
Abstract
Syncope is a symptom that is commonly encountered in the practice and may point to a cardiac or neurological diagnosis. The evaluation of syncope rests on a thorough clinical evaluation, aided by electrocardiogram (ECG) findings, followed by risk stratification of the particular case. Once high-risk factors have been ruled out, the patient can be further diagnosed as having a reflex syncope (RS), orthostatic hypotension, or cardiac syncope based on specific clues. If the initial evaluation is not confirmatory various diagnostic tests may be used to guide further management (eg, long-term ECG monitoring, tilt table testing, etc). The management should be based on the overall profile of the patient and not only on any single test. In this review, we discuss the evaluation of a patient with RS and give an overview of treatments available for the patients.
Abbreviations
AMI: Acute myocardial infarction
ARVC: Arrhythmogenic Right Ventricular Cardiomyopathy
AV: Atrioventricular
BP: Blood pressure
BrS: Brugada syndrome
CHF: Congestive heart failure
CLS: Closed-loop stimulation
CPM: Counterpressure maneuverers
CSM: Carotid sinus massage
CSS: Carotid sinus stimulation
ED: Emergency department
ELR: External loop recorder
EPS: Electrophysiological study
ILR: Implantable loop recorder
ISSUE: International study on syncope of unexplained etiology
LOC: Loss of consciousness
LQTS: Long QT Syndrome
LVOTO: Left ventricular outflow tract obstruction
NT-TLOC: Non-traumatic transient loss of consciousness
OH: Orthostatic hypotension
POTS: Postural orthostatic tachycardia syndrome
RS: Reflex syncope
SCD: Sudden cardiac death
TLOC: Transient Loss of Consciousness Úfter Sudden cardiac death
TT: Tilt training
TTT: Tilt table testing
UI: Urinary incontinence
VASIS: Vasovagal syncope international study
Introduction
One of the most challenging symptoms to evaluate, encountered by the medical practitioners, is syncope (pronounced “sing-kuh-pee”). Syncope is a syndrome in which there is a total loss of consciousness due to cerebral hypoperfusion, characterized by a rapid onset, short duration, and spontaneous complete recovery. 1 2 3 Syncope can be caused due to traumatic head injury which is outside the scope of this article. Most of the syncope seen in clinical practice is non-traumatic. Nontraumatic transient loss of consciousness (NT-TLOC)is defined as a real or apparent loss of consciousness (LOC), with loss of awareness for a short duration. 3 A clear and detailed history taking and a focused clinical examination for specific causes of syncope do lead to the diagnosis of the etiology in the majority of the cases. In a patient with NT-TLOC, one needs to rule out epileptic seizures, psychogenic LOC (pseudo-seizure), and other vascular causes (eg, subclavian steal syndrome, subarachnoid hemorrhage, etc), based on clinical and investigational clues, to come to the diagnosis of syncope. 4 The important thing to remember is—syncope is not a complete diagnosis but just the presenting symptom and identifying the underlying cause is important. 2
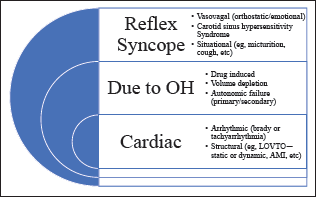
The causes of syncope can be broadly classified into reflex syncope (RS) (neurally mediated), syncope due to orthostatic hypotension (OH), and cardiac syncope, as per the European Practice Guidelines (Figure 1). 3 RS is the most common cause of syncope irrespective of age or clinical setting. 3 5 6 The epidemiological studies have shown that RS is common in the younger population, whereas cardiovascular causes are common in older individuals. 5 Syncope is considered to be due to cerebral hypoperfusion with a combination of multiple central as well as peripheral mechanisms. 3 7
Since the frequency and severity of syncope vary in the patients with RS, there is a myriad of treatment options available ranging from lifestyle management to cardiac ganglion ablation. 7 In this review, we will give a brief overview of the evaluation and treatment of RS.
Clinical Evaluation and Approach to Symptoms
The evaluation can be divided into 3 phases: history, examination, and investigations.
History
The most important component of the evaluation of a suspected case of syncope is history taking.
8
The goal of history taking would be as follows: (a) To establish the etiology of syncope with certainty and differentiate it from epileptic or nonepileptic seizure. (b) Clues to suggest the probable etiology of the syncope like RS.
8
To establish the etiology of syncope with certainty and to differentiate it from epileptic seizure or pseudosyncope (Table 1).
Differentiation of Syncope From Epileptic and Psychogenic LOC/syncope.
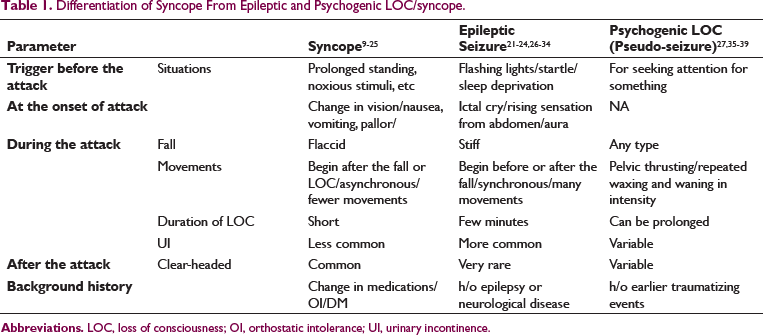
The goal should be in eliciting the history of sudden or gradual transient loss of consciousness (TLOC) with total recovery after a few seconds/minutes from the patient or bystanders. The following questions will be required to get clues regarding differentiation of syncope from epileptic seizure or nonepileptic seizure:
What was the body habitus?—supine/sitting/standing What was the activity?—meal, exercise, and so on. Were there any precipitating factors?—warm crowded place, fear, pain, cough, and so on. What were the historical details from the eyewitness with regard to the event? —duration, associated body movements, tongue bite, post-event confusion, and so on. What is the background history?—frequency, h/o sudden cardiac arrest, neurological disease, diabetes mellitus, vasoactive medications, and so on. What was the body habitus?—supine/sitting/standing.
There is a definite value for the video evidence of the event, so the relatives may be asked to record an episode if it occurs in the future again.
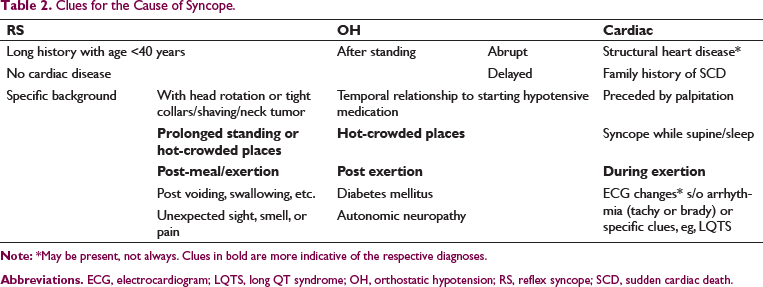
2. Is it a reflex-mediated syncope (RS) or syncope due to orthostatic hypotension or cardiac etiology?
Clues for the Cause of Syncope.
Examination
The physical examination should be focused to rule out or confirm the suspected cause of syncope. In particular, evidence of bradycardia, OH, and ejection systolic murmur should be looked out for to rule out organic causes of syncope. 40
Certain diagnostic clinical tests may aid in the diagnosis of the specific cause of syncope.
This test is used to diagnose different types of orthostatic intolerance.
3
The resting blood pressure (BP) of the patient should be measured in the supine position. Then the patient is made to stand without support and continuous BP monitoring is done. BP should be noted at 1-min and 3-min intervals, if continuous monitoring is not possible. The definition used for the abnormal test is—“abnormal BP fall is defined as a progressive and sustained fall in systolic BP from the baseline value ≥20 mmHg or diastolic BP ≥10 mmHg, or a decrease in systolic BP to <90 mmHg.” The test can classify OH into classical (within 30 s-3 min) and delayed OH (after 3 min).
43
The sensitivity, specificity, and accuracy of the active standing test were found to be 58.8, 63.3, and 60.9, respectively.
44
2. Carotid sinus stimulation
45
This test is useful in the diagnosis of carotid sinus syndrome (CSS). Carotid sinus stimulation can be performed with mechanical stimulation (carotid sinus massage [CSM]) or pharmacological stimulation (with nitroprusside and phenylephrine injections). CSM is performed by giving 5-s gentle pressure over the carotid sinus on one side with continuous heart rate and BP monitoring, in supine as well as 60o upright position. Carotid sinus hypersensitivity is considered to be present if CSM elicits asystole ≥3 s (cardio inhibition) and/or a fall in systolic BP >50 mmHg (vasodepression).
6
Reproduction of spontaneous syncope is considered as a relatively specific diagnostic sign for CSS.
46
Three forms of CSS may be diagnosed based on associated asystole ≥3 s or hypotension (any drop in systolic BP).
Vasodepressor: Syncope + Fall in Systolic BP + No Asystole ≥3 s Cardioinhibitory: Syncope + No Fall in Systolic BP + Asystole ≥3 s (sometime ≥ 6 s) Mixed: Syncope + Fall in Systolic BP (present/absent) + Asystole ≥3 s ↓ Atropine for the elimination of asystole ↓ Symptoms persist
The sensitivity and specificity of CSM to diagnose CSS were found to be 74% and 100%, respectively, in the supine position. The sensitivity increases to 100% if the test is performed in the upright position.
47
3. Clinical autonomic function tests
Valsalva maneuver During the maneuver, the patient is asked to conduct a maximally forced expiration for 15 s against a closed glottis, that is, with a closed nose/mouth, or into a closed system with 40 mmHg resistance.
6
Traditionally, the Valsalva ratio (ratio of maximum heart rate during expiration and minimum heart rate within 30 s after maximum heart rate) has been used to evaluate the autonomic function but it may give erroneous readings in the patients who have inadequate expiratory efforts, square wave BP response, and blunted phase IV overshoot.
48
Therefore, the common findings used are:
Deep breathing The patient is asked to breathe deeply at 6/min under continuous heart rate and BP monitoring.
6
52
Blunted or abolished heart rate variability during deep breathing (expiratory/inspiratory [E/I] index), that is, <15 bpm in healthy individuals of >50 years of age, is considered abnormal. A parasympathetic dysfunction should be ruled out in these patients.
48
50
Investigations
The investigations should be tailored as per the presenting complaints of the patients. Electrocardiogram (ECG) is considered an emergency investigation when the diagnosis of cardiac syncope is to be confirmed.
Used to rule out serious cardiac conditions (eg, acute coronary syndrome, heart blocks, pulmonary embolism, etc) or certain specific ECG characteristics (eg, long QT syndrome, short QT syndrome, Brugada syndrome, preexcitation syndrome, etc).
Holter (24 h or 3 days)—will be useful for daily syncopal events, with normal/unclear presenting ECG. External loop recorder (3-30 days)—for a less frequent event and implantable loop recorder (ILR) (up to 3 years)—for infrequent events only in the patients with high suspicion of arrhythmic cause. A major limitation with Holter monitoring is frequent noncompliance with keeping a log of symptoms and event markers (from the patient’s side), which may cause errors in the interpretation of Holter findings as symptom-event correlation becomes difficult.
53
The significant pause detected on long-term monitoring is traditionally considered to be ≥3 s, which has been included as an indication for permanent pacing in the American and European guidelines. This is based on observational evidence with low specificity, which has been challenged by recent studies.
54
55
Most of these studies concluded that the follow-up was not sufficient enough to decide on the benefit of permanent pacing.
56
ECG recordings on ILR were analyzed on follow-up in the first international study on syncope of uncertain etiology (ISSUE) study which has divided the findings into—Type 1 (asystole ≥3 s) [IA: sinus arrest, IB: sinus bradycardia with AV block, IC: AV block]; Type 2 (bradycardia) [2A: decreased HR >30%, 2B: HR <40 bpm for >10 s]; Type 3 (no/slight rhythm variation) [3A: none/<10% HR variation, 3B increase 10-30% and HR <120 or decrease 10-30% and HR >40 bpm]; Type 4 (tachycardia, ie, increase in HR >30% or >120 bpm) [4A: progressive sinus tachycardia, 4B: atrial fibrillation, 4C: supraventricular tachycardia (non-sinus), 4D: ventricular tachycardia].
57
A series of studies was carried out to define the need and clinical significance of ILR in patients with suspected RS.
57
58
59
These studies have defined cardioinhibitory responses based on the international study on syncope of uncertain etiology (ISSUE) classification as type 1 (asystole) or 2 (bradycardia).
57
Mobile phone-based monitoring The use of mobile phones and different apps focusing on cardiovascular disease (eg, atrial fibrillation) has increased tremendously over the last few years.
60
Mobile phone-based plethysmography and handheld ECG recorders with external sensors have been used for monitoring cardiac rhythm.
61
The study comparing various applications (apps) used for this purpose showed that there is wide variability in quality, functionality, and adherence to self-management behaviors in these apps.
62
Further studies are warranted in order to use these mobile phone applications for large-scale screening of heart rhythm abnormalities. Artificial intelligence and its subfields (ie, machine learning and deep learning) have found their utility in the monitoring of heart rhythm, diagnosis of certain conditions, and correlation of ECG findings with imaging (eg, left ventricular ejection fraction).
63
64
65
Tilt table testing (TTT) has been considered complementary to clinical examination since its inception in 1986. 66 The test typically carried out after 2 to 4 h fasting that involves ≥20 min supine phase (post-venous cannulation) followed by ≥20 min of tilt (60-80o) (passive phase) with or without the use of a provocative agent (nitroglycerine, isoproterenol, or clomipramine) for 5 to 20 min (active phase) if the first phase of the test is negative. 67 68 69 70 TTT is considered to be positive only if there is syncope during the testing. 3 The response can be mixed (type 1), cardioinhibition without asystole (type 2A), or cardioinhibition with asystole (type 2B), and vasodepressor (type 3) as per the new Vasovagal Syncope International Study (VASIS) classification. 71 Cardioinhibitory response means that HR falls to less than 40 bpm for more than 10 s but asystole >3 s doesn’t occur (BP falls before HR fall) (Type 2A) or asystole occurs for >3 s (BP falls with or before HR fall) (Type 2B). The positivity rate of TTT depends upon the indication for the test and provocative agent used—highest for vasovagal or emotional syncope with clomipramine (>90%), around 50% for atypical syncope (without classical features of vasovagal syncope 72 ) with nitroglycerine, and lowest ≤30% for unexplained syncope. 73 74 The sensitivity and specificity of TTT with the use of isoproterenol or sublingual nitrate have been reported to be similar (sensitivity: 61-69%; specificity: 92-94%). 68 69
Recently, there have been contrasting publications regarding the usefulness of TTT. One of these has advocated the abolishment of the test in view of no additional diagnostic benefit, high false positivity rates, use of active standing test instead of TTT in the patients with OH or postural orthostatic tachycardia syndrome, and no mortality benefit. 75 The other has highlighted the benefits of TTT as an ancillary test in the evaluation of suspected syncope and reiterated that it should be used as a part of the diagnostic workup, not as a standalone to draw any conclusions. 76 We propose that TTT may play a role in cases where the history is not diagnostic, provided the more serious causes like cardiac syncope are ruled out.
24-h ambulatory BP monitoring is recommended for the diagnosis and management of hypertension, as per the recent guidelines. 77 This can help in the diagnosis of OH based on nocturnal “non-dipping” (decrease in BP of less than 10% during night-time) or “reverse-dipping” (increase in BP at night) patterns. 78
Echocardiography is useful to rule out underlying structural heart disease which can present with syncope viz. left ventricular outflow tract obstruction (ie, aortic stenosis or hypertrophic cardiomyopathy), obstructive masses, pericardial tamponade, aortic dissection. 79 80 81 82 83 84 In the cases where resting echocardiography is normal but there is high clinical suspicion, a stress echocardiogram may help in the confirmation of the level of obstruction in the patients with hypertrophic cardiomyopathy. 85 86
The group of patients in which there is suspicion of cardiac syncope based on ECG changes (eg, sinus pauses, bifascicular blocks, etc) or history of acute myocardial infarction/low ejection fraction, electrophysiological study may aid in deciding the further course of action (eg, need for a pacemaker in a patient with bifascicular block and pharmacological challenge [≥80% positive predictive value] or need for implantable cardioverter-defibrillator in patients with low ejection fraction [yield of 42% in whom VT was inducible], etc). 3 87 88 89
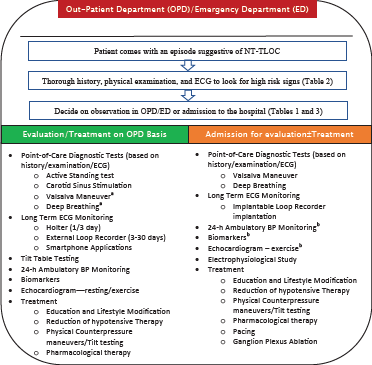
Evaluation Algorithm
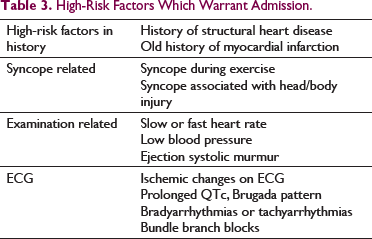
High-Risk Factors Which Warrant Admission.
Treatment
Overall management depends upon the predictability and frequency of the symptoms. Patients may be classified into 2 groups:
Group I: Unpredictable or high-symptom-frequency of syncope ↓ will need specific therapy.
Group II: Predictable or low-symptom-frequency of syncope ↓ education/reassurance may be enough.
The treatment should start with the education of the patient and relatives regarding the cause of syncope and then further treatment may be required in cases where there are high-risk ECG features, recurrence of symptoms, or nonresponse to conservative management.
The various treatment modalities used are:
This forms the cornerstone of the treatment of RS, but its long-term effects have not been evaluated with randomized studies. 3 The main components are:
The patients with hypotensive susceptibility (HS) may be helped with the reduction of hypotensive therapy targeting a systolic BP of 140 mmHg to reduce symptoms. 3
Isometric muscle exercises and counterpressure maneuvers viz. leg crossing, hand gripping, and hand tensing may help reduce syncopal episodes. 94 95 They need to be taught and should be employed when the patient recognizes the prodrome. 6 These maneuvers may help prevent and/or abort an episode of RS or orthostatic fainting. Leg crossing is done with maximum tensing of the leg, abdominal, and buttock muscles for the maximum tolerated time or until the disappearance of symptoms. Hand gripping means squeezing a rubber ball or similar soft object in the dominant hand for the maximum tolerated time or until the disappearance of symptoms. Arm tensing consists of maximum tolerated isometric contraction of the 2 arms achieved by gripping 1 hand with the other and at the same time abducting for the maximum tolerated time or until the disappearance of symptoms. 6
In patients with RS which is triggered by orthostatic stress, the prescription of a prolonged period of enforced upright posture is called tilt training. 96 The training is generally started in a hospital setting with 10- to 50-min sessions based on the prodromal symptoms and then home training is advised. 97 The hospital training generally is similar to the protocol used for diagnostic TTT. After discharge, the patient is advised to continue the training with feet 15-cm away from the wall with upper back resting on the wall for increasing time starting from 15 min based on the symptoms. 98 There is conflicting evidence regarding the use of tilt training, with a few studies showing benefit 96 99 100 101 , while the others reporting no benefit. 102 103 104 Zeng et al 99 studied 125 consecutive patients with positive TTT; they found that there was no recurrence of syncope in 72.6% of patients undergoing orthostatic training (OT), as against 36.1% in patients without any treatment, at 1-year follow-up and as against a placebo-controlled trial demonstrated a positive trend in terms of the benefit of home OT (20% vs 50%, P = 0.2) but it did not reach statistical significance level. 104 The contrasting results of the studies may be due to the non-uniformity of methods and variable compliance of the patients with tilt training.
The use of yoga for the treatment of RS has been recently studied in a randomized study by Shenthar et al. 105 The yoga module described in the trial consisted of warmup, asanas (yoga postures), pranayama (breathing exercises), dhyana (meditation), and deep relaxation technique with each session of 60 min at least 5 times/week for 12 months. At 12 months follow-up, there was a significant reduction in syncope recurrence in the yoga therapy group as against conventional conservative therapy (without yoga) (3.8 ± 3.2 episodes vs 1.1 ± 0.8, P < 0.001).
Fludrocortisone 106
These work by the mechanism: increasing renal sodium reabsorption ↓ expansion of plasma volume↓ reducing orthostatic component of the syncope
Alpha agonists—these act by peripheral vasoconstriction (increasing peripheral resistance).
Beta-blockers have been tried in the past for the treatment of RS, presumed to be acting by decreasing the ventricular mechanoreceptor activation by their negative inotropic effect. There was no benefit in the treatment of RS in the randomized trials. 107 108 Moreover, if the patient has underlying borderline or low heart rate, these may worsen the condition. The latest ESC guidelines have given class III indication for the use of beta-blockers in the treatment of RS. 3
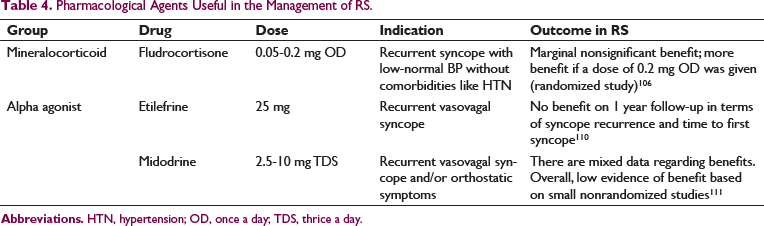
Pharmacological Agents Useful in the Management of RS.
A pacemaker may be indicated in a specific subset of the patients with RS. A small subset of patients has a predominant cardioinhibitory response (VASIS type 2 or ISSUE type 1 or 2) on TTT or long-term ECG monitoring (eg, ILR) with or without HS, which is common in the elderly population. 5 57 71 These patients may be treated with the conservative line of management, along with medications, at the initial presentation but may require additional treatment if 112 :
Recurrent symptoms are not responding to medications
Very short prodrome
Syncope during high-risk activities, for example, driving, machine operations, flying, etc.
The benefit of pacing in this particular subset is based on the rationale—pacing may be able to modulate RS episodes if acted sufficiently early at a rate higher than lower pacing rate and with atrioventricular (AV) sequential pacing. 113 Early studies have used cardioinhibitory response on TTT to decide on the need for pacing. 114 115 Few of the nonblinded studies were positive but the metanalysis by Sud et al 116 including both blinded and nonblinded studies found that there was no benefit of pacing based solely on TTT response and the benefit shown in nonblinded studies was an “expectation effect.” The most convincing evidence regarding this was provided by the ISSUE-3 study, in which all the patients had undergone ILR implantation and found that pacing in the patients with syncope with ≥3 s or without syncope with ≥ 6s pause reduced recurrent syncope over 2 years follow-up. 59
Since the earliest evidence of the usefulness of pacing in RS, it tried to use various specific algorithms which may help the patients with recurrent syncope like rate-drop response (RDR) algorithm and closed-loop-stimulation (CLS) pacing. 117 118 119 120 RDR algorithm detects a sudden decrease in heart rate and increases the rate of pacing so that the syncopal event can be avoided. The detection portion of the algorithm has a programmable “heart rate change-time duration” window which is helpful in the detection of imminent RS (based on decreasing heart rate) and triggers AV sequential pacing at a programmable rate. 117 In the ISSUE-3 study, all the patients receiving pacemakers had an RDR algorithm and it showed 57% relative risk reduction in syncope recurrence. 59 The main issue with the RDR algorithm is that it takes time to respond in an episode of RS. 121
CLS is the proprietary algorithm of Biotronik (Berlin, Germany), which detects right ventricular (RV) impedance as an indirect measure of RV contractility and uses it to counteract RS events. 122 RV lead constantly measures impedance, which is dependent on the amount of myocardium interfering with the lead tip. In diastole, there is maximum blood in RV so impedance is low. In contrast, in systole, when there is minimum blood pool in RV, the amount of myocardium interfering with lead tip is highest and so is the impedance. This high impedance triggers pacing at the CLS intervention rate (programmable). This beat-to-beat monitoring of RV impedance can detect inotropic changes early in an RS event. The response time is relatively fast for the CLS algorithm. 123 An elegant study has recently been done to evaluate the benefit of the CLS algorithm in 127 patients aged 40 years and older with at least 2 episodes of unpredictable severe syncope in last year and a systolic pause of >3 s induced by TTT. The syncope recurrence, at 11.2 months of median follow-up, was reduced by 77% with the use of the CLS algorithm (16% vs 53%, P = .00005) as compared to the control population (with ODO pacing mode). 120
The patients who have mixed or hypotensive responses on TTT (type 1/3) are suspected of having HS. 124 These patients may require the measures to counteract HS like discontinuation/reduction in hypotensive drugs, optimal salt/fluid intake, use of medications (eg, fludrocortisone/midodrine), and so on. 3
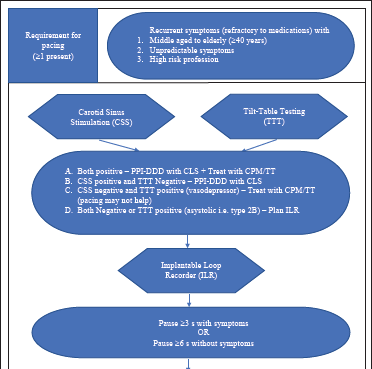
We propose an algorithm based on the European Society of Cardiology (ESC) guidelines to decide on pacing in patients with RS (Figure 3).
Common precipitants associated with syncope are micturition, gastrointestinal stimulation (swallowing and defecation), cough, sneeze, laughing, and so on. The easiest way to avoid these episodes is to educate the patient regarding the events and if possible avoid the specific situations which may induce symptoms, but it may not be possible always. In all these patients, the addition of salt and water in the diet, an inclination of the head end of the bed by 10 degrees, and avoiding a sudden change of posture may avoid precipitation of the symptoms. 125 For micturition syncope, patients are advised to do an intermittent voiding and avoid sudden bladder emptying of the bladder. 126 For gastrointestinal-related syncope and cough/sneeze-related syncope, the underlying cause of difficulty in swallowing/defecation has to be determined for the definitive management of the patient. 127 128
Low-adenosine syncope
Some patients affected with recurrent syncope have a very short duration prodrome (<5 s) with a structurally normal heart and normal ECG. This particular population has been found to have low plasma adenosine levels and is susceptible to even a small increase in adenosine, which may act on the A1 receptor located in the AV node and sinus node, which may lead to heart block. 129 The most common mode of presentation is paroxysmal AV block, some patients may present with symptomatic bradycardia. 130 In the recent case series of 16 patients, it was found that use of theophylline (adenosine receptor blocker) in this specific type of syncope helps in the reduction of syncope (2.6 syncope/year vs 0.4 syncope/year; P = .005) 131 132
b. Low-norepinephrine syncope
RS is associated with the sudden withdrawal of sympathetic activity and release of epinephrine from the adrenal medulla as a “fight” response. Similarly, in the nerve endings of the cardiac sympathetic nervous system (SNS), there is an increase in norepinephrine levels. 133 This is associated with increased serum levels of metabolic by-products of norepinephrine (ie, dihydroxy phenyl glycol or DHPG). 134 With the use of norepinephrine reuptake transporter inhibitors (ie, reboxetine, sibutramine), there is a decreased peripheral (adrenal medulla) adrenaline secretion, increased local norepinephrine concentration (in cardiac SNS), and decreased DHPG levels (indicating decreased degradation of norepinephrine). 135 This correction of the catecholamine milieu has been found to be beneficial in improving orthostatic tolerance in the patients presenting with recurrent syncope with a positive TTT (TTT duration 35 ± 1 min vs 29 ± 2 min, P = .001). 134 These medications are found to increase BP and HR in all the subjects due to locally increased norepinephrine concentration, hence it has been advised to be given to the patients with low baseline levels of norepinephrine. 3
c. Cardioneuroablation (CNA)
RS may be very rapid in some patients which may not provide enough time for the use of any other management modalities like counterpressure maneuvers or pacing to abort a particular episode. 136 Catheter ablation to attenuate vagal activity on sinus and AV node has evolved as one of the treatment modalities in a subgroup of patients not responsive to other treatments. 136 137 138 This technique of treatment of bradyarrhythmia is termed CNA. In this technique, ganglionated plexi (GPs) are targeted systematically—left-sided plexi first, aorto-superior vena cava (Ao-SVC) GP (for tackling atrial vagal innervations), posteromedial left GP (in case of AV block as the presenting feature), and an additional right-sided ablation if left-sided ablation was not sufficient. 138 This has recently been compared with conventional management without the use of CNA in the propensity-matched patient subset (recurrent syncope with VASIS-type 2B response or >3 s asystole), which showed that CNA caused a significant reduction in syncope recurrence (4-year syncope free rate—CNA: 0.86 vs conventional therapy: 0.50). 139 Also, the same group has recently shown that CNA reduces QTc through neuromodulation which is not noted in the patients treated with pacemaker implantation for RS. 140
Concluding Remarks
Syncope needs meticulous evaluation on the part of the physician. The diagnosis of RS centers around the history and examination of the episode. The other diagnostic modalities can help in the confirmation of the diagnosis and in deciding the treatment of the condition. The management of RS may be conservative if the episodes are infrequent or may require additional management in case of recurrence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.