
Abstract
Total anomalous systemic venous connection (TASVC) with interruption of inferior vena cava in the absence of heterotaxy is an extremely rare anomaly. TASVC is diagnosed when both the caval veins and coronary sinus drain into the left atrium. The diagnosis of TASVC is possible only when all the systemic veins (both superior and inferior caval veins) and coronary sinus drain into the left atrium in the setting of normal or mirror-imaged atrial arrangement. The presence of cyanosis despite left-to-right shunt across an atrial septal defect with hypoplastic or small right heart chambers should arouse the suspicion of TASVC. The severity of symptoms and the age of presentation depend highly on mixing at the atrial level across the atrial septal defect. The amount of mixing also decides the growth of the right atrium, right ventricle, main and branch pulmonary arteries. Adequately sized right heart chambers and tricuspid annulus with good mixing at the atrial level facilitate complete correction and event-free survival. Prompt diagnosis is possible with contrast echocardiography performed both from upper and lower limb veins, cath study, and cardiac computed tomography or magnetic resonance imaging. However, it is not uncommon to note that even in the era of advancement in echocardiography, the complete miss diagnosis of this entity as single ventricle physiology and denial to the patient of possible complete surgical correction. We are reporting here a case of successfully treated TASVC with interrupted inferior vena cava in an adolescent.
Keywords
Introduction
Total anomalous systemic venous connection is a rare anomaly, where all systemic veins, ie, inferior vena cava (IVC), superior vena cava (SVC), and coronary sinus (CS), drain into the left atrium (LA). 1 It may be seen in isolation or with other congenital anomalies, cardiac malposition, or heterotaxy syndrome. 2 The amount of left-to-right shunt governs the growth and size of the right atrium (RA) and right ventricle (RV). 3 Patients with small shunts have hypoplasia of the right-sided chambers and present with intense cyanosis early in life, whereas the presence of a large shunt allows good oxygenation, adequate growth of RA and RV, thus permitting complete surgical repair, 4 as noted in this case. This diagnosis is often missed entirely, and the arrangement is misinterpreted as the functionally single ventricle. 4
This article reports a scarce case of total anomalous systemic venous connection (TASVC) with interruption of IVC and its successful management in an adolescent girl.
Presentation
A 15-year-old girl, with no significant family history, normal developmental milestones presented with bluish discoloration of nails and exertional fatiguability since early childhood. She had no history of cyanotic spells, stroke, or prior infective endocarditis.
Clinical examination revealed a pulse rate of 110 bpm, BP of 90/60 mmHg, respiratory rate of 20/min, peripheral arterial oxygen saturation (SpO2) of 84% on room air, normal jugular venous pulse, and grade 3 clubbing. Cardiovascular and other system examination was unremarkable.
Investigations
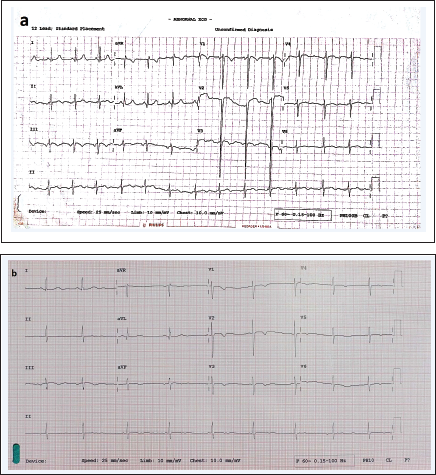
Complete blood count showed hemoglobin of 22.7 g%, packed cell volume of 69.3%, and red cell count of 8.36 mn/cumm. Other blood investigations were within normal limits. Electrocardiogram revealed sinus rhythm, an axis of –30°, deep S waves, and T wave inversion in V1 to V4 (Figure 1). Chest X-ray was unremarkable (Figure 2).
Electrocardiogram (ECG) Before Intra-cardiac Repair (ICR): (a) Sinus Rhythm, a Leftward Axis of –30°, Deep S Waves, and T Wave Inversion in V1 to V4. (b) ECG After Five Years Post-ICR Showed Similar Findings Excepting S Wave Amplitude Reduction in V1 to V4.
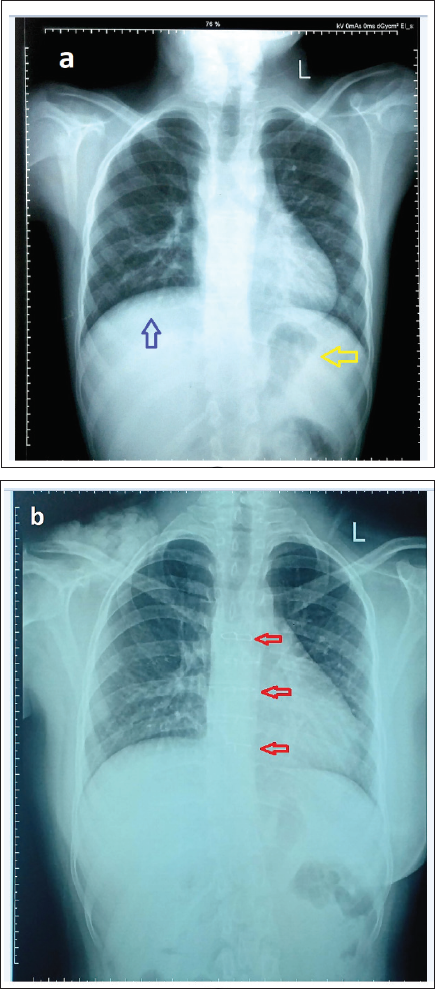
Pre-ICR-Chest X-ray PA View: (a) No Significant Cardiac or Lung Pathology. Situs Solitus Can be Noted With a Left-Sided Fundic Gas Shadow (Yellow Arrow) of the Stomach and Liver Shadow on the Right Side (Blue Arrow). (b) Post-ICR CXR PA View Showing Similar Findings. However, Red Arrows Showing Sternal Binders Indicating Surgery.
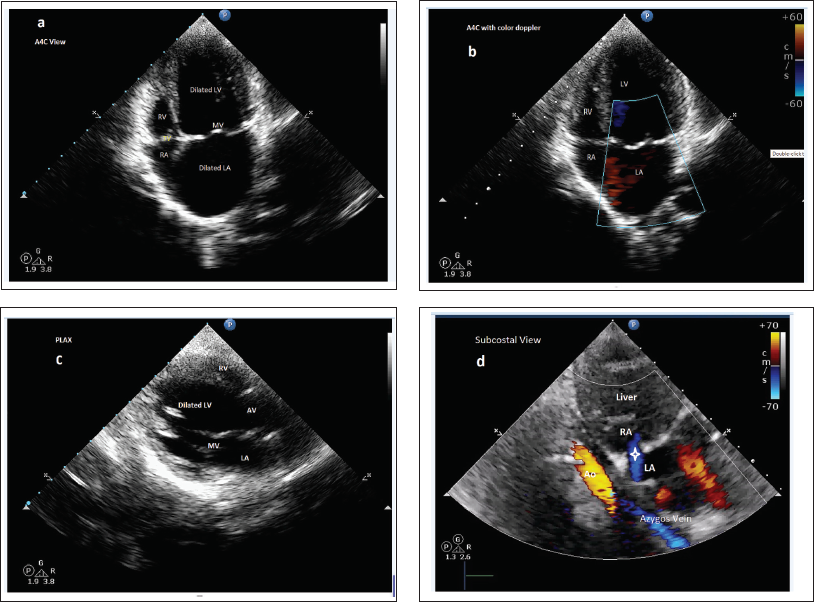
Two-dimensional ECHO (2D-ECHO) findings: Showed dilated LA and left ventricle (LV), fully formed but smaller RA and RV, IVC not draining into RA, and left-to-right shunting high ostium secundum (OS)-atrial septal defect (ASD). Other findings were unremarkable.
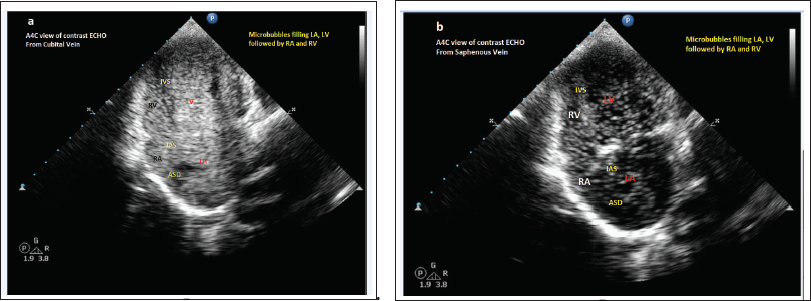
Saline contrast 2D-ECHO: Demonstrated left to right shunt at the atrial level (late opacification of RA) when performed on both cubital veins. Contrast injection into the right saphenous vein confirmed anomalous drainage of both SVC and IVC to LA. The drainage of the CS could not be clarified (Figures 3 and 4, Video Clips 1 and 2).
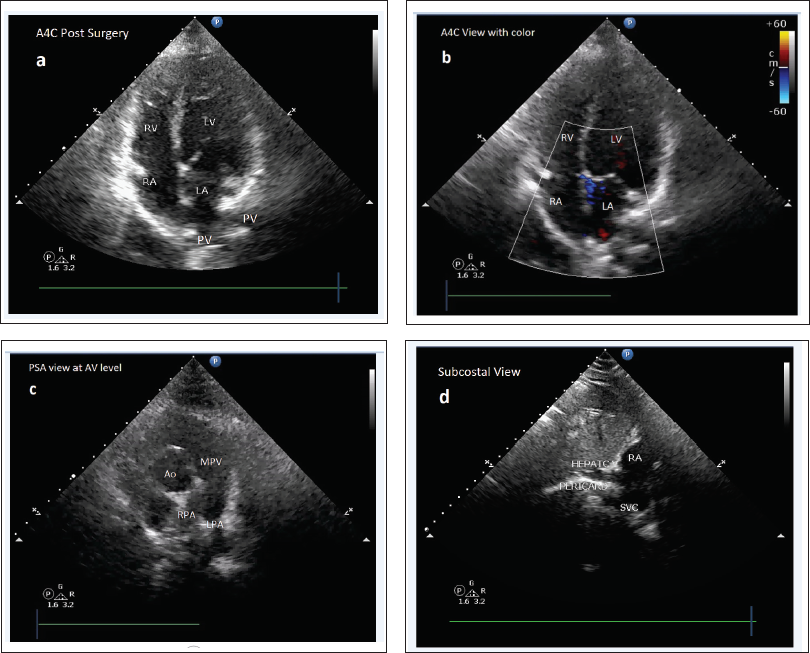
Pre-ICR ECHO Cardiography: (a ) A4C View: Dilated LA and LV, With Smaller RA and RV, (b ) A4C View With Color Doppler, (c ) Parasternal Long-Axis View (PLAX) Showing Dilated LA and Other Structures as Marked, (d ) Subcostal View Showing no Clear Evidence of Intrahepatic IVC With Aortic and Azygos Flow, a High Ostium Secundum ASD with a Left-to-Right Shunt (White Star Head). Ao, Aortic Flow; RA, Right Atrium; LA, Left Atrium; RV, Right Ventricle; LV, Left Ventricle; MV, Mitral Valve; AV, Aortic Valve.
Saline Contrast ECHO Cardiography: Showing Opacification of All Chambers (LA and LV Followed by RA and RV) When Agitated Saline Was Injected Through (a ) Cubital and (b ) Saphenous Veins.
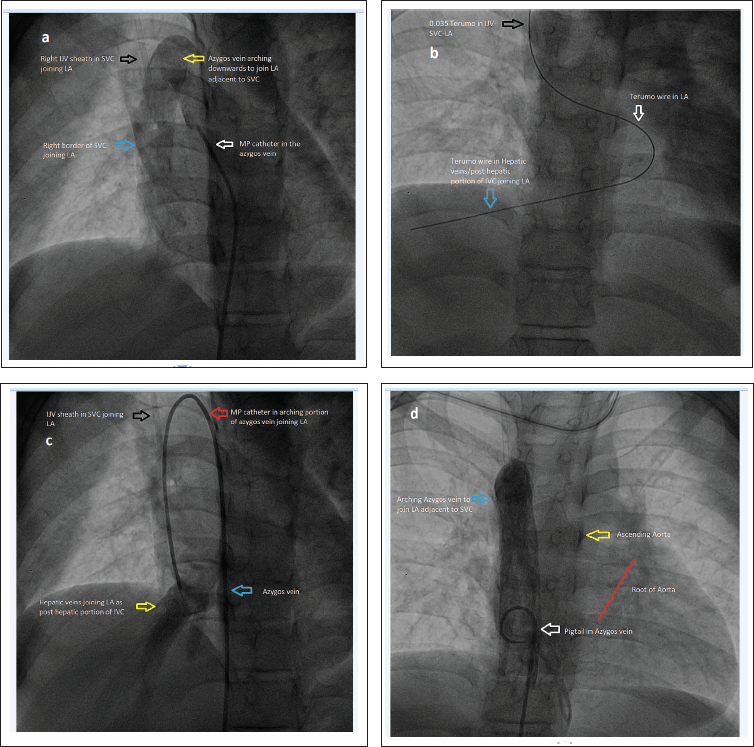
Cardiac Catheterization: (a ) Right SVC and Azygos Veins Joining LA and (b ) Showing Terumo Wire Entering From the Right Internal Jugular Vein-SVC-LA-Hepatic Veins. (c ) Showing Drainage of Hepatic Veins into LA. MP Catheter in IVC-Azygos-SVC-LA-Hepatic Veins. (d ) Dilated Azygos Vein Imaged Using Contrast Injection With a Pigtail Catheter.
Management
Given reasonably developed RA and RV with a good amount of blood flow to lungs maintained via a high OS-ASD with a left-to-right shunt, the heart team planned and performed complete re-routing of all the systemic veins into RA and atrial re-septation. The CS, which was found draining into the LA, was left alone. Pre- and postprocedure imaging are depicted in Figure 6 and Video Clips 5 and 6 for comparison.
2D-ECHO After Five Years of Corrective Surgery: (a ) A4C View Showing Well-Developed RA and RV and (b ) The Colour Doppler Image Showing no Evidence of ASD, (c ) Parasternal Short-Axis View (PSA)-Adequately Sized MPA, LPA, and RPA, (d ) Subcostal View Showing Hepatic Veins and SVC Joining RA With Pericardial Patch Used for Reconstruction.
Discussion
The TASVC is diagnosed when both IVC, SVC, all the hepatic veins, and CS are connected to morphological LA. 5 It is an extremely rare congenital anomaly with unknown prevalence. TASVC is diagnosed only in normal or mirror-imaged atrial arrangement and is not tenable even if one of the systemic veins joins the RA. 1
Interruption of the IVC is rare, with an incidence of approximately 1:5000 of the population, based on prenatal ultrasound screening. In 90% of cases, it occurs as an isolated anomaly, although it may be associated with cardiac or splenic abnormalities. 6 The suprarenal segment of the IVC, in this case, drained into LA via the azygos vein. In rare cases, IVC may drain via the hemiazygos vein if there is a left-sided IVC. The prevalence of azygos continuation of the IVC is ∼1.5%, and the range is 0.2% to 3%, 7 in which case azygos vein will be dilated. The posthepatic segment of the IVC, which is embryologically derived from the right vitelline vein, was present in this case and was draining into LA. The case described in this report included a very rare occurrence of TASVC with interrupted suprarenal/intrahepatic portion of the IVC, which represents a failure of fusion of the vitelline and subcardinal embryological portions of the IVC. 8 The occurrence of interrupted IVC in TASVC is hardly reported in the literature.
Conclusion
TASVC, in association with the interruption of IVC, is an extremely rare anomaly. TASVC should be a differential diagnosis in the presence of cyanosis despite left-to-right shunt across an ASD, in the setting of hypoplastic or small right heart chambers with concordant atrioventricular and ventriculoarterial connections. Complete surgical repair is possible with good mixing at the atrial level and adequately sized RA and RV, as noted in this case.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.