
Abstract
We present a bizarre electrocardiogram that needs critical evaluation to avoid unnecessary investigations.
Clinical Vignette
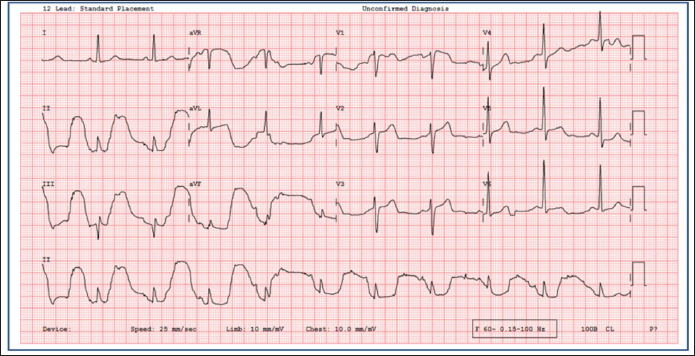
A man in his 70s presented to the emergency room with functional class II dyspnea without angina. In the past, he had an angioplasty to fix a block in the right coronary artery. A follow-up angiogram two years ago had confirmed a patent stent and non-significant disease in the left coronary artery. He was evaluated and noted to have a bizarre electrocardiogram (ECG) (Figure 1). What is the likely etiology and mechanism(s) involved in the case?
A 12-lead Electrocardiogram of the Patient.
Discussion and Explanation
There were abnormally large apparent positive T waves and minimal ST segment elevation in inferior leads (II, III, aVF), negative T waves in aVR, and aVL with biphasic T in lead V1 (Figure 1). However, there were no such changes in lead I. On careful inspection, normal T wave deflections could be seen in the second complex of leads II and III (Figure 1). This, along with the fixed coupling with the R wave, also indicates that it is an artifact related to the cardiac cycle. This phenomenon is called an arterial pulse-tapping artifact caused by arterial pulse hitting the ECG electrode. Similar ECG changes had been inadvertently attributed to coronary ischemia in the past. 1 Later, it was found to be an arterial pulse-tapping artifact. 2
In our case, a T-wave abnormality was noted in all limb leads except lead I, which gave clues about the etiology. Lead I does not utilize the left lower limb electrode (Figures 1 and 2). Thus, it confirmed the artifact’s origin in the left lower limb, probably from the left posterior tibial artery. Precordial leads also showed minimal changes as they used the Wilson central terminal, formed by connecting the negative poles of limb electrodes (Figure 2). After the first four beats in the ECG, there was a change in the artifact morphology, probably because of the displacement of the electrode from the artery during the movement of the same limb. Arterial pulse-tapping artifacts are usually associated with hyperdynamic circulation. However, we ruled out arteriovenous fistula, anemia, hyperthyroidism, aortic regurgitation, and patent ductus arteriosus.
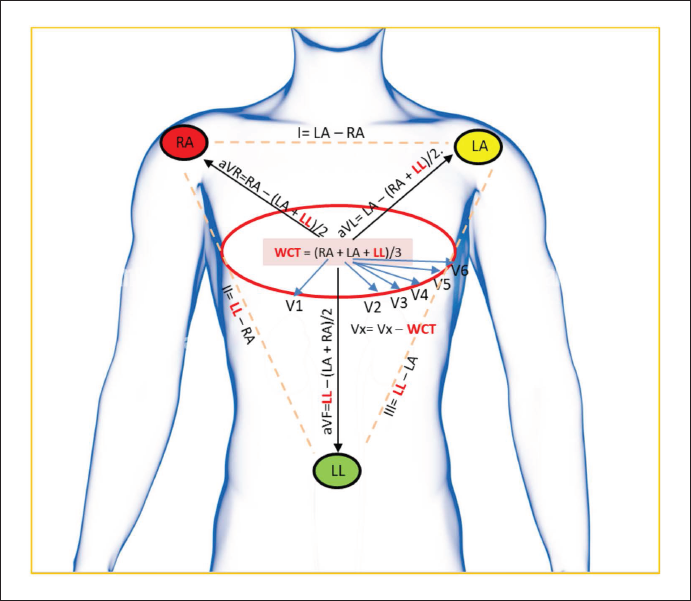
It is imperative to note that the affection of leads other than limb leads and aVF is lesser due to the contribution of the abnormal lead being divided by denominators in the formula (note the formulas in Figure 2). This explains the minimal affection of aVR and aVL (compared to aVF) and other precordial leads (further lower because of the denominator being 3).
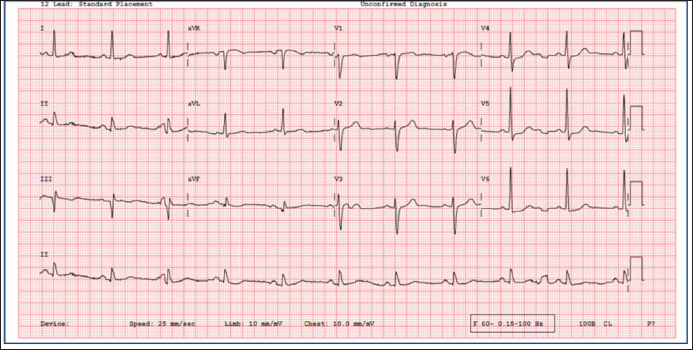
A repeat ECG taken with electrode locations slightly distant from the previous location showed a normal ECG with baseline wander (Figure 3). Echocardiography did not show any new wall motion abnormalities. This case illustrates that recognizing ECG artifacts may help avoid unnecessary investigations.
Bizarre ST-T Changes Disappear in the Electrocardiogram Conducted.
Informed Consent
Obtained from the patient in line with COPE guidance.
Author Contribution
SM (conceptualization: lead; formal analysis: lead; writing – original draft: lead; writing – review and editing: lead); DPR (writing – review & editing: equal); JV (writing – review and editing: equal).
Data Availability Statement
All data are incorporated into the article and its online supplementary material.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as it is an anonymous case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.