg, and oxygen saturation was 83%. Physical examination demonstrated bilateral crackles in lung auscultation. Laboratory test showed leukocytosis 16,800/µL, neutrophils 12,260/µL, lymphocytes 2,020/µL, and high-sensitive C-reactive protein of 39 mg/L.
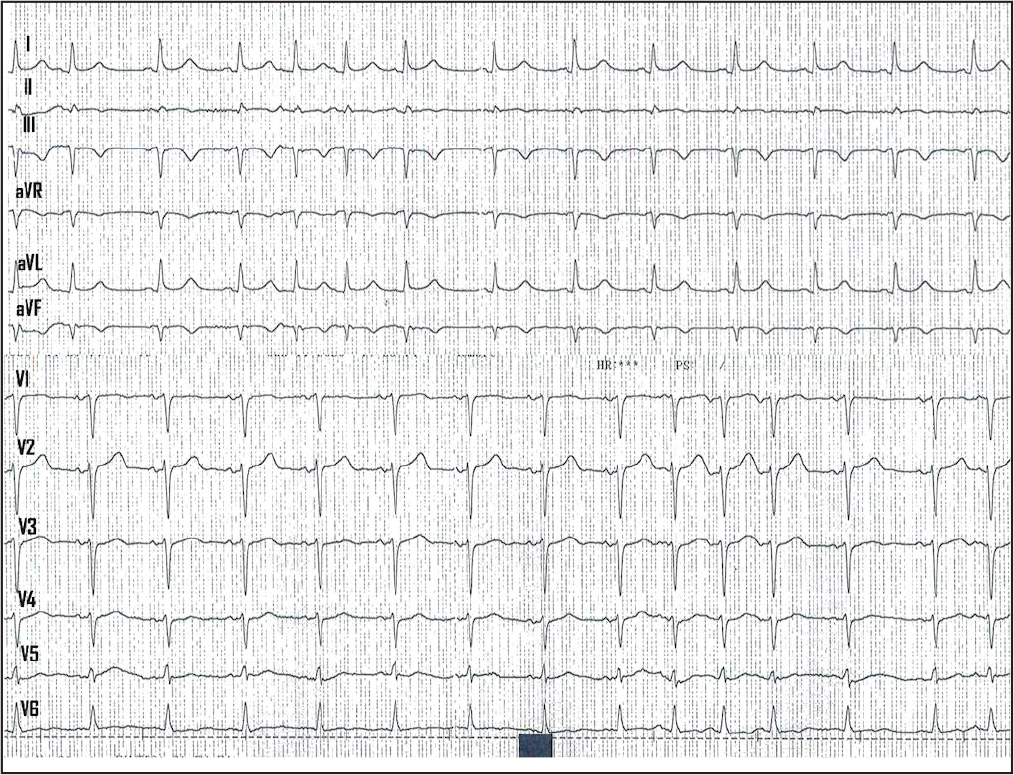
Electrocardiogram Shows Sinus Rhythm, T-waves Inversion in Leads III and aVF, and Premature Supraventricular Beats.
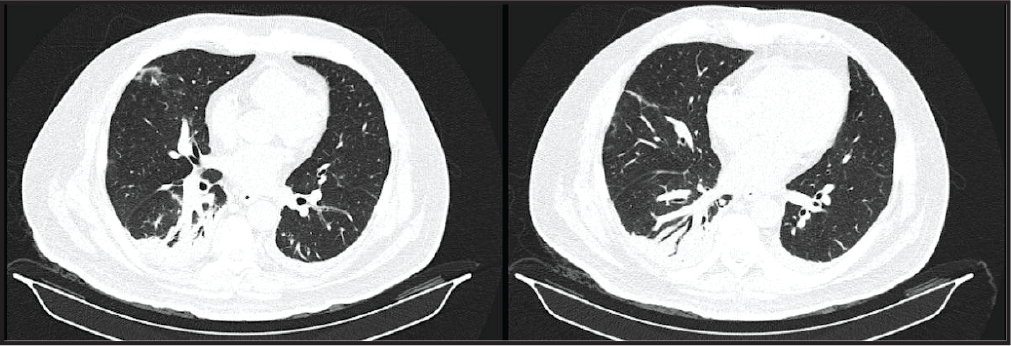
Computed tomography of the chest revealed bilateral basal consolidations and ground glass opacities consistent with an infectious or inflammatory process, the computed tomography angiography was negative for pulmonary embolism (Figure 2).
Computed Tomography of the Chest Reveals Bilateral-basal Consolidations and Ground Glass Opacities.
According to the risk-stratification of myocardial injury based on baseline hs-cTnI measurement, the patient was classified as intermediate risk as a stable patient with significant laboratory abnormalities of myocardial injury. 4 The initial management involved initial supplementary oxygen, dual antiplatelet therapy (aspirin plus clopidogrel), atorvastatin, and enoxaparin.
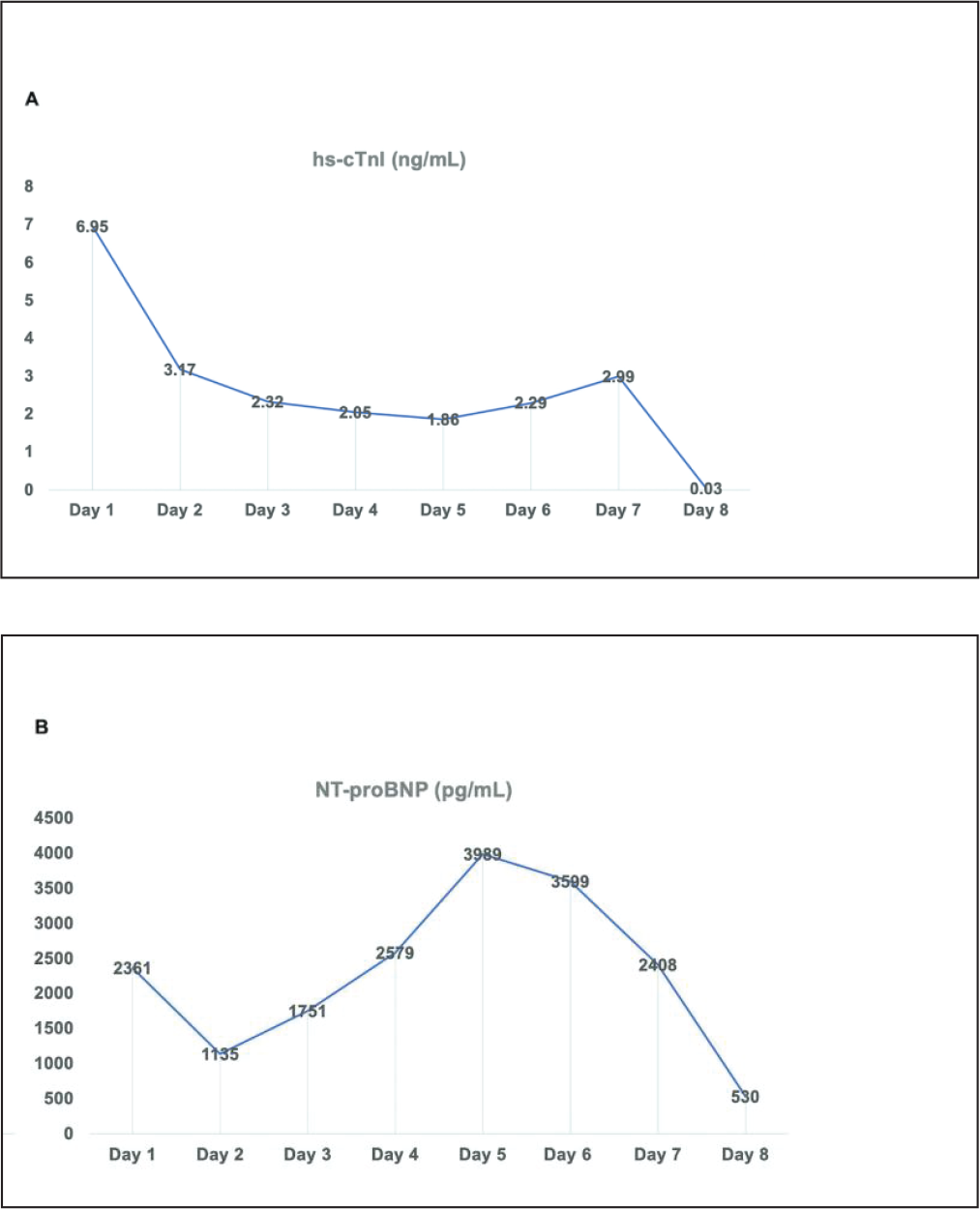
Serial hs-cTnI and NT-proBNP were measured every 24 hours with dynamics shown in Figure 3. Based on serial hs-cTnI and NT-proBNP, we can observe that in the first 3 days the pattern shows a lower risk in the hospital risk-stratification, but after the 4th day the pattern shown was of higher risk. 4 These pattern changes were correlated with the electrocardiographic changes shown on the 7th day of hospitalization (ST elevation and T-waves inversion) (Figure 4).
(A) Serial High-sensitive Cardiac Troponin I (hs-cTnI) Measurements. (B) Serial N-terminal Pro-brain Natriuretic Peptide (NT-proBNP) Measurements.
Electrocardiogram Shows Sinus Rhythm, T-waves Inversion in Leads III, aVF and ST-elevation in Leads V2-V6.
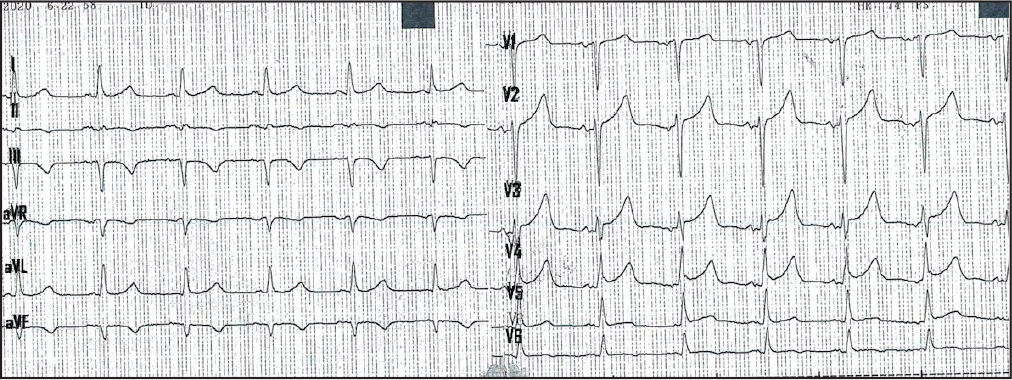
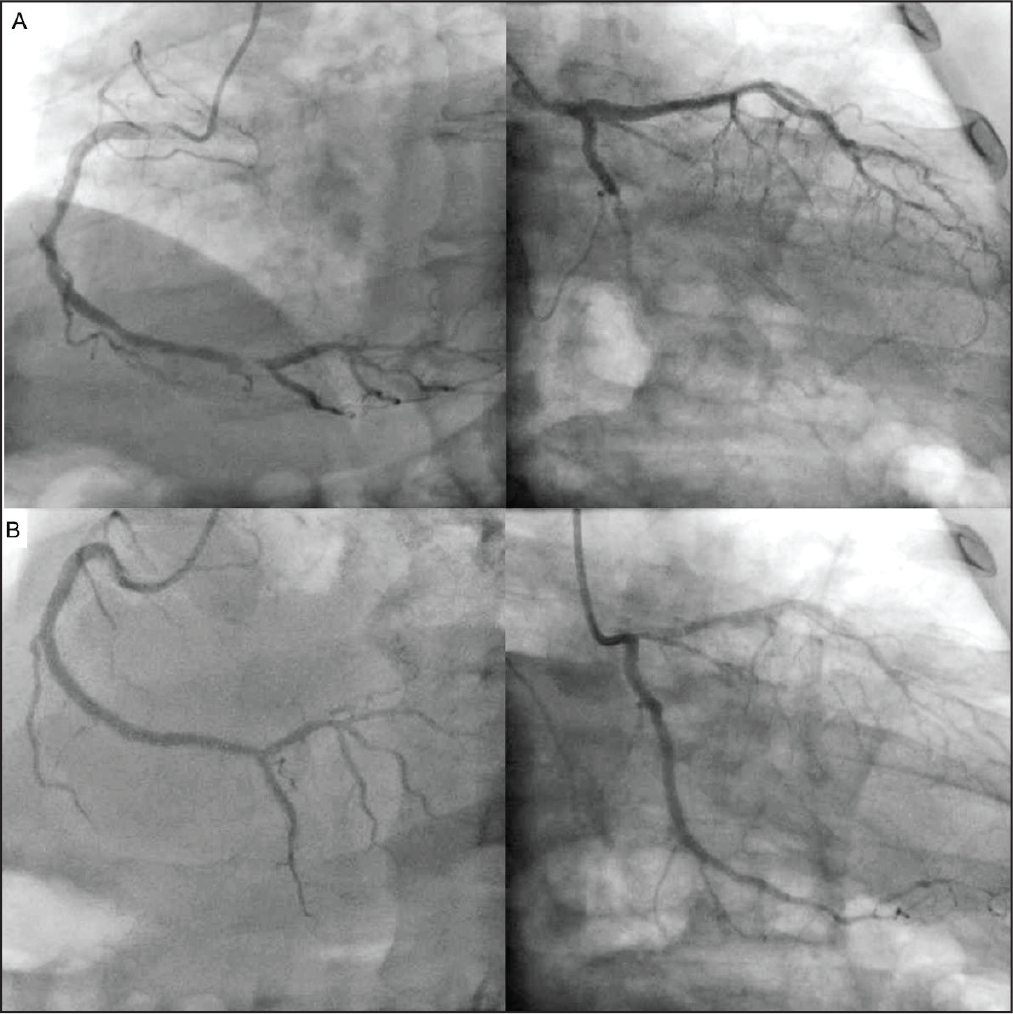
According to changes in the electrocardiogram which consisted of T-wave inversion in leads III, aVF and ST-elevation in leads V2-V6, the patient underwent emergency diagnostic coronary angiography that showed total occlusion of circumflex artery and critical lesion on right coronary. Successful angioplasty to the circumflex and right coronary arteries was performed using medicated stent devices, with TIMI 3 flow in all arteries achieved after the procedure (Figure 5; Movie I and Movie II in the Data Supplement). The patient was discharged to home 2 days later after finishing COVID-19 treatment protocols, which consisted of dexamethasone, enoxaparin, atorvastatin, and empirical antimicrobials for suspected bacterial infection.
(A) Coronary Angiography Showed Total Occlusion of Circumflex Artery and Critical Lesion on Right Coronary. (B) Successful Angioplasty Showed TIMI 3 Flow in All Arteries.
Discussion
The Fourth Universal Definition of Myocardial Infarction defines myocardial injury as cTn concentrations >99th percentile upper-reference limit. 5 Several studies have defined the frequency of myocardial injury in COVID-19,6,7 however, sampling hs-cTnI intervals used are often not well defined. We present a clinical case that underscores the use of serial (every 24 hour) measurements to detect changing patterns of hs-cTnI and NT-proBNP that facilitate the identification for additional intervention, in this case successful angioplasty.
It is important to understand that the initial role of hs-cTnI measurements is for risk-stratification and if it is necessary, serial hs-cTnI can help us understand that initial abnormal hs-cTnI results do not equate to acute myocardial infarction in many cases, but the incorporation of hs-cTnI measurement to a set of other inflammatory and thrombotic markers to facilitate the understanding of COVID-19 stages 8 and risk profiles. On the other hand, it is important remember that the inflammatory and thrombotic responses to COVID-19 infection increase the risk of nonischemic myocardial injury, mentioned previously; and acute myocardial infarction as our clinical case.
Myocardial injury is common in patients with COVID-19; COVID-related myocardial injury etiologies can include myocarditis, myocardial infarction, sepsis-related myocardial injury, and/or stress-induced cardiomyopathy. In our patient, at the beginning of hospitalization, the first etiological option that we considered was myocarditis and we decided to continue with serial measurements of markers of myocardial damage. However, on day 7 of hospitalization, a new ST-segment elevation was observed in the electrocardiogram associated to elevation of troponin levels, so we decided to perform coronary angiography in which we found coronary obstruction. After said procedure, changes in the electrocardiogram were reversed and troponin levels decreased.
We consider that the myocarditis, stress-induced cardiomyopathy, and sepsis-related cardiomyopathy are always diagnoses made by elimination/exclusion in the context of a patient with a new ST-segment elevation on electrocardiogram.
Conclusion
Cardiac troponin increases indicative of myocardial injury are frequent in patients with COVID-19, due to diverse mechanisms previously described. 3
The increased inflammatory and thrombotic responses in patients with COVID-19 increase the risk for nonischemic myocardial injury and acute myocardial infarction. To facilitate the detection of myocardial injury and risk-stratification, an important role may exist for serial hs-cTnI measurements among hospitalized patients with COVID-19.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for ST-Elevation Myocardial Infarction and COVID-19 Pneumonia: The Importance of Risk-Stratification of Myocardial Injury in COVID-19 Era by Julio C. Sauza-Sosa, Oscar Millan-Iturbe, Jorge Mendoza-Ramirez, Carlos N. Velazquez-Gutierrez, Erika Lizeth De la Cruz Reyna, Alfredo Gutierrez-Marin, and Jorge A. Fernandez-Tapia, in Indian Journal of Clinical Cardiology
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.