
Abstract

Introduction
A 55-year-old male presented with an episode of syncope. There was no history of breathlessness, angina, or palpitation. Clinical examination was unremarkable. He was admitted for evaluation of syncope. Electrocardiogram was done which revealed ST segment elevation in leads II, III, augmented vector right (aVF); ST segment depression in leads augmented vector left (aVL), aVR, and bizarre T waves in leads aVL, aVR, and V1. However, patient was asymptomatic at this point of time. Echocardiography did not reveal any regional wall motion abnormality. Electrocardiogram (ECG) was repeated after a couple of minutes which was normal (Figure 1). The repeat ECG was done by making sure the electrode is not placed over the artery.
(A) Electrocardiogram showing ST segment elevations and bizarre T waves. (B) ST-T changes disappear in the subsequent electrocardiogram.
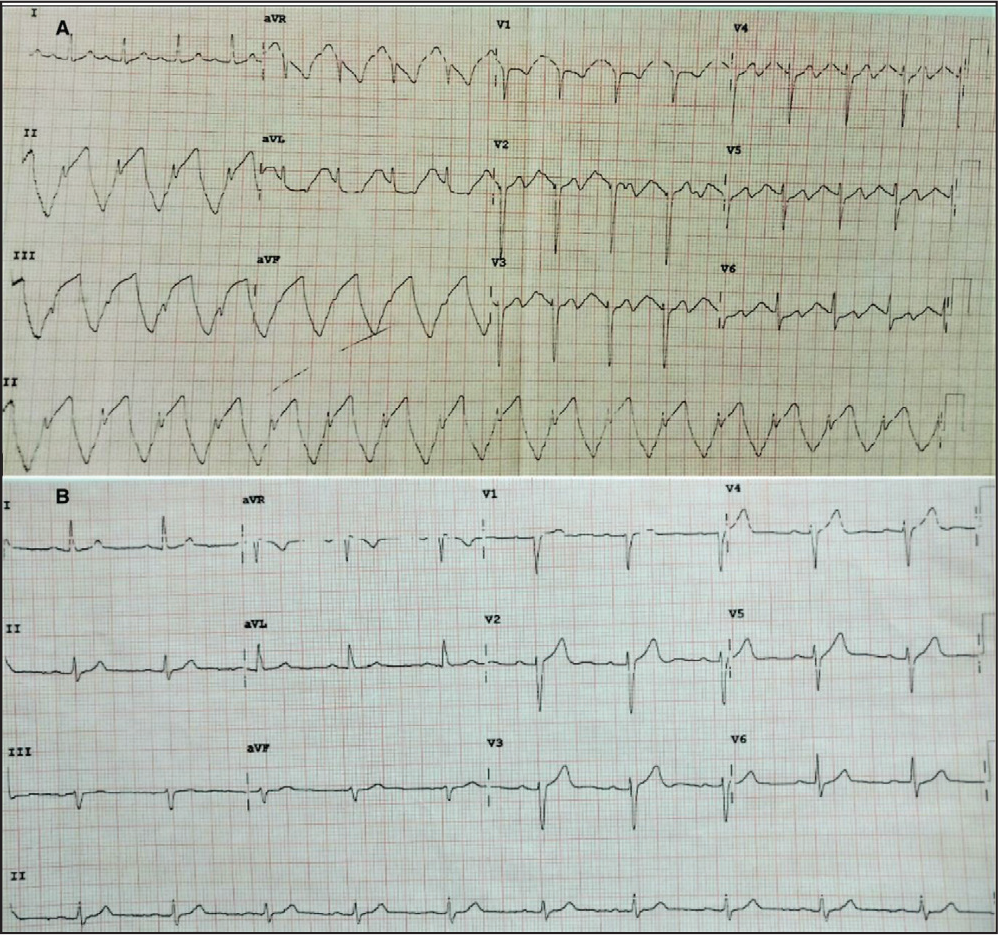
The differential diagnoses of ST segment elevation are myocardial infarction, early repolarization, left ventricular hypertrophy, left bundle branch block, acute pericarditis, hyperkalemia, Brugada syndrome, and pulmonary embolism. Seldom ECG artifacts can also masquerade as ST segment elevation. In our case, though there were ST segment changes in the ECG, patient was asymptomatic and the changes disappeared in the subsequent ECG. ST segment elevation was seen in the inferior leads, but there was no corresponding reciprocal ST segment depression. These features were not suggestive of myocardial ischemia. Moreover, the ST segment changes here were beginning at the onset of QRS complex and T wave morphology was bizarre, which goes in favor of an artifact. The coupling interval of the QRS complex and the artifact is identical, which signifies that the artifact is synchronous with cardiac cycle. Hence, the artifact in unlikely to be from any external source. This phenomenon occurs due to tapping of arterial pulse on the ECG electrodes, which is known as arterial pulse tapping artifact. Such bizarre ECG changes were first reported by Ozhan et al 1 in a post-percutaneous coronary intervention patient, which he initially attributed to silent ischemia. However, it was Aslanger and Bjerregaard 2 who described that the mechanism of those ECG changes was indeed due to arterial pulse. In the given ECG, ST segment changes were seen in all limb leads except lead I, the only lead which does not utilize left lower limb electrode. This suggests that the artifact arose from left lower limb electrode, probably due to posterior tibial artery pulsations. Lead V1 also showed changes because in precordial leads Wilson central terminal is produced by connecting negative pole of limb electrodes. 3 Pulse tapping artifacts are being reported in patients with large volume pulse like in arteriovenous fistula for dialysis. But such artifacts are rarely reported in patients with normal pulse. We had ruled out conditions which lead to hyperdynamic circulation like anemia, hyperthyroidism, valvular regurgitation, and patent ductus arteriosus. We hypothesize that the artifact might have been produced as a result of increased amplitude of the pulse consequent to sympathetic stimulation, since the ECG was done just after patient returned from rest room. Recognizing such intimidating ECG artifacts is very important to avoid unnecessary interventions in a benign condition, at the same time being vigilant to pick up such life-threatening conditions.